Abnormal Course of Right Coronary Artery Together with Variant Left Coronary Artery and Partial Atresia of Cicumflex Artery
Rajani Singh1
1 Additional Professor, Department of Anatomy, AIIMS, Rishikesh, Uttarakhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajani Singh, Additional Professor, AIIMS Rishikesh Virbhadra Marg Pashulok, Rishikesh-249203, Uttarakhand, India.
E-mail: nani_sahayal@rediffmail.com
Heart is supplied by right and left coronary arteries. Therefore, the knowledge of normal and variant anatomy of both these arteries and their configurations is indispensable for proper understanding of diagnosis and treatment of dreaded cardiac diseases.
During routine cadaveric dissection, a heart of an adult female with anomalous course of Right Coronary Artery (RCA), new variant of trifurcated Left Coronary Artery (LCA) and partial atresia of circumflex (CX) artery was detected. Trifurcation of LCA into anterior interventricular, CX and a ramus intermedius without giving accessory branches has been reported. But in the present case, a variant trifurcation was found having rare configuration i.e., the interventricular branch gave two additional branches, a new variant along with ramus intermedius also giving an additional branch another new variant followed by partially hypoplastic circumflex artery. Besides this, RCA has an aberrant course modifying normal supply of heart. This rare configuration of coronary arteries will facilitate the cardiac surgeons to improve the understanding of defects of coronary arteries and planning of angiography, coronary by bypass grafting and other surgical interventions, radiologists for refining interpretation of imagery and anatomists for new variants.
Cardiac diseases, Surgical interventions, Trifurcation
Case Report
During routine cadaveric dissection, a heart of an adult female cadaver was detected having rare variant of trifurcation of Left Coronary Artery (LCA) associated with anomalous course of Right Coronary Artery (RCA). The LCA immediately after originating from posterior left coronary sinus travelling about 1mm from ascending aorta underwent variant trifurcation giving rise to three branches namely: 1) Anterior Interventricular (AI) artery; 2) Ramus Intermedius (RI) artery; 3) Circumflex (CX) artery [Table/Fig-1].
Showing trifurcation of left coronary artery.
AA- Asending aorta, RCA- Right coronary artery, LCA- left coronary artery, RI- ramus intermedius, CX- circumflex artery, AIV- anterior interventricular artery, DI- diagonal artery.
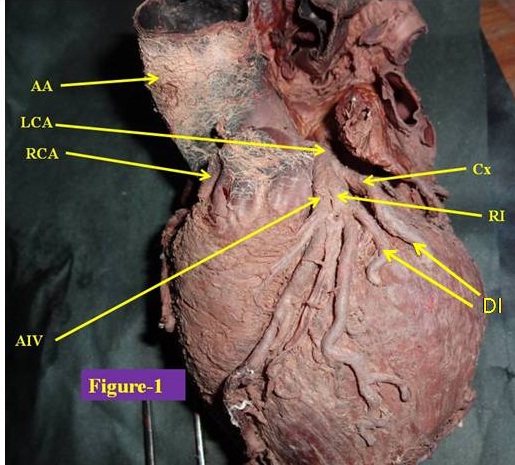
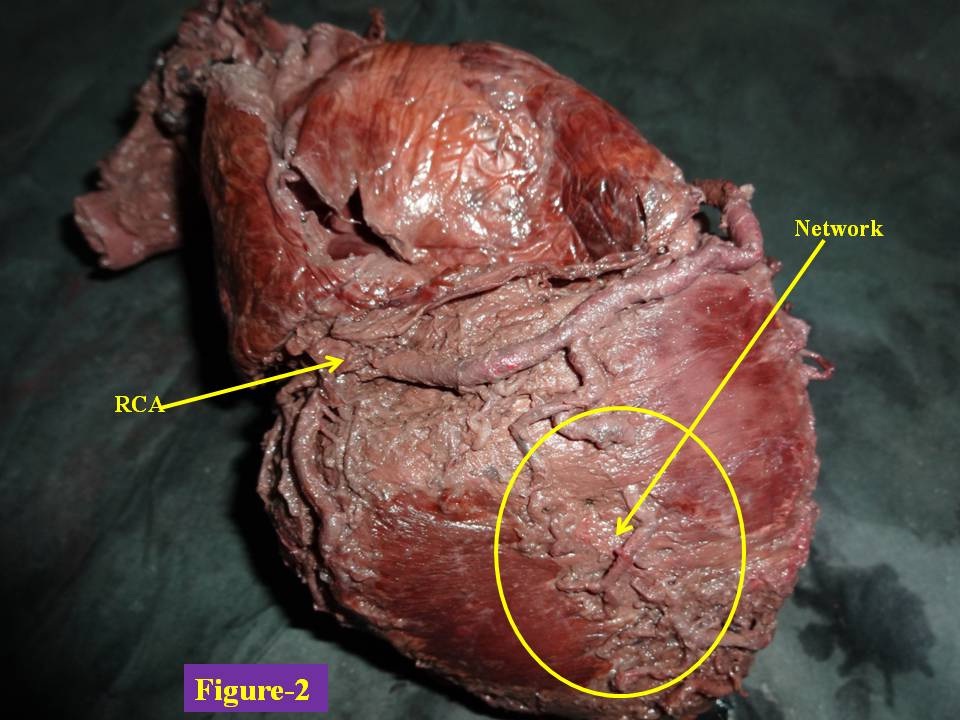
Anterior Interventricular Artery (AI), arising from main trunk, gave two ventricular arteries with main branch continuing further. All the three branches of AI supplied left ventricle (anterior wall). Main AI crossed the inferior border and ended there instead of advancing further to the inferior surface for anastomising with posterior interventricular artery as in the normal case. This is a rare variant of AI and its length too was found short. Posterior interventricular artery was absent and replaced by network of small vessels from RCA and AI [Table/Fig-2].
