Complete Heart Block in Pregnancy: A Report of Emergency Caesarean Section in a Parturient without Pacemaker
Vandana Mohapatra1, Aparajita Panda2, Satyanarayan Behera3, Jagadish Chandra Behera4
1 Senior Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences (AIIMS), Bhubaneswar, Odisha, India.
2 Assistant Professor, Department of Anaesthesiology, All India Institute of Medical Sciences (AIIMS), Bhubaneswar, Odisha, India.
3 Senior Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences (AIIMS), Bhubaneswar, Odisha, India.
4 Senior Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences (AIIMS), Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vandana Mohapatra, Senior Resident, Department of Obstetrics and Gynaecology, AIIMS Bhubaneswar-751019, Odisha, India.
E-mail: mohapatravandana@yahoo.in
Management of women with Complete Heart Block (CHB) presenting without pacing, during pregnancy and labour is debatable. Temporary pacemakers have been routinely inserted for labour and birth probably to withstand any haemodynamic variations. However, due to lack of large scale prospective studies, the necessity of this procedure has not been objectively assessed. Also, the most appropriate anaesthetic technique for caesarean section in women with CHB is yet to be clarified. We report herein the case of a pregnant woman with CHB who had uneventful emergency caesarean delivery under spinal anaesthesia without temporary pacing. She was an unbooked case detected with congenital CHB first time during active labour; echocardiography showed no structural cardiac disease and her heart rate increased with atropine. We suggest further research so that guidelines could be established to prevent unnecessary morbidity and expense of temporary pacemaker insertion. Newly diagnosed cases of asymptomatic CHB in late pregnancy should be worked up for chronotropic responsiveness using atropine and responsive cases may be managed without pacemaker.
Haemodynamic variations, Maternal complete heart block, Temporary pacing
Case Report
A 26-year-old, gravida 2 abortion 1, unbooked case, presented to the labour ward at 36+5 weeks gestational age in active labour. Two years back, she had an induced abortion at 6 weeks of gestation by medical methods. During her present pregnancy, she had irregular antenatal check ups at a local hospital with no follow-up in the third trimester. She had no known history of any medical illnesses, drug intake or addiction. On examination, her pulse rate was 42/minute, while blood pressure was 110/80 mmHg. Cardio-respiratory system examination was unremarkable. Obstetric examination revealed term size uterus with fetus in longitudinal lie and cephalic presentation. There were regular uterine contractions, fetal heart rate was 140 beats/minute. On per vaginal examination, cervix was fully effaced, os was 4 centimetres dilated, vertex station was at -2 and membranes were intact.
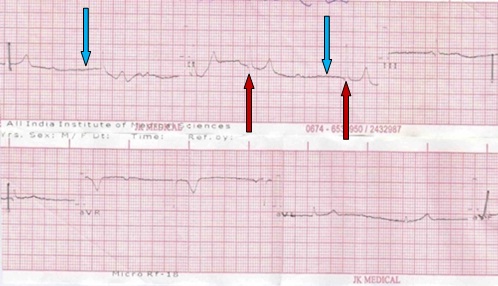
Cardiologist’s opinion was sought in view of persistent bradycardia. Electrocardiogram (ECG) was done which showed sinus bradycardia with narrow QRS complexes suggestive of congenital Complete Heart Block (CHB) [Table/Fig-1]. Echocardiography was normal. Routine blood investigations were within normal limit. Pulse rate settled to 70-76/minute with intravenous injection atropine. Plan was to proceed with temporary pacing if heart rate did not increase after injection atropine or any deterioration in haemodynamic status occurred.
Electrocardiogram showing sinus bradycardia (heart rate - 38/min) with narrow QRS complexes (red arrow) and junctional escape rhythm (blue arrow) suggestive of congenital complete heart block.
