Subcoracoid impingement is an unc ommon condition wherein there is narrowing of the space between the coracoid process and the humerus. It is an often unrecognized cause of shoulder pain, but is an important entity to be mindful of as it has been identified as a cause of persistent postoperative shoulder pain after rotator cuff repair [1]. The primary cause of this condition has been determined to be the impingement of the lesser tuberosity of the humerus against the coracoid process [2]. Clinically subcoracoid impingement is characterized by pain at the anterior aspect of the shoulder that is induced by adduction, internal rotation and forward flexion [3]. This position leads to narrowing of the coraco-humeral interval (CHI)- that is, the space between the coracoid process and the lesser tuberosity of the humerus. Structures in the rotator interval are at greatest risk for impingement which includes the subscapularis tendon, tendon of the long head of the biceps, and the middle gleno-humeral ligament.
Clinical suspicion of subcoracoid impingement must lead to directed investigation in the form of specific MRI imaging of the shoulder to evaluate the CHI distance. Rotator interval pathologies such as subscapularis tear and long head of biceps tendon subluxation and/or fraying must be examined for.
This prospective study intended to determine the radiological confirmation of Subcoracoid impingement and also gives an insight into the extent of CHI reduction that could possibly lead to subscapularis tendon tears.
To study the prevalence of radiological evidence of reduced CHI in patients with clinically evident subcoracoid impingement and to examine the presence of subscapularis tears in these patients.
Materials and Methods
This was a prospective study done at our Institute which is a tertiary care centre, from January 2014 to December 2015, after approval was obtained from the institutional review committee and patient consent. Inclusion criteria were all patients who presented with clinical evidence of subcoracoid impingement and underwent arthroscopic surgery. Patients with infection, arthritis and significant cuff tear arthropathy were excluded.
A total of 24 patients were included in this prospective study, of which 6 were males and 18 were females. Age of the patients ranged from 41 to 71 years (mean age 52.83 years). All patients had presented with shoulder pain, difficulty in shoulder abduction and restriction of overhead activities. They were clinically assessed in the outpatient department and were diagnosed to have rotator cuff pathology after thorough examination. Clinical examination included the coracoid impingement test which involved cross arm adduction, forward elevation and internal rotation of the arm. Nine of the patients tested positive in the form of having pain during mid-range of elevation while performing this test, thus indicating the presence of subcoracoid impingement [3].
MRI of the shoulder was obtained for all patients with images also being procured with the humerus in maximal internal rotation apart from routine images. Static MRI images were obtained and T1 or proton density images were used for measurement as the cortical margins were best outlined in them [4]. The CHI was measured in the axial and oblique sagittal images as the shortest distance between the outer cortices of the coracoid process and adjacent lesser tuberosity of the humerus. Evidence of bony or soft tissue oedema and observation of soft tissue impingement were recorded. Presence of a tear in the subscapularis tendon and rotator interval pathology was noted.
Clinical data, CHI values obtained from MRI and presence of subscapularis tears were correlated and subjected to statistical analysis. A CHI of 5.5mm was used as a cut-off and percentage of patients with a Subscapularis tear was determined in relation to this value. Statistical evaluation of the data was performed using Students t-test and Fisher’s-exact test. On completion of analysis, the results were applied to two cohorts of patients. One cohort consisted of patients who had a CHI value of less than 5.5mm and the other cohort had a CHI value greater than 5.5mm. Average CHI values in patients with and without a subscapularis tear were determined.
