Human Immunodeficiency Virus (HIV) infection is one of the serious public health issues of modern times [1]. Globally in 2014 an estimated 36.7 million people were living with HIV and 2.1 million people were newly infected with HIV [2]. India has the third highest number of people living with HIV in the world [2]. As per the National Sentinel Surveillance 2014-15 the overall HIV prevalence among general population in India is 0.29% and in Rajasthan is 0.32%, slightly higher than the national prevalence [3].
HIV infection reduces the number and functionality of CD4 helper lymphocytes that direct and coordinate acquired immunity against most pathogens [4]. The decrease in CD4+ T lymphocyte count leads to various Opportunistic Infections (OI) in HIV infected persons [5]. Opportunistic respiratory tract infections are common and remain a major cause of morbidity and mortality in HIV patients [6]. In developing countries patients are usually unaware of their HIV status until they are tested on presentation with symptoms suggestive of this infection. It is estimated that 65% of the patients infected with HIV present with pulmonary involvement as their first clinical manifestation, and that approximately 80% of HIV positive patients have some kind of pulmonary involvement over the course of the disease [7]. Infection by fungal species depend both on amount of inoculum size at the time of exposure and general resistance of the host [8]. The extent of fungal illness varies from asymptomatic mucosal candidiasis to overwhelming disseminated infections, fungal pneumonia and life threatening meningitis [8]. The diagnosis of fungal lung infection is most often delayed because of lack of consideration of these as causative agent by clinicians. In HIV the immune status and the risk of infection with specific aetiologic agents, changes with time and with the stage of the disease [9]. In HIV seropositive patients the aetiology of pulmonary disease is vast and varies from place to place [10]. This study will further add to our knowledge of the prevailing profile of fungus in sputum of HIV positive patients with lower respiratory tract infections in this region. It will also define the range of CD4+ T lymphocyte count where various fungal species can be suspected as probable pathogen.
Materials and Methods
This study was conducted in the Department of Microbiology, Sawai Man Singh Medical College Jaipur from May 2014 to April 2015. One hundred and eighty treatments naive, HIV sero-positive patients, of both sexes, having LRTI, attending the Integrated Counselling and Testing Centre (ICTC) were included. The HIV status of these patients was confirmed by three tests with different antigens or principles as recommended by National AIDS Control Organisation (NACO) [11]. After obtaining informed consent from the patients, the socio demographic details, clinical signs and symptoms, occupation, education and history of risk behaviour were filled on a structured proforma. Ethical clearance for the study was taken from college research review committee. Patients who had prior antiretroviral or antifungal treatment were excluded.
CD4+ T lymphocyte count estimation was done by flow cytometry using BD FACS Calibur (Becton Dickinson Immunocytometery System, San Jose, CA, USA) as per manufacturer’s instructions [12]. Sputum samples were collected from the patients who were diagnosed HIV positive and who had complaint of cough and fever. The patients were visiting the ICTC for the first time. From each patient, both early mornings expectorated and induced sputum samples were collected. Patients were asked to collect the expectorated sample in a sterile wide mouth container. Induced sputum sample was collected at ICTC. All samples were kept at 4°C until processed. The quality of expectorated sputum was evaluated macroscopically and by Bartlett’s scoring method [13].
The sputum specimens were subjected to microscopy using Gram staining & KOH mount. India ink preparation was done only when capsulated budding yeast cells were seen on Gram staining. Specimens were inoculated in duplicate on Sabouraud’s Dextrose Agar (SDA) with chloramphenicol (16mg/ml) and incubated at 25°C and at 37°C. The cultures were examined on alternate days for growth, for 21 days before discarding them as negative. Macroscopically fungal growth was identified by rate of growth, colony morphology, texture and surface pigmentation [14]. Microscopic identification of molds was done by morphology and arrangements of the spores and hyphae on Lacto Phenol Cotton Blue (LCB) mount. Micro slide culture was done in case the sporulating structures were not clear on LCB mount [14].
When mucoid yeast-like growth was present on SDA, Gram staining was done. If capsulated budding yeast cells were seen on Gram staining Christiensens’ urea agar and Bird Seed Agar was inoculated to identify Cryptococcus neoformans [14].
Candida species were identified by germ tube test, chlamydospore formation on cornmeal agar, sugar assimilation and fermentation test [14].