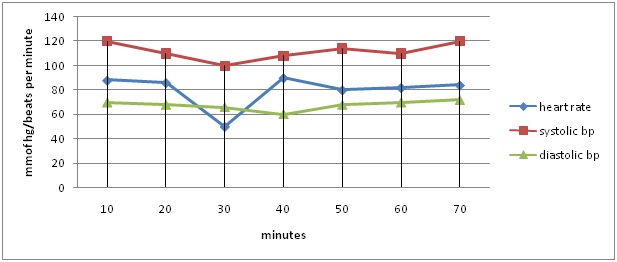
Labour was augmented with injection oxytocin. In the meantime, thick meconium stained liquor was detected on artificial rupture of membranes and cardiotocograph showed non-reassuring fetal heart rate pattern. The woman was taken up for caesarean section under emergent conditions without temporary pacing. However, injection isoprenaline and temporary pacemaker was kept on standby. She was preloaded with 750 mililitres of Ringer’s lactate solution prior to spinal anaesthesia. Two mililitres of hyperbaric 0.5% Bupivacaine was injected into subarachnoid space at L3-L4 level with the woman in left lateral position. A sensory level upto T8 was achieved. A late preterm vigorous male baby with birth weight of 2400 grams (appropriate for date) was delivered. The average estimated total blood loss was approximately 600 mililitres. Monitoring included continuous ECG, pulse oximeter and both invasive and noninvasive blood pressure. During surgery, heart rate dipped to 50/minute once; it responded to atropine [Table/Fig-2]. Intraoperative haemodynamics remained stable and surgery proceeded uneventfully.
Intraoperative haemodynamics during caesarean section; BP in mmHg.
Postoperatively, continuous monitoring was done with pulse oximeter and invasive blood pressure. The woman’s heart rate remained steady at 54-64 beats/minute. Analgesia was achieved with injection diclofenac 75mg intravenous 8th hourly. Postpartum period was uneventful; she was discharged on the seventh postoperative day. The neonate did not have any rhythm disturbance. She was doing well on follow up at 6 weeks. She was prescribed progesterone only pill (desogestrel 75μg) for 3 months and advised to continue follow-up in cardiology. During the present pregnancy, the entire period of hospital stay and on follow-up, the woman never had symptoms of CHB.
Discussion
CHB detected for the first time during pregnancy and delivery is rare [1]. It is a disorder of the cardiac conduction system with complete absence of atrioventricular conduction. The first case of CHB in pregnancy was reported by Nanta in 1914 [2]. It may be congenital or acquired secondary to cardiac surgery, rheumatic heart disease or infective disorders. Isolated congenital CHB is relatively benign with narrow QRS complexes on ECG, and heart rate may increase with atropine or sympathomimetics [3]. Prognosis in acquired heart block is generally worse. Our case was detected with congenital CHB.
Fetomaternal outcome is favourable in asymptomatic cases and in uncomplicated bradyarrhythmias without significant underlying heart disease [1,4]. Rarely preterm birth and intrauterine growth restriction has been observed. Few asymptomatic women without pacemakers may present with sudden cardiac death or heart failure during pregnancy, or may become symptomatic during labour due to valsalva induced bradycardia [5]. Contrary to this, some authors observed no significant bradyarrhythmia during labour and delivery, which they attributed to increased sympathetic response at this stage or high uptake of regional anaesthesia [6]. However, antenatal care warrants close surveillance by interdisciplinary teams. Vaginal delivery is not contraindicated. Caesarean section is reserved for obstetric reasons and in those with intractable heart failure.
In women without a permanent pacemaker, temporary pacemakers have been routinely inserted for labour and birth probably to withstand any haemodynamic variations [7]. However, the requirement of temporary pacing during labour and the accurate timing or rate setting of pacemaker has not been objectively evaluated [4]. Hidaka et al., recently outlined that most women with complete atrioventricular block who are asymptomatic and do not require a permanent pacemaker before delivery, can be safely managed during labor without pacing [5]. A pacemaker is indicated in the presence of symptoms (chest pain, dyspnea, syncope, palpitations), Q-T interval prolongation, wide QRS complex, ventricular dysfunction, or heart failure [8]. Permanent pacemakers are implanted at any stage of pregnancy whereas short-term temporary pacing is done during delivery.
Operative delivery particularly, has been considered therapeutically challenging as hemodynamic instability is anticipated in presence of CHB [9]. Mothers with congenital CHB have undergone caesarean delivery both with and without temporary pacing in the past. However, isolated case reports have precluded formulation of specific guidelines for perioperative management. A primigravida with triplet pregnancy and CHB underwent uncomplicated caesarean section without pacing [10]. Intraoperative haemody-namics remained stable in an asymptomatic case, and did not require pacemaker activation even when significant blood loss was encountered [9]. Asymptomatic women who responded to exercise or atropine by an increase in heart rate were managed without pacemaker [3,11]. Our case responded to atropine and had an uneventful caesarean delivery without temporary pacing.