Results
Among the 24 patients included in this study who were diagnosed to have rotator cuff tears, 9 of them were found to have clinical signs of Subcoracoid impingement concomitantly. On MRI, all 9 of these patients were found to have a reduced CHI value with the average being 5.33mm (range 4.6mm to 5.9mm, SD=0.43). These patients were also found to have an associated tear in the Subscapularis tendon with long head of biceps tendon subluxation and/or fraying. The remaining 15 patients of the cohort had an average CHI value of 10.48mm (range 8.6mm to 12.4mm, SD=0.87). These patients were found to have intact Subscapularis tendons with no signs of rotator interval pathology on MRI, but had tears elsewhere i.e., in the supraspinatus or Infraspinatus tendon. The difference between these two groups of patients was found to be statistically significant with a p-value<0.001. The cases with Subscapularis tear was associated with lower CHI value of 5.34 mm [Table/Fig-1]. Significant p-value between the group showed that subscapularis tears are associated with reduced CHI [Table/Fig-2]. The number of patients who had a CHI value of less than or equal to 5.5mm was found to be seven, whereas 17 patients had a CHI value more than 5.5mm. All the seven patients with CHI<=5.5mm were found to have a subscapularis tear with long head of biceps tendon subluxation or fraying. Of the remaining 17 patients, two patients were found to have a subscapularis tear, whereas rest 15 patients did not have the same. The difference between these two groups was found to be statistically significant with a p-value<0.001.
Graph showing the mean CHI values in patients with and without subscapularis tear.
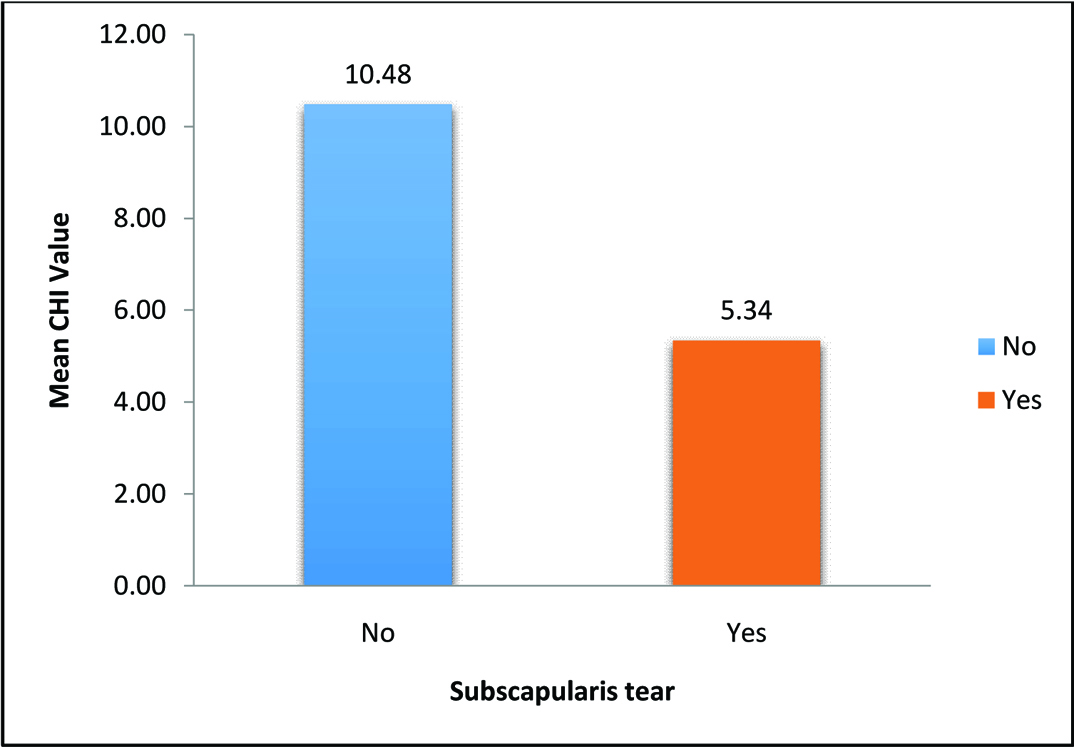
Mean and SD values of CHI in patients with and without Subscapularis tear.
| Subscapularis tear | No. of patients | CHI | p-value |
|---|
| Mean | SDs |
|---|
| No | 15 | 10.48 | 0.87 | <0.001 |
| Yes | 9 | 5.33 | 0.43 |
Of the two cohorts, < 5.5 mm group showed that all cases with CHI< 5.5 mm had Subscapular tears [Table/Fig-3]. Significant p-value showed that CHI < 5 mm is associated with subscapularis tears [Table/Fig-4].
