Triple Negative Breast Cancers (TNBC) are defined as tumours that are negative for estrogen and progesterone receptors as assessed by Immunohistochemistry (IHC), combined with lack of over-expression of HER2 when tested by IHC or absence of its gene amplification when tested by fluorescence in situ hybridization technique [1]. Hence these cancers do not respond to hormonal therapy and chemotherapy is currently the treatment of choice [2].
TNBC account for 10-20% of all breast cancers worldwide and different molecular subtypes have been identified, the basal like subtype being the most common [3,4]. The basal like subtype is associated with an aggressive clinical behaviour, present usually in younger women with early development of recurrence, distant metastasis and poor survival [5].
Gene expression profiling, the gold standard to identify the molecular subtypes of TNBC is difficult to use in routine clinical practice because of its prohibitive cost and suboptimal results obtained with paraffinized material [6]. There are no specific morphological parameters that can identify these tumours reliably by routine histology. Many studies have therefore used basal immunohistochemical markers as a surrogate to identify the basal like subtype [7]. These markers permit identification of the basal like subtype at an affordable cost with feasibility of use in routine clinical practice and without the need for fresh tissue [6,8,9].
This study was undertaken to assess the frequency and evaluate the clinico-pathological features of TNBC in our institution. We used three immunohistochemical markers as a surrogate for gene expression profiling, to classify TNBC into basal and non-basal subtypes. We studied in detail the morphological features of both basal and non basal like subtypes.
In addition we also attempted to classify TNBC into four prognostically different histological subtypes as described by Ishikawa et al., [10]. The immunohistochemical and histological classifications were also correlated with disease free and overall survival outcomes.
Materials and Methods
This study was approved by the institutional review board with waiving off the need for informed consent as fresh frozen paraffin embedded tissues of a retrospective cohort of patients were used for the study. A total of 238 cases of primary invasive breast carcinomas diagnosed between the periods January 2010 to June 2011, in the department of pathology in our institution were screened for 3 IHC markers, ER, PR and HER2. Of these 238 cases, 53 cases were found to be triple negative for ER, PR and HER2 and were included in the study. Cases with insufficient tissue sample required for performing further IHC were excluded.
The clinical details were obtained from the hospital records through the electronic database and patient charts from the medical records. The clinical features analysed included age, sex, size, side, quadrant of tumour involvement, chemotherapy status, clinical staging, metastasis, family history and treatment received.
The histomorphological features were studied in detail. The cases in our study were classified according to Ishikawa subtypes of TNBC [10] as follows: Type A- “atypical” medullary carcinoma, Type B- carcinoma with a central acellular zone, Type C- other invasive ductal carcinomas, Type D- special types.
Density of lymphocytic infiltration was graded as mild, moderate and marked according to Thike et al., [11]. Tumours with up to one-third of lymphocytic infiltration were graded as mild, one-third to two-thirds as moderate and more than two thirds was graded as marked. Amount of cytoplasm was assessed depending on the Nucleo-Cytoplasmic (N/C) ratio [12].
Three IHC markers, CK5/6, CK14 and EGFR [Table/Fig-1] were used to categorize these tumours into basal and non-basal subtypes. More than 1% tumour cells staining for any one of these markers was considered as positive [13].
Antibody clones used for Immunohistochemical markers.
| Antibody | Clone | Dilution | Source | Pre-treatment |
|---|
| EGFR | E30 | 1:50 | Dako M7239 | Pressure cooking |
| CK5/6 | D5/16B4 | 1:100 | Dako M7237 | Pressure cooking |
| CK14 | LL002 | 1:20 | NovocastraNCL- LL002/Biogenex | Pressure cooking |
Overall and disease free survival of TNBC and of basal and non-basal subtypes was performed using the Kaplan Meier survival analysis [14].
Results
Fifty three (22.2%) cases were found to be negative for ER, PR and HER2. The microscopic features were analysed in 52 of 53 cases as in 1 case the paraffin embedded block was received as a consult case and returned to the patient after diagnosis.
Type of specimen: Of 53 cases of TNBC, 35 cases (66%) were of modified radical mastectomy specimens, 4 cases (7.5%) were of lumpectomy, 1 case (2%) was a wedge biopsy, 7 cases (13.2%) had only a trucut biopsy and the remaining 6 cases (11.3%) were received as consultation from other hospitals.