Induced sputum was examined for the presence of trophozoites and cysts of Pneumocystis jiroveci by Giemsa, Toludine Blue and Gomori’s Methamine Silver staining [15].
One sample of suspected Aspergillus nidulans was confirmed from PGI Chandigarh.
Results
In the present study the mean age of patients was 37.21 ± 11.2 years. Majority (63.9%) of the patients were in the age group of 21 to 40 years. Males outnumbered females with male female ratio 1.95:1 [Table/Fig-1]. Labourers were the most affected group [Table/Fig-2]. The most common route of HIV transmission was heterosexual contact noticed in 171 (95%) patients, followed by perinatal route in 7 (3.89%) patients. The mean CD4+ T lymphocyte cell count of patients was 209.05±195.23 cells/μl. The mean CD4+ T lymphocyte count of males was 192.85±189.70 cells/μl and females were 240.66±203.47 cells/μl. No significant difference was found in CD4+ T lymphocyte counts of males and females. The majority of patients had CD4+ T lymphocyte counts between 101-200 cells/μl [Table/Fig-3]. Fungal species were isolated from 155 (86.1%) patients. The most common isolate was Candida albicans (31.7%), followed by Aspergillus niger (17.7%) and Aspergillus flavus (10%). No mixed fungal growth was isolated. Alternaria species, Aspergillus niger, Aspergillus flavus, Aspergillus nidulans, Penicillium species, Cryptococcus species, Candida tropicalis and Candida parapsilosis were isolated from sputum of patients with CD4+ T lymphocyte cell count <350 cells/μl, whereas Candida albicans, Candida pseudotropicalis and Mucor species were also seen in patients with CD4+ T lymphocyte cell count >350 cells/μl [Table/Fig-4,5,6 and 7].
Age & sex distribution of HIV positive patients with LRTI.
| Character | No. of patients(n=180) | Percentage of patients |
|---|
| Sex |
| Male | 119 | 66.1 |
| Female | 61 | 33.9 |
| Age Group (years) |
| 0 to 10 | 2 | 1.1 |
| 11 to 20 | 7 | 3.9 |
| 21 to 30 | 43 | 23.9 |
| 31 to 40 | 72 | 40 |
| 41 to 50 | 37 | 20.6 |
| ≥51 | 19 | 10.5 |
| Mean Age | 37.21 ± 11.2 years | |
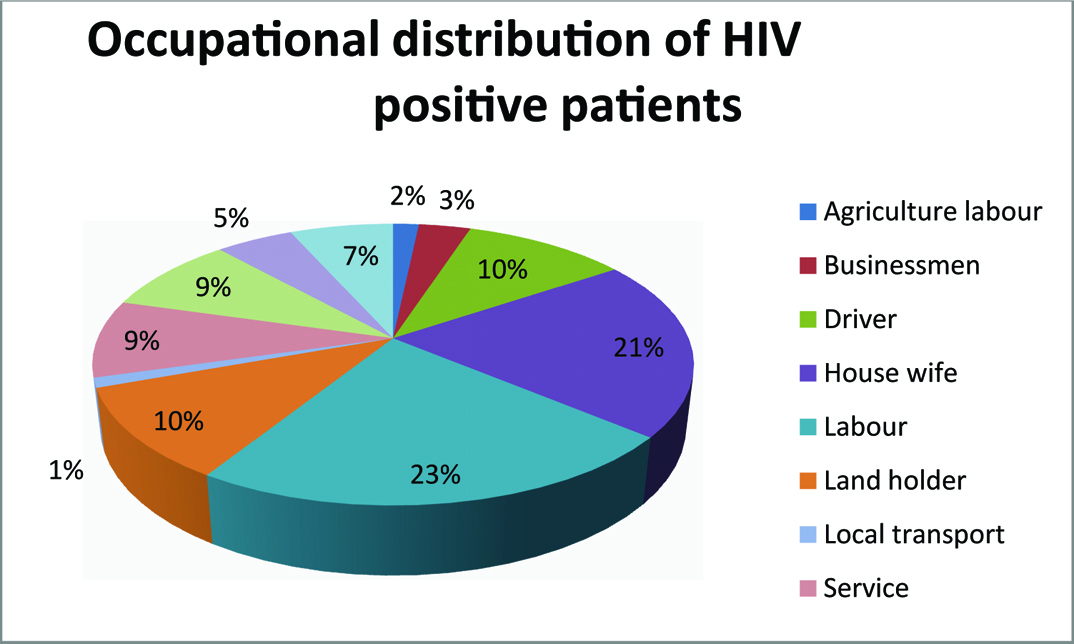
Occupational distribution of HIV positive patients with LRTI.