Showing abnormal course of right coronary artery.
RCA- right coronary artery, Network- network formed by branches from RCA and anterior interventricular artery.
CX artery had very short course in left coronary sulcus and ended there by giving branches to supply left ventricle without crossing the left border of the heart. RI is present between AI and CX artery. After originating, it bifurcates providing main branch and a new branch which is abnormal. This is also new variant.
RCA has classical course as described in standard text books from beginning up to right posterior coronary sulcus. It gave all normal branches viz., conus branch, anterior arterial branch, anterior ventricular branch and right marginal artery. Thereafter, normally it ends up by anastomising with CX artery but in the present case, it continued in the left posterior coronary sulcus and ended near left border of heart giving branches to supply left ventricle without crossing the left border [Table/Fig-2]. Its extended course follows the path and function of the LCA. There was no abnormality in the branching pattern of RCA.
Discussion
Trifurcation and quadrifurcation of LCA have been documented in the literature [1–4]. Baptista et al., found trifurcation of LCA in 38.7% of cases [1]. Trifurcation of LCA in this case after originating from aorta ran for 1 mm and then trifurcated into AI, RI and CX artery whereas the trifurcation of LCA into AI branch, CX branch and RI without giving accessory branches was also reported by Ballesteros and Ramirez [5]. But in the present case, the trifurcation is a new variation by the fact that the interventricular branch gave two additional branches along with ramus intermedius also giving an additional branch (diagonal artery) which supplied the left surface of left ventricle followed by partially hypoplastic CX artery. The length of LCA under current study is short measuring 1mm. But a short main trunk of LCA poses problems in carrying out coronary angiography because when catheter is inserted into one of the terminal branches, the opacification of the other branch does not occur and an incomplete image of the coronary tree is seen [6]. Hence, short LCA in the present case may cause misinterpretation of coronary angiography.
An unusual gross variation nurtures interest of anatomists and causes concern for clinicians when it mimics pathology. So these anomalies may mislead the anatomists, radiologists and clinicians. These may create many clinical complications which are detailed below-
1. The effects of variant anatomy of RCA and LCA-
a) In the absence of knowledge of the variant, defect in extended RCA course the radiologist and clinician may be misled with the defect in LCA in place of RCA. Lot of confusion may arise due to this variation to an anatomist academically.
b) Interventicular artery immediately after emergence gave out two branches. This is another variant but it may cause increased perfusion of anterior wall of left ventricle.
c) Main interventricular artery was short and posterior interventricular artery was absent. There may be inadequate supply to the inferior surface of heart due to above mentioned anomaly. But in this case it is compensated to some extent by network formed by branches from this artery and RCA.
d) CX artery had very short course in left coronary sulcus so there is partial atresia of CX artery. The area supplied by CX artery normally is supplied by RCA in this case.
e) RI gave a new branch. This is an unusual variant.
Thus, if there is any complication in the supply or defect in the areas pertaining to above six anomalies, the diagnosis may be misinterpreted. In such cases, if these variations are not kept in mind then heart diseases due to abnormal RCA and absence of posterior interventricular artery may be attributed to CX artery and posterior interventricular artery. In presence of such variation, difficulties may occur in the diagnostic procedures, resulting in failure cases. Therefore, identification of the anomaly is essential for proper management of cardiac diseases, especially in patients undergoing evaluation for percutaneous coronary intervention, coronary artery surgery or prosthetic valve replacement [6].
Conclusion
Thus, the above mentioned variations are of utmost use to the cardiac surgeon in diagnosing and treating cardiac ailments, radiologists in avoiding misinterpretation and to anatomists for new variation.
[1]. Baptista CAC, Di Dio LJA, Prates JC, Types of division of the left coronary artery and the ramus diagonalis of the human heartJapanese Heart Journal 1991 32(3):323-35. [Google Scholar]
[2]. Cavalcanti JS, Anatomic variations of the coronary arteriesArquivos Brasileiros de Cardiologia 1995 65(6):489-92. [Google Scholar]
[3]. Reig J, Petit M, Main trunk of the left coronary artery: anatomic study of the parameters of clinical interestClinical Anatomy 2004 17(1):6-13. [Google Scholar]
[4]. Hirak D, Termination of left coronary in the population of AssamNational Journal of Basic Medical Sciences 2005 1(3):145-48. [Google Scholar]
[5]. Ballesteros LE, Ramirez LM, Morphological expression of the left coronary artery: a direct anatomical studyFolia Morphol 2008 67(2):135-42. [Google Scholar]
[6]. Dombe DD, Anitha T, Giri PA, Dombe SD, Ambiye MV, Clinically relevant morphometric analysis of left coronary arteryInt J Biol Med Res 2012 3(1):1327-30. [Google Scholar]