Root canal therapy is an invaluable measure to preserve the teeth than being extracted. With advancing technology, better understanding of the root canal anatomy and usage of improved biocompatible materials; success rate of root canal therapy has increased. Gutta-percha has been in use for over a century to fill root canals and it remains the material of choice.
Bacterial residue in the root canal system plays a significant role in the prognosis of root canal treatment. When a tooth is infected before treatment, success of the root canal therapy drops to 79%, as compared to the 93% success rate of the canal treated without any infection like apical periodontitis [1].
Complete elimination of bacteria from the root canal prevent re-infection which remains to be a major goal of endodontic treatment [2]. Biomechanical instrumentation, intracanal irrigation, intracanal medication and root canal filling are the pivotal steps in the root canal system for reducing the population of micro-organisms. It seems that complete removal of micro-organisms has proven to be difficult in endodontic treatment and the endodontic material that could sustain in the root canal having high antimicrobial efficacy can serve as an eminent weapon in reducing the growth of micro-organisms [3].
Systemic administration of an antibiotic and the negligible concentration reaching the root canal is unlikely to be beneficial. The main advantage of local delivery of antibiotics is substantially higher concentrations of drug gets diffused and utilized in inaccessible areas compared to systemic route [6,7]. E.faecalis is susceptible to Amoxicillin-Clavulanic acid [6] and Ofloxacin-Ornidazole combinations, hence this combination was tried and tested in the present study.
Various studies have shown that gutta-percha cones impregnated with antibiotics remain in inert form and when it comes in contact with tissue fluid, the antibiotic gets activated [3]. Till date, antimicrobial property of gutta-percha alone or Tetracycline impregnated gutta-percha have been tested. None of them is effective against E.faecalis [3]. Hence an attempt has been made to assess the antimicrobial efficacy of antibiotic coated gutta-percha cones on E.faecalis.
Materials and Methods
This was an invitro study, conducted at Department of Public Health Dentistry and Department of Microbiology at ACPM Dental College, Dhule, Maharashtra, India. Ethical clearance for the study was obtained from Institutional Ethical Committee. Different antibiotics used in the study were Amoxicillin, Amoxicillin-Clavulanate combination and Ofloxacin-Ornidazole combination. [Table/Fig-1].
Schematic representation of Methodology.
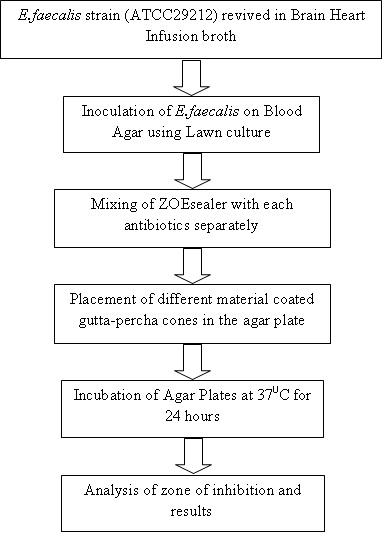
Preparation of the medium for E. faecalis: Standard strains of E. faecalis (ATCC29212) spores were procured from HiMedia Laboratories, Mumbai. The bacterium was grown and maintained on Brain Heart Infusion (BHI) broth (HiMedia Laboratories, Mumbai). To preserve the bacterium and its characteristics, cultures were frozen (-20°C) in vials with glycerol from which new stock cultures were periodically established. Initially, as per the manufacturer’s instructions viability of spores was checked by reviving a pellet from the available vial of E.faecalis into 5ml of BHI broth at 37oC for 18 hours followed by observing changes in turbidity to check bacterial growth. A spectrophotometer was used to check bacterial concentration of a drop of BHI containing E.faecalis placed in saline solution. The broth culture suspension of bacteria was adjusted at a density equivalent to the barium sulfate standard of 0.5 McFarland units (equivalent to 1.5x108 CFU/ml) [8].
Preparation of the blood agar plates: Whenever we design a study, an appropriate justification for the sample size should be provided in the protocol. However, there are a number of settings when undertaking a pilot trial, there is no prior information to base a sample size on. A sample size of 12 per group is recommended in such pilot studies. The rationale behind selecting this sample size is taking into account the feasibility; precision about the mean and variance; and regulatory considerations. Depending on the information obtained from the pilot study, future studies will be carried out [9]. Based on this justification, nearby round value i.e., 15 blood agar plates of 15×100mm were prepared for inoculation. Blood agar was used to culture E.faecalis as it is one of the most common, easily available, enriched and economical culture medium [10]. Blood agar plates were prepared according to the manufacturer’s instructions. The plates were incubated at 37oC for 24 hours in ambient atmosphere to check any external contamination [8]. Microbiologist helped in obtaining the lawn culture by evenly swabbing the blood agar plates inoculated with prepared E.faecalis suspension with a sterile cotton swab.
