Nevus Lipomatosus Cutaneous Superficialis - A Rare Hamartoma: Report of Two Cases
Mayank Goyal1, Vaishali Hainath Wankhade2, Jayesh Ishwardas Mukhi3, Rajesh Pratap Singh4
1 Resident, Department of Dermatology, Venereology and Leprology, Government Medical College, Nagpur, Maharashtra, India.
2 Associate Professor, Department of Dermatology, Venereology and Leprology, Government Medical College, Nagpur, Maharashtra, India.
3 Associate Professor, Department of Dermatology, Venereology and Leprology, Government Medical College, Nagpur, Maharashtra, India.
4 Professor and Head, Department of Dermatology, Venereology and Leprology, Government Medical College, Nagpur, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mayank Goyal, 59, Basant Vihar Special, Opposite Blood Bank, Kota-324009, Rajasthan, India.
E-mail: mayank.kem@gmail.com
Nevus Lipomatosus Cutaneous Superficialis (NLCS) is a rare benign hamartomatous disorder in which mature collection of adipocytes are present ectopically in the dermis. NLCS usually presents as multiple, soft, pedunculated, cerebriform, yellowish or skin colored papules, nodules, or plaques, mostly involving the pelvic or gluteal region. We herewith report two cases of adult onset classical NLCS. First case had a classical presentation with lesion on lower back while second case was associated with some unusual features like occurrence on pubic area and associated comedo-like lesions.
Atypical, Comedo like lesions, Papules
Case Report
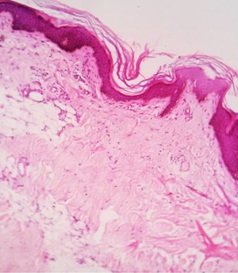
Case 1: A 40-years-old female presented with asymptomatic growth on lower back which had gradually increased to the present size over a period of 25 years. There were no systemic complaints. Family history of similar lesions was absent. Cutaneous examination revealed multiple soft, skin colored to hyperpigmented, non tender, smooth surfaced, coalescing papules and cerebriform plaques situated on the right lower back [Table/Fig-1]. There was no ulceration, discharge, associated excessive hair growth, comedo like plugs or cafe-au-lait spots. Biopsy from the papule revealed islands of mature adipose tissue in the dermis [Table/Fig-2]. Based on the clinical and histopathological findings diagnosis of nevus lipomatosus cutaneous superficialis was confirmed. Patient was referred to plastic surgery department for further management.
Well defined skin colored nodules and plaques with cerebriform surface on the lower back.

Mature adipose tissue seen in the superficial dermis with ovelying epidermis showing papillomatosis and increased pigment (H&E 40X).
Case 2: A 38-years-old female presented to dermatology department with multiple swellings over the pubic area. The lesions had started as a small cutaneous mass when she was 10-years-old. Lesions had increased slowly in number and size. Past family and medical history were not significant. There was no history of irritation or minor trauma. She had no systemic complaints. Dermatological examination revealed multiple, soft, non-tender, sessile, cerebriform, skin colored and hyperpigmented nodules and plaques [Table/Fig-3] with multiple, discrete open comedones at few places [Table/Fig-4]. Examination of the scalp, hair, nails and mucous membranes were normal. There were no systemic abnormalities. Routine laboratory investigations were normal.
Cerebriform plaques on pubic area.

Surface of plaque studded with multiple open comedones.