CD4+ T Lymphocyte cell count (cells/μl) of HIV Positive patients with LRTI.
| CD4+ T lymphocyte cell Count (cells/μl) | Number of patients | Percentage of patients (%) |
|---|
| <50 | 42 | 23.3 |
| 51 to 100 | 25 | 13.9 |
| 101 to200 | 46 | 25.6 |
| 201 to 350 | 31 | 17.2 |
| 351 to 500 | 20 | 11.1 |
| > 500 | 16 | 8.9 |
| Total | 180 | 100 |
Distribution of fungal isolates in HIV positive patients and its relation with CD4+ T Lymphocyte cell count.
| FungusN=155 | No. of isolates | CD4+ T Lymphocyte cell count(cells/μl) |
|---|
| <50(N=42) | 50-100(N=25) | 101-200(N=46) | 201-350(N=31) | 351-500(N=20) | >500(N=20) |
|---|
| Alternaria.species | 5 | 2 | 1 | 2 | 0 | 0 | 0 |
| (40) | (20) | (40) | (0) | (0) | (0) |
| Aspergillus niger | 32 | 13 | 9 | 6 | 4 | 0 | |
| (40.6) | (28.1) | (18.7) | (12.6) | (0) | 0 |
| Aspergillus flavus | 18 | 4 | 3 | 8 | 3 | 0 | (0) |
| (22.2) | (16.7) | (44.4) | (16.7) | (0) | 0 |
| Aspergillus nidulans | 1 | 0(0) | 1(100) | 0(0) | 0(0) | 0(0) | (0) |
| Penicillium species | 12 | 5 | 2 | 2 | 3 | 0 | 0 |
| (41.6) | (16.7) | (16.7) | (25) | (0) | (0) |
| Mucor species | 5 | 1 | 0 | 2 | 0 | 1 | 1 |
| (20) | (0) | (40) | (0) | (20) | (20) |
| Candida pseudo-tropicalis | 9 | 2 | 0 | 5 | 1 | 0 | 1 |
| (22.2) | (0) | (55.6) | (11.1) | (0%) | (11.1) |
| Candida tropicalis | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| (0) | (0) | (100) | (0) | (0) | (0) |