Clinical features [Table/Fig-2]: The mean age (with standard deviation) of TNBC patients in our present study was 46±12 years. The youngest patient with TNBC was 23-year-old and the oldest patient was 79-year-old. The average size of tumour was 4.3 cm and 53% of cases presented with stage III and IV disease. There was no statistically significant difference in the laterality of breast involvement.
Clinicopathological features of triple negative breast carcinomas.
| Parameters(N=number of cases) | Percentage (%) |
|---|
| Age(N=52) | 46±12 years |
| Size(N=33) | 4.3±2.56cm |
| Staging(N=47) IIIIIIIV | 9383815 |
| WHO subtype(N=52)Invasive ductal carcinomaOther subtypes | 964 |
| Histologic grading(N=49)Grade IIGrade III | 4357 |
| Tumour borders (N=45)PushingPushing and infiltrativeInfiltrative | 383131 |
| Tumour infiltrating lymphocytes(N=52)AbsentMildModerateMarked | 2543311 |
| Shape of cells(N=52)PolygonalSpindle | 982 |
| Type of chromatin(N=52)HyperchromaticVesicularHyperchromatic and vesicular | 372835 |
| Nucleoli(N=52)InconspicuousPresent, but not prominentProminent | 83557 |
| Amount of cytoplasm(N=52)ModerateAbundant | 8713 |
| Nucleo-cytoplasmic ratio(N=52)LowHigh | 298 |
| Amount of intratumoural stroma(N=52)ScantMildModerateAbundant | 4425274 |
| Necrosis and central acellular sclerosis (N=52)NecrosisAbsentPresentCentral geographic necrosis(N=52)AbsentPresent | 96498 |
| Central acellular sclerosis without necrosis (N=52)AbsentPresent | 28812 |
| Squamous metaplasia(N=52)AbsentPresent | 946 |
| Other Metaplasia(N=1) | 2 |
| Ductal carcinoma in situ(N=52)AbsentPresent | 6733 |
| Lymphovascular invasion(N=52)AbsentPresent | 3169 |
| Ishikawa subtypesType A(Atypical medullary carcinoma)Type B (Carcinoma with central acellular zone)Type C (other invasive ductal carcinoma)Type D (Special types) | 1514674 |
WHO subtype: Ninety-six percent cases were classified as invasive ductal carcinoma, Not Otherwise Specified (NOS).
Histological grading: Modified Bloom-Richardson histological grading [15] was done only in 49 cases because mitotic activity could not be assessed in 3 cases. None of the cases was found to be of grade 1 [Table/Fig-2].
Borders: Majority of TNBC cases, 37.8% had a predominantly pushing border, 31.1% had both infiltrating and pushing borders and 31.1% had infiltrating border.
Tumour infiltrating lymphocytes: Ninety-eight percent cases of TNBC had lymphocytic infiltrate out of which 54% had mild infiltrate, 33% had moderate infiltrate and 11% had dense infiltrate.
Cytological features of TNBC: Ninety-eight percent cases had polygonal cells, 2% had spindle shaped cells, 72% had hyperchromatic nuclei, 57% had prominent nucleoli, 87% had moderate amounts of cytoplasm and 98% of cases had high N/C ratio.
Necrosis and central acellular sclerosis: Necrosis was present in 4% cases. Only 1 case showed central geographic necrosis. Central acellular sclerosis without necrosis was seen only in 12% of cases.
Metaplasia in TNBC: Three out of 52 cases (6%) of TNBC had shown focal squamous differentiation. Of these 3 cases, 1 case also showed syncytiotrophoblasts with bizarre giant cell formation.
Ductal Carcinoma In Situ (DCIS) in TNBC: Seventeen out of 52 cases (33.3%) of TNBC had an associated DCIS component. Of these 17 patients with DCIS, 8 (47%) cases were found to be triple negative of which 3 cases were found to be basal like both in DCIS and invasive component.
Lymphovascular invasion: It was seen in 69% cases.
Ishikawa subtype: TNBC were classified according to the Ishikawa subtypes. Invasive ductal carcinoma NOS (Type C -67%) was found to be the commonest subtype, followed by “atypical medullary carcinoma” (type A -15%), carcinoma with central acellular zone (type B-14%) and special type (type D -4%).
Immunohistochemical findings: Three markers, CK14, CK5/6 and EGFR were used on 47 cases to identify the basal like subtype in TNBC. 35 cases (74.4%) were classified as basal like subtype based on positivity for any one basal marker. A total of 24 (51%) were found to be positive for CK5/6, 17 (36%) were positive for CK14 and 29 (62%) were positive for EGFR [Table/Fig-3].