Percentage of patients having a subscapularis tear.
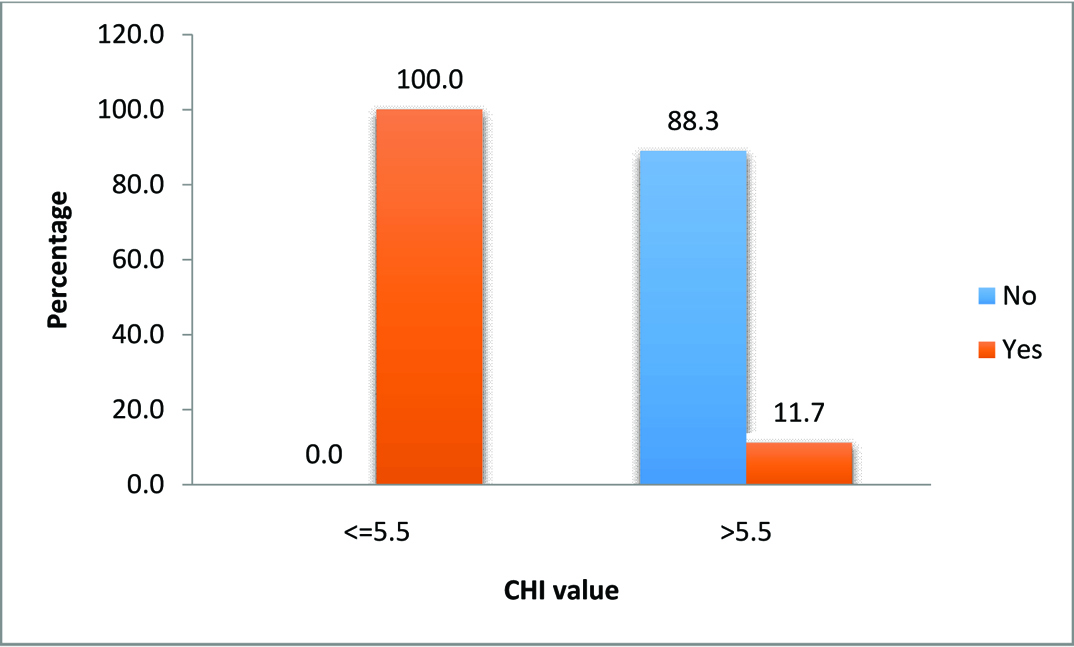
Patients having Subscapularis tear in relation to cut-off value of CHI.
| Tear | p-value |
|---|
| CHI (n) | Yes | No | <0.001 |
| >5.5mm (17) | 2 | 15 |
| <=5.5mm (7) | 7 | 0 |
Discussion
Subcoracoid impingement is an infrequently diagnosed cause of anterior shoulder and tends to be overlooked in the presence of rotator cuff tears. This might possibly be due to the presumed low incidence of this condition. But several studies have highlighted that the incidence is much higher [5–8]. Narrowing of the CHI, which leads to subcoracoid impingement, is best reproduced with maximal internal rotation of the humerus [4]. This reduction in the CHI leads to subcoracoid stenosis which has a "roller-wringer effect" on the subscapularis tendon when it gets impinged between the lesser tuberosity of the Humerus and coracoid process. This kind of tension placed on the subscapularis tendon increases the tensile loads on the articular surface of the tendon that leads to Tensile Under surface Fibre Failure (TUFF) lesion of the Subscapularis insertion, which in turn can lead to tendon rupture over a period of time [9].