| Candida albicans | 57 | 7 | 5 | 13 | 16 | 9 | 7 |
| (12.2) | (8.8) | (22.9) | (28) | (15.9) | (12.2) |
| Candida parapsilosis | 12 | 3 | 2 | 3 | 4 | 0 | 0 |
| (25) | (16.6) | (25) | (33.4) | (0) | (0) |
| Cryptococcus species | 3 | 2 | 1 | 0 | 0 | 0 | 0 |
| (66.6) | (33.4) | (0) | (0) | (0) | (0) |
| Total | 155 | 39 | 24 | 42 | 31 | 10 | 9 |
Note: Figures in parenthesis indicates percentage
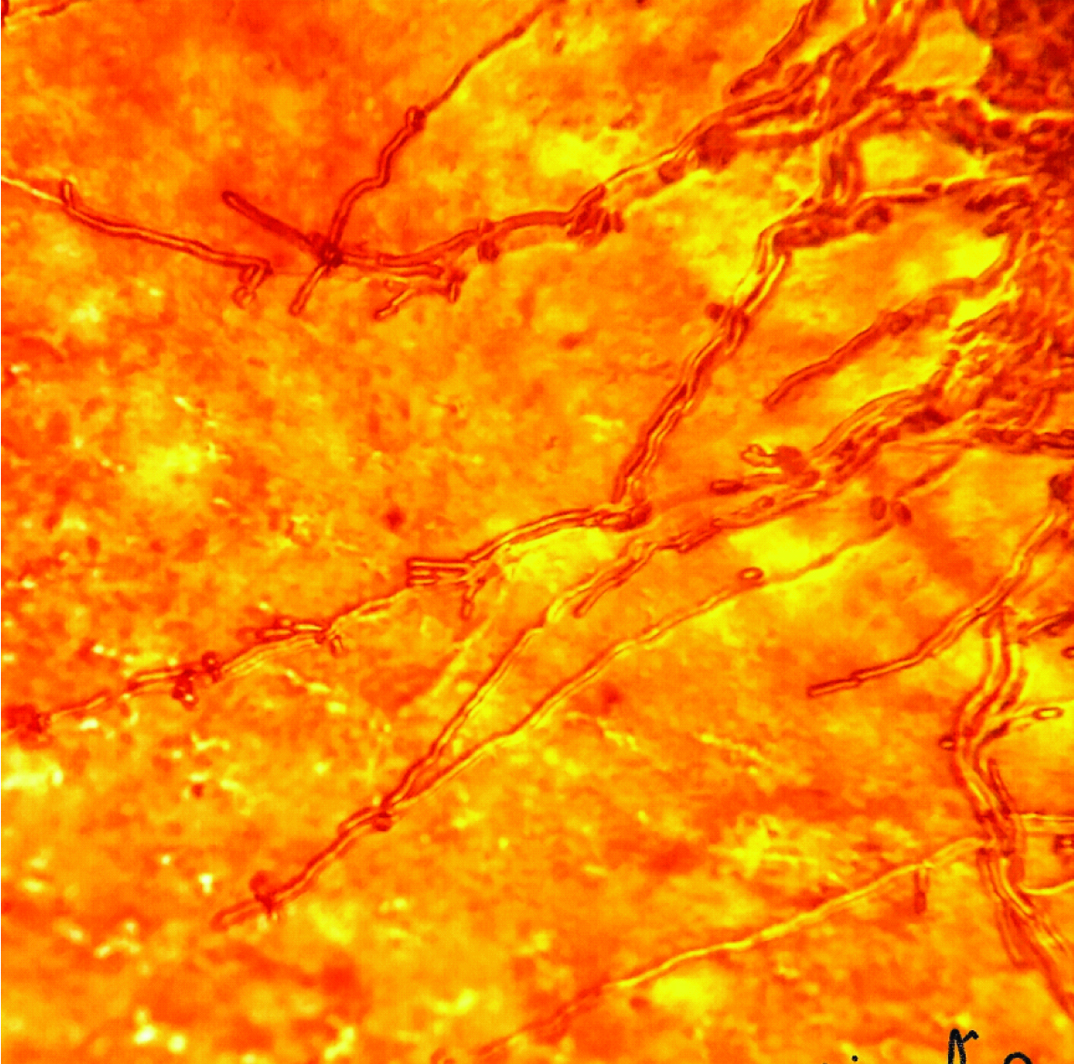
Aspergillus nidulans in LCB stain (400X).
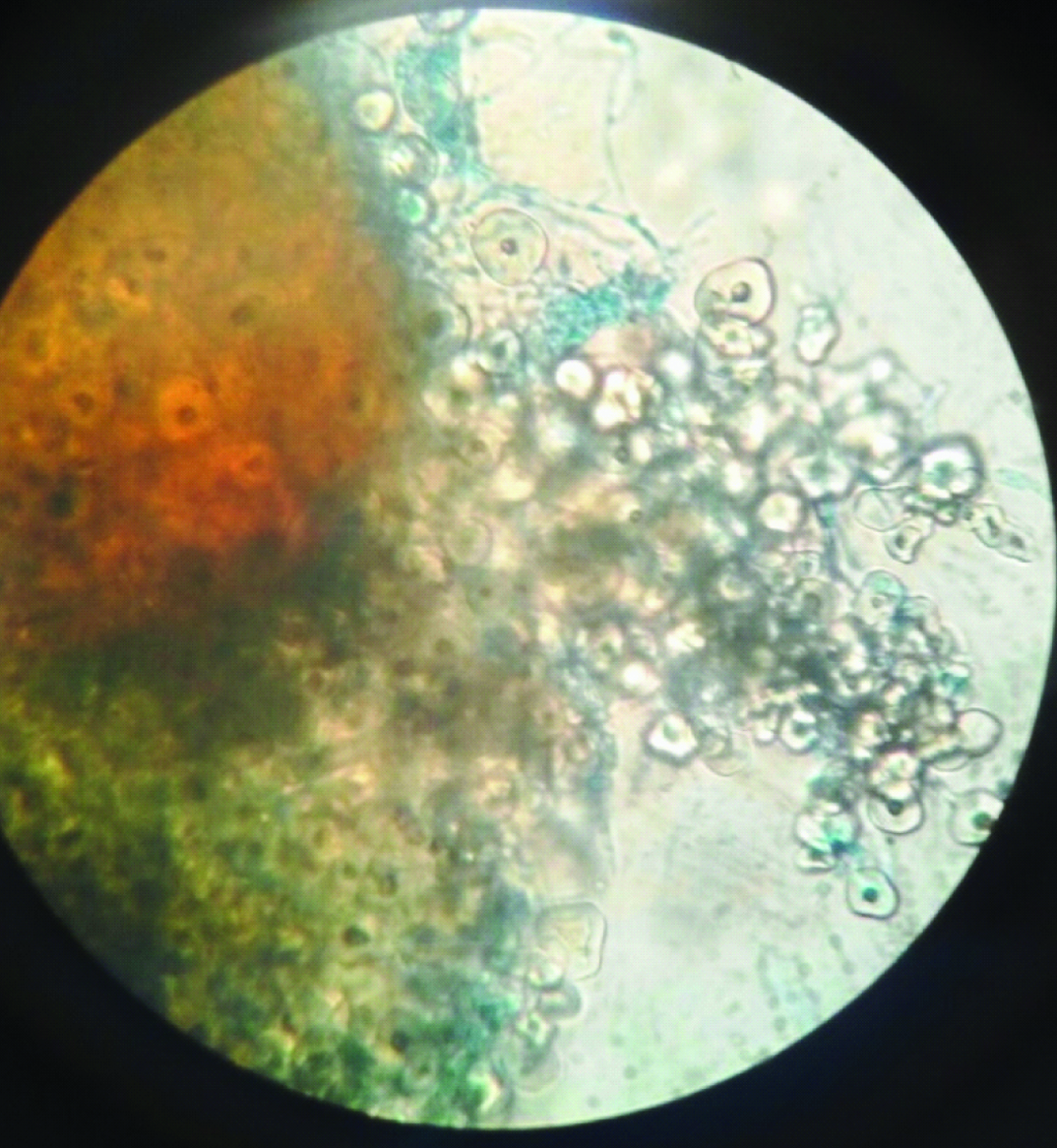
Cleistothesia with hulle cells of Aspergillus nidulans in LCB stain (400X).
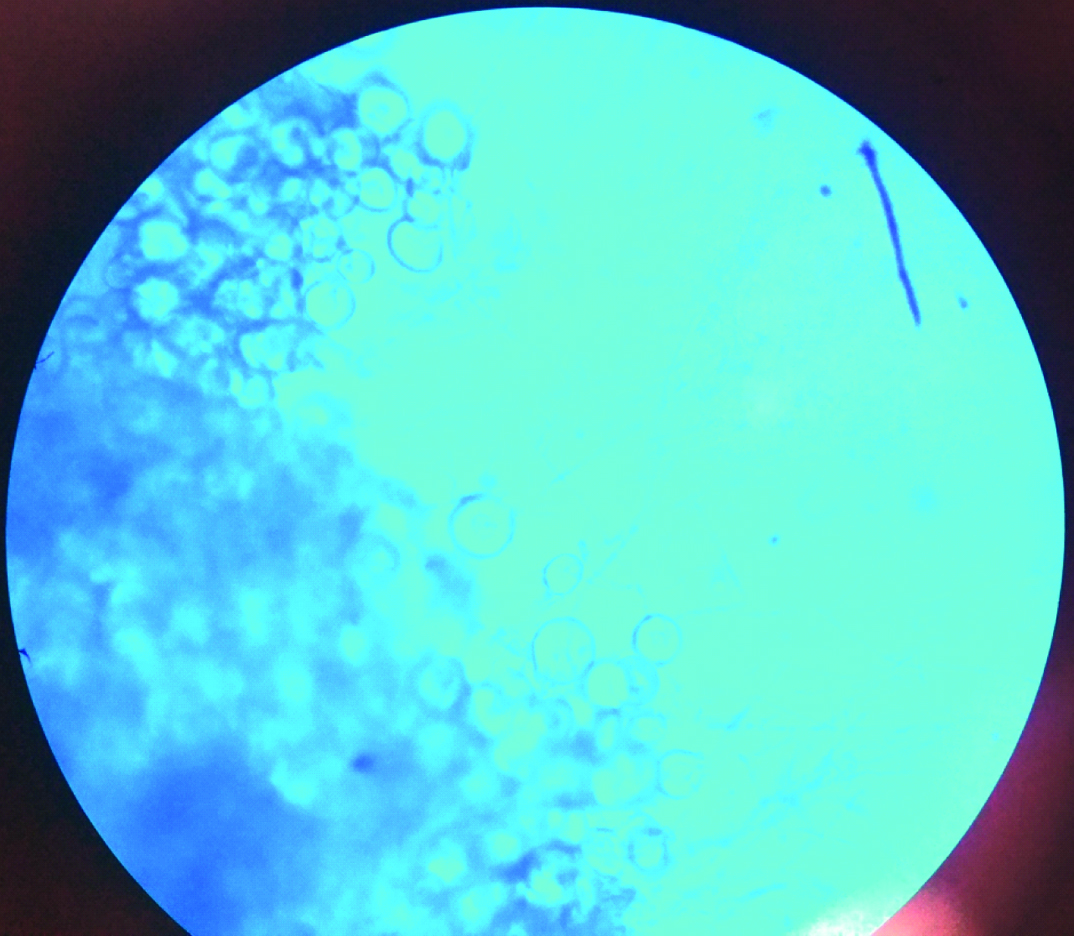
Log in the steam appearance of Candida pseudotropicalis on cornmeal agar.