Traditionally, antimicrobial activity of endodontic materials is assessed by agar disc diffusion method and agar dilution method. Agar dilution method was difficult, technique sensitive, could alter some properties of the sealer being tested and moreover, some sealers could not be homogenously dissolved. Agar Disc Diffusion method (Kirby-Bauer method) offered more advantages like chemical properties of the sealer was not changed, an easy and less technique sensitive method so it was used in the present study [10,11].
Today, numerous root canal sealers are available, based on various formulas. Canal sealers containing Zinc oxide-Eugenol (ZOE, PDP Pvt Ltd.) have a strong antibacterial effect so it was used [12]. ZOE sealer was mixed on sterile glass slab according to manufacturer’s instructions to get homogenous consistency using sterile stainless steel spatula. Single dose of antibiotics adhering to manufacturer’s instructions were added to freshly mixed ZOE cement. Similarly ZOE mixed with different antibiotic formulation was prepared. Gutta-percha cones of same size and company were taken and coated with the respective antibiotics along with ZOE using varnish. Immediately, antibiotic coated gutta-percha cones and Conventional gutta-percha cones (coated only with ZOE sealer) were aseptically transferred into the inoculated plates. The agar plates were placed in the incubator and incubated at 37oC for 24 hours. Zones of inhibition were measured at the end of 24 hours using Vernier Calliper [13]. A single examiner calibrated prior to and during the study carried out all the measurements of zone of inhibition. Intraexaminer variability was minimized by re-examining 5% of the samples and it was determined using kappa statistics (k). According to Landis and Koch, the scientific requirement for validity and reliability was fulfilled as the intraexaminer agreement score (k=0.94) was obtained [13].
Zone edge corresponds to the point of abrupt diminution growth i.e., complete growth inhibition [8,14]. Microbial zones of inhibition were measured in millimeters (mm), and the largest diameter was recorded. Clear zones known as ‘Zone of Inhibition’ were formed on the culture due to emergence of antibiotics & antibacterial agents through the disc from the sealer [14,15]. Results were recorded by group and were statistically analysed with analysis of variance (ANOVA) followed by Tukey post-hoc test for group wise comparisons. The p-value <0.001 was considered statistically significant.
Results
In the present study, diameter of zone of inhibition (in mm) obtained for group A, group B, group C and group D were 5±0.03, 26.6±0.05, 21.5±0.04 and 15.8±0.03 respectively [Table/Fig-2].
Zone of inhibition (in mm) measured at the end of 24 hours.
| Groups | Mean ± SD | Minimum | Maximum | ANOVA | Post-hoc Tukey’s Test |
|---|
| Group A | 5.00 ± 0.03 | 4.91 | 5.05 | One Way ANOVA F = 909017.3, p < 0.001, HS | B>C>D>A |
| Group B | 26.61± 0.05 | 26.53 | 26.68 |
| Group C | 21.53 ± 0.04 | 21.47 | 21.59 |
| Group D | 15.81 ± 0.03 | 15.75 | 15.87 |
Group A-ZOE Coated GP Point Group B – ZOE+Amoxicillin-Clavulanate
Group C – ZOE+Amoxicillin Group D – ZOE+Ofloxacin-Ornidazole ** p < 0.001, HS
All the antibiotics used were effective in inhibiting the E.faecalis. Maximum inhibition was found with Group B against E.faecalis among the different combinations used. The difference in the values of the different antibiotics were statistically significant (p<0.001). Among the 15 values recorded for each group, maximum diameter was obtained with group B i.e., 26.68mm and minimum diameter was obtained with group A i.e., 4.91mm.
Discussion
Direct comparison of the filling materials against the test micro-organisms, indicating which material has the potential to eliminate bacteria in the local micro-environment of the root canal system is possible with agar disc diffusion method. Hence, it was used to assess the antimicrobial efficacy of antibiotic coated gutta-percha cones in the present study [10,11].
The most critical step responsible for root canal treatment failure is improper biomechanical preparation or instrumentation [16–18]. However, occasionally bacteria resistant to conservative treatment may also be involved. Ideally, a sealer should be bacteriostatic or at least, should not encourage bacterial growth [19]. This shows that the antimicrobial property of the sealer along with three dimensional seal are critical factors for endodontic success [17].
It is believed that significant cause of root canal treatment failure is due to re-infection of the root canal system due to persistence of micro-organisms in apical third of root that results in a chronic periapical lesion after endodontic treatment [20]. The antimicrobial efficacy of root canal filling material may help to eliminate residual micro-organisms [21,22]. A high proportion of E.faecalis is seen in such persistent periapical lesions [23]. Predominantly gram-negative anaerobic rods are associated with mixed bacterial flora of primary endodontic infections; whereas E. faecalis is the only one, associated with secondary infection [23]. In the present study, E.faecalis was chosen as it is the most common organism isolated from root canal failures. It is a gram positive, facultative anaerobe capable of surviving extreme environmental challenges and could grow at temperatures ranging from 10°C to 45°C and pH of 9.6. It is a possible microbial factor in a therapy resistant to apical periodontitis as well as resistant to many conventional antimicrobial agents used in dentistry till date [24].