Gerber et al., in their CT scan based study demonstrated a clinical, radiological and surgical correlation of subcoracoid impingement in 37 symptomatic patients [10]. Friedman et al., established that asymptomatic population had an average CHI of 11mm and patients with anterior shoulder pain had an average CHI of 5.5mm [11].
Some authors have argued that impingement being a dynamic process in especially occurring in forward flexion, adduction and internal rotation requires a dynamic investigation and a quantification like ultrasonography [12]. But they accept inter-observer variation as a major cause of error. Considering this major drawback we accepted MRI as investigation of choice since quantification of CHI is systematic. Specific MRI imaging of the shoulder with the humerus in maximal internal rotation was used as this is the position which produces anterior shoulder pain. Conventional position of MRI to examine for rotator cuff pathology is with humerus in neutral or in external rotation which gives good visualisation of the rotator cuff tendons, has been found inadequate to diagnose subcoracoid impingement [11].
Other studies have tried to find out association of a reduced CHI to partial or full thickness subscapularis tears, mostly taking a CHI value of < 6mm as significant reduction in space [13–15].
Not many published data is available from Asia, but Chen et al., found an average CHI of 8.7mm in Taiwanese patients [16]. European MRI studies like Nové-Josserand et al., found that CHI in asymptomatic patients averaged 11.2 mm and symptomatic patients it was 6.7 mm at maximal internal rotation of the shoulder [15]. Lo and Burkhart favoured a CHI of < 6mm for coracoplasty while Friedman et al., found cut off of 5.5mm as significant reduction in CHI [9,11]. Some other MRI studies have given higher CHI values in symptomatic patients but the position of MRI is in neutral or not mentioned [12,17].
This variation in data was baffling and considering the paucity of data in the Indian population was a hindrance in radiological assessment and planning surgery.
In our study in which MRI was done in position of maximal internal rotation, we have obtained a mean value of 10.48mm in the patients who did not have clinical signs of Subcoracoid impingement and in the cohort of patients who were clinically diagnosed with subcoracoid impingement were found to have a mean CHI of 5.3mm which is close to the values obtained in the earlier studies.
We further adopted 5.5mm as cut-off CHI value for deciding the cohorts, this was done since the MRI was done in a similar position as described by Friedman et al., [11].
There are few studies that demonstrate a correlation between the clinical diagnosis of subcoracoid impingement and radiological evidence of reduced CHI. We have been able to obtain statistically significant results in our study which demonstrate that patients with clinically diagnosed subcoracoid impingement have a significant reduction in the CHI as seen on MRI. In addition, these patients have rotator interval pathology in the form of a Subscapularis tendon tear and/or long head of biceps tendon subluxation or fraying. This is also in concurrence with the study conducted by Millet et al., based on 94 patients which showed a significant association between narrowing of CHI and rotator interval pathologies [18].
Limitation
The limitation of this study is that the sample size is small, owing to it being a single centre study. Evaluation of effect of sex of patient in the study was not possible as we had a predominantly female skewed cohort of patients. The morphology of the coracoid process has been ascribed a significant role in the process of subcoracoid impingement which needs further examination and is planned in our on-going prospective study.
Conclusion
Patients who present with anterior shoulder pain, especially during activities involving forward flexion, adduction and internal rotation of the arm such as driving or during follow-through phase of throwing must be examined with a high index of suspicion for subcoracoid impingement. If clinical tests for subcoracoid impingement reproduces the symptoms, investigation with MRI of the shoulder with images being specifically obtained in the position that reveals narrowing of CHI i.e., with maximal internal rotation of Humerus is helpful in diagnosis. Reduction of CHI has been found to have a significant association with rotator interval pathologies such as subscapularis tendon tear and long head of biceps subluxation or fraying. Treatment of such patients should include modalities such as coracoplasty or anterior shoulder stabilisation apart from a rotator cuff repair, as is deemed fit for each case, to prevent persistent postoperative anterior shoulder pain or functional deficits.