Discussion
Opportunistic pneumonias are the major cause of mortality and morbidity amongst the HIV seropositive patients [16] Fungus is one of the important causes of LRTI. Identification of the fungal species is important, as it helps in the initiation of specific antifungal therapy which improves the outcome of treatment.
In the present study most of the HIV positive patients were in the age group of 31-40 years(40.0%) followed by the age of group 21-30(23.9%). The mean age of HIV positive patients was 37.21±11.2 years. The higher mean age of HIV positive patients may be because the index of suspicion is low and testing for HIV infection is carried out only when clinical signs and symptoms start appearing, which happens in the advanced stage of infection. Our findings are consistent with other studies elsewhere in India [17–19].
In the present study male patients were more than females. The male female ratio was 1.95:1. Majority of patients were non agriculture labourers, truck drivers, business/self employed and housewives. Our findings are consistent with that of Khan et al., and Shilpa et al., [1,17]. However, in the study conducted by Chakraborty et al., and Sangeeta et al., majority of patients were males (84% and 75% respectively) [18,20]. The male prevalence seen might have been due to the fact that in the existing social milieu in India, females do not seek medical care because of fearing isolation and loss of family support. Male migrates to different places for education and work. Migrants form a link between urban and rural areas, and high-risk and low-risk groups [21]. About 75% of women testing positive in India have a husband who is a migrant labourer [21]. Migrants returning back may infect their wives which significantly increases the rate of infection among housewives. Truck drivers themselves are a highly vulnerable group for HIV infection. They stay away from their families for extended period of time and are in close proximity to “high risk” sexual network. Awareness about HIV transmission is low among truck drivers. Approximately 2.6% of the two million truckers in India are living with HIV [22].
In present study in 95% of patients HIV was transmitted through heterosexual contact. However Chakraborty et al., and Gupta et al., reported transmission by heterosexual route only in 64% and 66.6% of cases respectively [18,23].
In the present study, 113(62.7%) patients had CD4+ T lymphocyte cell counts <200 cells/μl. Our results are comparable with results of Chakraborty et al., who reported CD4+ T lymphocyte cell counts <200 cells/μl in 75% of cases [18]. However, Bharathi et al., reported 21% of patients with CD4+ T lymphocyte cell counts <200 cells/μl [24].
In the present study, fungus species were isolated from 86.1% of patients. Out of them Candida albicans was the most common fungus isolated from 57 (36.7%) patients. Non AlbicansCandida (NAC) was isolated from 22 (14.1%) patients. Our results are consistent with that of Ochiabuto et al., and Usman et al., who reported Candida albicans from 30% and 26% of patients respectively [25,26]. However Bharathi et al., reported Candida albicans from 26% of patients and Non-albicansCandida from 29% of patients [24]. Even though Candida albicans is the most common causative agent, the incidence of non-albicanscandida has been increasing in last few years due to increased use of antifungal drugs [27].