A sealer with additional antimicrobial property can be considered advantageous, in order to eliminate or inhibit the growth of remaining microbes present in the root canal system in order to prevent re-infection [23,25].
ZOE based sealers which meet most of Grossman’s requirements for sealers are still considered as a benchmark against which other sealers are compared [26]. A new paradigm in the form of various antibiotics active against E.faecalis were mixed and tested in order to improve the antimicrobial efficacy of ZOE sealer. Varnish helped in the adhesion of the antibiotic to the surface of gutta-percha. Varnish is a biocompatible material and volatile in nature, hence used in the study. BHI broth was used to revive the spores of E.faecalis according to manufacturer’s instructions [10].
Clavulanate, a broad-spectrum β-lactamase inhibitor active against both Gram-positive and Gram-negative bacteria have been used widely and effectively in treating a broad range of clinical infections for nearly 20 years [27–30]. Literature has very well supported the pharmacokinetic characteristics, the therapeutic success of the Clavulanate-Amoxicillin combination therapy regimens [30].
An invitro study conducted showed greater activity of co-amoxiclav compared with amoxicillin alone against β-lactamase negative isolates. β-lactamase-negative pathogens such as Enterococcus faecalis were more susceptible to co-amoxiclav than to amoxicillin alone [31].
In the present study, susceptibility of E.faecalis was highest towards Amoxicillin-Clavulanic acid among the different antibiotics used as it is potent bactericidal causing lysis of bacterial cell wall. The combination of Ofloxacin-Ornidazole was used for the study for two reasons:-
E.faecalis is susceptible to Ofloxacin.
Ornidazole is active against anaerobic coccus [32].
Ofloxacin, a synthetic floroquinolone inhibits the enzyme bacterial DNA gyrase, which in-turn nicks the double stranded DNA that leads to negative super-coiling of it and then again reseals the nicked end. Damaged DNA transmits signals to produce exonucleases that result in digestion of DNA depicting the rapid bactericidal action of Ofloxacin. It exhibits limited activity against gram positive bacteria and very potent activity against gram negative bacteria. Ofloxacin is resistant to majority of anaerobic bacteria and hence combined with ornidazole to treat mixed infections. Ofloxacin-Ornidazole combination is one of the routinely prescribed antibiotic in dental infections having synergistic effect against enterococci [32].
In the present study Amoxicillin-Clavulanate combination exhibited high antimicrobial efficacy compared to other drug formulations as Amoxicillin – Clavulanic acid combination showed high success rate in orodental infections compare to Amoxicillin alone and Ofloxacin-Ornidazole combination due to the growing number of bacterial resistance, as well as its broad spectrum, pharmacokinetic profile, tolerance and dosing characteristics [33]. Despite the recent introduction of many new antimicrobials, none have demonstrated significant benefit in application to oral infections justifying their replacement to penicillin derivatives, which is similar to findings of Rafael Roda et al., study by Swift et al., [34,35].
Sharma et al., used five different antibiotics i.e. Amoxicillin, Metronidazole, Azithromycin, Erythromycin, Gatifloxacin when added into endodontic sealers showed significant increase in their antibacterial properties in anaerobic & aerobic conditions. Among all the antibiotics used Amoxicillin combination showed the maximum zone of inhibition [36].
A similar study conducted by Shori et al., showed triple antibiotic paste containing Ofloxacin, Ornidazole and Amoxicillin were added to the ZOE sealer and imparted increased antimicrobial activity to the sealer [37]. The results of present study are similar with the study of Sandhya S et al., and it can be postulated that antibiotic additives may have increased zone of inhibition, i.e., antibiotic + sealer as compared to sealer alone [38].
Limitation and Recommendation
The present study has its own inherent limitations like BHI Agar was not used due to affordability and highlights the importance of using rationally the antibiotic coated gutta-percha cones while providing endodontic care in selective cases. Further clinical trials are required to understand synergistic effect of antibiotic alone with ZOE sealer and also to calculate exact dose of antibiotic required to coat the gutta-percha points.
Conclusion
Amoxicillin-Clavulanic acid combination was most effective against E. faecalis among the different combinations used. It shows that Antibiotic-coated gutta-percha potentially increase the success rate of endodontic treatment compared to conventional gutta-percha cones.
Group A-ZOE Coated GP Point Group B – ZOE+Amoxicillin-Clavulanate
Group C – ZOE+Amoxicillin Group D – ZOE+Ofloxacin-Ornidazole ** p < 0.001, HS