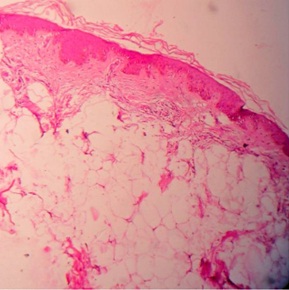
Histopathological examination revealed dermis replaced by islands of mature adipose tissue [Table/Fig-5]. Clinicopathological correlation suggested a diagnosis of NLCS. The patient was referred to the plastic surgery department for surgical management.
Histopathology showing normal epidermis with islands of mature adipocytes in epidermis (H&E 40X).
Discussion
NLCS, first described by Hoffman and Zurhelle in 1921, is a rare hamartomatous condition which is characterised by the presence of mature adipose tissue in dermis [1]. Clinically, NLCS is classified as classical or solitary type. The classical form is characterized by asymptomatic groups of soft, fleshy, skin-colored to yellow papules or nodules, often coalescing into plaques whose surface may be smooth, wrinkled or have a peau d’orange appearance [2]. There is no observed sexual or familial trend. The classical form of NLCS may be present at birth or develops during first two decades of life. The lesions have a predilection for the pelvic girdle, being seen most commonly on gluteal region, lower back, and upper thighs [2]. Lesions have also been reported less frequently at other sites including neck [3], perianal area [4], nose [5], groin [6] and pinna [7]. Das et al., reported a case of huge NLCS presenting as multiple swellings on scapular region and lower back [8]. Co-existent anomalies reported are trichofolliculoma of lower leg [9] and deep penetration nevus [10]. This form of NLCS may sometime be associated with hypertrichosis, comedo-like plugs, cafe-au-lait or hypopigmented macules, ulceration and foul smelling discharge [11].
The second form of NLCS comprises a solitary, domed or sessile papule, which develops in adult life, and has been reported at sites other than lower trunk, including the knee, axilla, arm, ear and scalp [11].
Histopathology reveals acanthosis, hyperkeratosis and increased pigmentation of the epidermis. There is presence of multiple mature fat lobules distributed irregularly throughout the dermis extending below till the junction between dermis and hypodermis and above till papillary dermis [12].
Exact pathogenesis is not known. But since the electron microscopy shows the presence of lipocytesin in close association with the capillaries, it has been suggested that they may originate from the pericytes, as in fetal lipogenesis [13]. Recently mosaicism for a 2p24 deletion was found in NLCS [11].
Differentials include lipofibromas, Goltz’s syndrome, and giant acrochordons. Histopathological evaluation usually helps in differentiation. The pedunculated appearance, later onset in life, fat content without skin appendages help to distinguish lipofibroma from NLCS. Goltz’s syndrome is characterized by the absence of collagen and associated underlying deformities and no fat cells are present in the dermis in case of skin tags [4].
As it is a benign condition with no systemic abnormalities or malignant changes, treatment is usually advocated only for cosmetic reasons. In most of the cases simple surgical excision is enough. However, if it is not adequate, recurrence is a possibility. Recently, CO2 laser treatment is reported as an effective modality without recurrence for large lesion. Staged surgical excisions and covering with local advancement flaps is another treatment modality which has been tried with good success [14].
Our first patient had the classical form of this uncommon condition while our second case had NLCS situated at an atypical site and was associated with comedo like plugs on the lesion which is a rare clinical feature of NLCS.
Conclusion
NLCS is a rare cutaneous hamartomatous condition, commonly occurring on lumbosacral area. However, occasionally physicians may encounter lesions with variable morphology and involvement of atypical sites.
[1]. Hoffmann E, Zurhelle E, Ubereinen nevus lipomatodes cutaneous superficialis der linkenglutaalgegendArch Dermatol Syph 1921 130:327-33. [Google Scholar]
[2]. Velaskar S, Nevi and Other Developmental defects. In: Sacchidanand S., Oberai C., Inamadar A., editorsIADVL textbook of dermatology 2015 4th edMumbaiBhalani Publishing House:286-344. [Google Scholar]
[3]. Das JK, Sengupta S, Gangopadhyay AK, Nevus lipomatosus superficialis over neck, an atypical siteIndian J Dermatol Venereol Leprol 2006 72:66-67. [Google Scholar]
[4]. Dhamija A, Meherda A, D’Souza P, Meena RS, Nevus lipomatosus cutaneous superficialis: An unusual presentationIndian Dermatol Online J 2012 3(3):196-98. [Google Scholar]
[5]. Sáez Rodríguez M, Rodríguez-Martin M, Carnerero A, Sidro M, Rodríguez F, Cabrera R, Naevus lipomatosus cutaneous superficialis on the noseJ Eur Acad Dermatol Venereol 2005 19(6):751-52. [Google Scholar]
[6]. Namazi MR, Nevus lipomatosus cutaneous superficialis of the groin arising in the fifth decade of lifeJ Drugs Dermatol 2008 7(8):787-88. [Google Scholar]
[7]. Ghosh SK, Bandyopadhyay D, Jamadar NS, Nevus lipomatosus cutaneous superficialis: An unusual presentationDermatol Online J 2010 16(7):12 [Google Scholar]
[8]. Das D, Das A, Bandyopadhyay D, Kumar D, Huge nevus lipomatosus cutaneous superficialis on back: an unusual presentationIndian J Dermatol 2015 60(3):296-97. [Google Scholar]
[9]. Sakanoue M, Kawai K, Kanekura T, Nevus lipomatosus cutaneous superficialis associated with trichofolliculoma on the lower legIndian J Dermatol 2013 58(4):330 [Google Scholar]
[10]. Kim HJ, Lee MG, Nevus lipomatosus superficialis associated with deep penetrating nevusIndian J Dermatol Venereol Leprol 2015 81(4):410-11. [Google Scholar]
[11]. Moss C, Shahidullah H, Nevi and other developmental defects. In: Burns T., Breathnach S., Cox N., Griffiths C., editorsRook’s textbook of dermatology 2010 8th edWiley-Blackwell Publishing Ltd:18.1-107. [Google Scholar]
[12]. Ragsdale BD, Tumors with fatty, muscular, osseous, and cartilaginous differentiation. In : Elder DE, Elenitsas R, Johnson BL, Jr, Murphy GF, editorsLever’s Histopathology of the Skin 2005 9th edPhiladelphiaLippincott:1061-107. [Google Scholar]
[13]. Pai VV, Naveen KN, Athanikar SB, Rao R, Sori T, Unusual presentation of naevus lipomatosus cutaneus superficialisIndian J Dermatol 2013 58(6):486-87. [Google Scholar]
[14]. Kim YJ, Choi JH, Kim H, Nam SH, Choi YW, Recurrence of nevus lipomatosus cutaneous superficialis after CO2 laser treatmentArchives of Plastic Surgery 2012 39(6):671-73. [Google Scholar]