Review of cases revealed that whilst facilities for temporary pacemaker insertion were extremely valuable, many asymptomatic women who were treated probably did not require pacing. This insertion is also not risk free. Complications such as irradiation, bleeding, infection or embolism are common. Temporary pacemakers may malfunction unexpectedly, leading to sudden hemodynamic instability [12]. Guidelines should be established to prevent unnecessary morbidity and expense of the procedure.
There are no specific recommendations as regards the most appropriate anaesthetic technique for caesarean section in women with CHB. Studies suggested that regional anaesthesia is safe in pregnant women with cardiac disease undergoing caesarean section [8,13]. Although the risk of hypotension is less with epidural technique, it may not be suitable in emergent situations with time constraints. Haemodynamic stability can be obtained by titrated regional anaesthesia, intravenous volume, and phenylephrine infusion guided by continuous invasive monitoring [13]. We encountered no intraoperative haemodynamic instability under spinal anaesthesia probably due to adequate preloading.
Conclusion
Women with asymptomatic CHB can present at the time of labour and pose a challenge to the obstetricians. Furthermore, there are no protocols for perioperative management during caesarean section due to rarity of the disease. As suggested by our case, caesarean delivery might be safely contemplated without temporary pacing in asymptomatic women with CHB who demonstrate chronotropic responsiveness to atropine. Nevertheless, close monitoring, multidisciplinary approach with facilities for temporary pacing, and follow-up of symptoms and cardiac function is warranted in these pregnant women during labour and perioperative period.
[1]. Suri V, Keepanasseril A, Aggarwal N, Vijayvergiya R, Chopra S, Rohilla M, Maternal complete heart block in pregnancy: analysis of four cases and review of managementJ Obstet Gynaecol Res 2009 35(3):434-37. [Google Scholar]
[2]. Jaffe R, Gruber A, Fejgin M, Altaras M, Ben-Aderet N, Pregnancy with an artificial pacemakerObstet Gynecol Surv 1987 42(3):137-39. [Google Scholar]
[3]. Kumar AU, Sripriya R, Parthasarathy S, Ganesh B A, Ravishankar M, Congenital complete heart block and spinal anaesthesia for caesarean sectionIndian J Anaesth 2012 56(1):72-4. [Google Scholar]
[4]. Keepanasseril A, Maurya DK, Suriya JY, Selvaraj R, Complete atrioventricular block in pregnancy: report of seven pregnancies in a patient without pacemakerBMJ Case Reports 2015 doi:10.1136/bcr-2014-208618; Available from:casereports.bmj.com accessed on 10th February 2016 [Google Scholar]
[5]. Hidaka N, Chiba Y, Fukushima K, Wake N, Pregnant women with complete atrioventricular block: perinatal risks and review of managementPacing Clin Electrophysiol 2011 34(9):1161-76. [Google Scholar]
[6]. Thaman R, Curtis S, Faganello G, Szantho GV, Turner MS, Trinder J, Cardiac outcome of pregnancy in women with a pacemaker and women with untreated atrioventricular conduction blockEuropace 2011 13:859-63. [Google Scholar]
[7]. Hidaka N, Chiba Y, Kurita T, Satoh S, Nakano H, Is intrapartum temporary pacing required for women with complete atrioventricular block? An analysis of seven casesInt J Obstet Gynaecol 2006 113:605-07. [Google Scholar]
[8]. Chohan U, Afshan G, Mone A, Anaesthesia for caesarean section in patients with cardiac diseaseJ Pak Med Assoc 2006 56(1):32-38. [Google Scholar]
[9]. Rai V, Shariffuddin II, Chan YK, Muniandy RK, Wong KK, Singh S, Peri-operative management of hysterostomy in a parturient with complete heart block, placenta accreta and intrauterine deathBMC Anesthesiology 2014 14:49 [Google Scholar]
[10]. Awasthi K, Gupta S, Awasthi G, An unusual case of complete heart block with triplet pregnancyIndian Heart J 2003 55:641-42. [Google Scholar]
[11]. Modi MP, Butala B, Shah VR, Anaesthetic management of an unusual case of complete heart block for LSCSIndian J Anaesth 2006 50(1):43-44. [Google Scholar]
[12]. Ganjoo P, Navkar DV, Tandon MS, Complete heart block complicating intracranial aneurysm surgery in a pregnant patientNeurol India 2010 58(1):146 [Google Scholar]
[13]. Langesaeter E, Dragsund M, Rosseland LA, Regional anaesthesia for a caesarean section in women with cardiac disease: a prospective studyActa Anaesthesiol Scand 2010 54(1):46-54. [Google Scholar]