In the present study, 41(71.92%) isolates of Candida albicans and 21(95.45%) isolates of NAC were isolated from patients with CD4+ T lymphocyte cell count <350 cells/μl. Our results are consistent with that of Rajeev Shah [28], whereas, Ochiabuto et al., observed Candida albicans from patients with CD4+ T lymphocyte cell count <200 cells/μl [25]. Candida is part of normal flora of upper respiratory tract. When immunity is low it acts as an opportunistic pathogen [29]. HIV positive individuals also have other predisposing factors like neutropenia, lymphopenia, selective T cell defects, altered monocyte macrophage function and frequent lowered immunity due to low CD4+ T lymphocyte count [29]. All these factors contribute to the development of opportunistic pulmonary candidiasis.
Aspergillus species are ubiquitous molds found in organic matter [29]. Aspergillus primarily affects the lungs [29]. The fungal spores are transmitted to the human via inhalation. Alveolar macrophages are the first line of defence against inhaled Aspergillus conidia [29]. In the present study, Aspergillus species were isolated from 51 (32.9%) patients. The most common species was Aspergillus niger isolated from 32(20.6%) patients, followed by Aspergillus flavus from 18 (11.6%). Ochiobuto et al., also reported Aspergillus from 27.9% of cases however in their study the most common species was Aspergillus fumigatus followed by Aspergillus niger [25]. This may be due to geographic and temporal variation.
In the present study 30(58.23%) isolates of Aspergillus species were from patients with CD4+ T lymphocyte count <100 cells/μl. No Aspergillus species was isolated from patients who had CD4+ T lymphocyte count >350 cells/μl. In human defence against the inhaled spores of Aspergillus begins with the mucous layer and the ciliary action in the respiratory tract [29]. Macrophages and neutrophils encompasses, engulfs, and eradicates the fungus [29]. Immunosuppression in HIV contributes directly to neutrophil dysfunction or decreased number of neutrophils leading to failure in eradication of fungus. HIV-associated aspergillosis is seen in patients who have CD4+ counts <100 cells/μL [30], a history of other AIDS-defining opportunistic infections, and patients who are not receiving antiretroviral therapy (ART). Our results are consistent with that of Khan et al., and Mylonakis et al., [1,31].
Aspergillusnidulans is a low grade pathogen and has been rarely reported to cause human disease [32]. In the present study, Aspergillusnidulans was isolated from one HIV positive patient with the clinical symptom of chest pain and cough. The patient had CD4+ T lymphocyte cell count of 83 cells/μl. To the best of our knowledge it was the first case reported from HIV positive patient with lower respiratory tract infection from Rajasthan.
Cryptococcosis is one of the AIDS defining infections [33]. The respiratory route is the most likely portal of entry however pulmonary cryptococcosis is diagnosed less frequently than meningitis in patients with AIDS. In the present study Cryptococcus species were isolated from 3 (1.66%) patients with CD4+ T lymphocyte cell count <100 cells/μl. Our findings are similar with that of Usman et al., who reported Cryptococcus species from 1.4% of cases [26]. All HIV positive patients in whom C. neoformans is isolated from the sputum should be considered for antifungal treatment to prevent dissemination of infection [34].
In the present study, Penicillium species, Mucor species, Alterneria species were isolated from 7.7%, 3.2%, 3.2% patients respectively. All the species were isolated from patients having CD4+ T lymphocyte cell count<200cells/μl. Our findings are consistent with other studies [17,19].
Pneumocystis jirovecii pneumonia is one of the AIDS-defining illness [35]. In the present study none of the sputum samples were positive for Pneumocystis jirovecii. Prevalence of Pneumocystis jirovecii is low in India. Similar observation was made by Shailaja et al., and K Shreevidhya et al., [36,37], however Rupali et al., reported Pneumocystis jeroveci from 7% of patients [38].
Conclusion
This study provides a basis for early suspicion of fungal aetiology in respiratory tract infections in treatment naive HIV positive patients. Definitive diagnosis of fungus is time consuming and it is difficult to arrive at a diagnosis based exclusively on signs and symptoms. We have been able to define some correlation between CD4+ T lymphocyte cell count and fungal species causing LRTI which can be helpful in early diagnosis. Fungus was isolated from 86.1% of patients; it is desirable to screen all HIV positive individuals with cough for fungal pathogens. Empirical antifungal treatment should be included for lower respiratory tract infections in these patients. The study finding also indicates that high CD4+ T lymphocyte counts are protective for fungal colonization. As invasive fungal colonization of the lungs remains important cause of death in immunocompromised patients, early isolation, identification and treatment of the colonizing fungi can improve the prognosis of patients.
Note: Figures in parenthesis indicates percentage