Cases positive for individual markers.
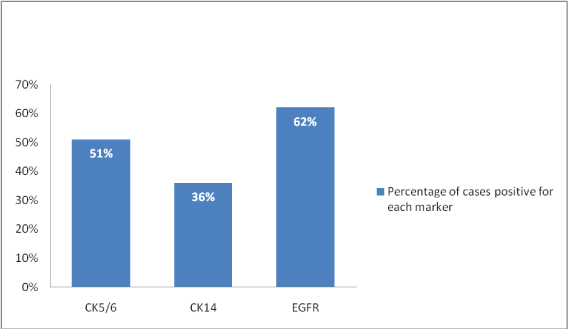
EGFR as a single marker picked up the maximum number of cases of basal like subtype of TNBC.
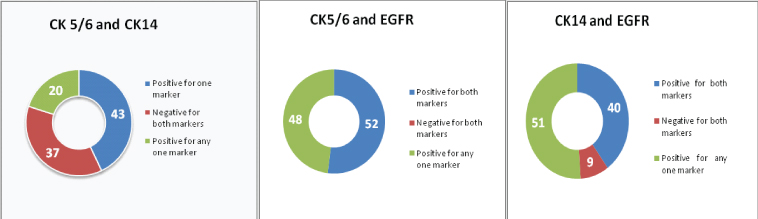
The combination of CK5/6 and EGFR picked up all cases of basal like subtype (100%) as compared to the combinations of CK5/6 and CK14 (80%) and CK14 and EGFR (91%) [Table/Fig-4].
Combination of two markers to identify TNBC.
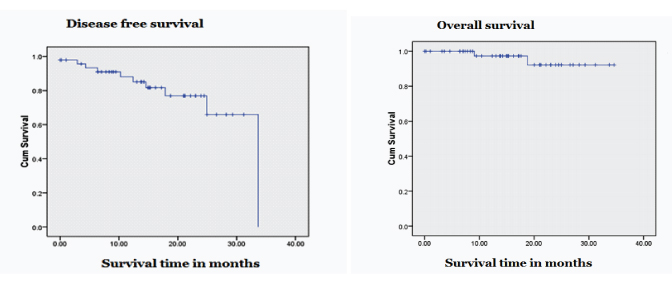
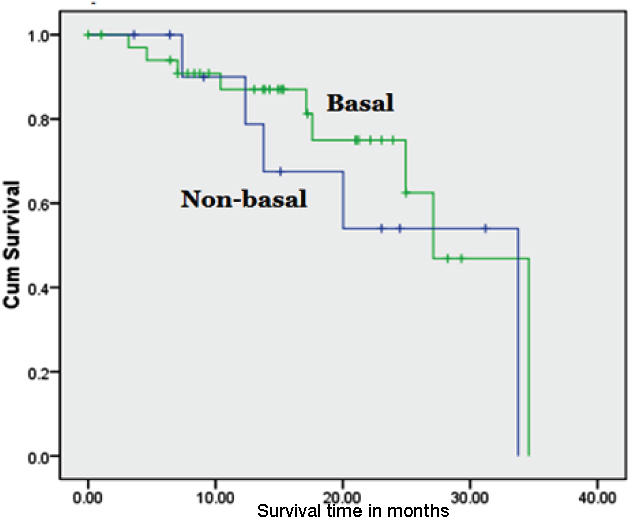
In our study, the only clinical parameter which showed statistical significance was the size of tumours, which was found to be larger in the basal type (p-value: 0.023). There was no significant difference in the microscopic features between basal and non- basal TNBC, except for the amount of cytoplasm (p-value: 0.049) [Table/Fig-5]. In our study, follow up was done for a period of 1.5 years up to 3 years. The median disease free survival for TNBC was 27 months and the median overall survival was 33 months [Table/Fig-6]. There was no significant difference in survival outcomes between basal and non- basal TNBC [Table/Fig-7].
Comparison of clinico-pathological features in basal and non basal TNBC.
| Parameters | Basal Numberof cases (%) | Non-basalNumber ofcases (%) | p-value |
|---|
| Age: Mean(SD) | 47.29(46.17) | 12.21 (10.21) | 0.78 |
| Age< 40 years> 40 years | 8(24)26(76) | 2(17)10(83) | 0.93 |
| Family historyPresent | 3(12) | --- | 0.81 |
| Size<1cm1-2cm>2cm | ---14(52)13(48) | 2(25)4(50)2(25) | 0.023 |
| Lymph node involvement | 28(80) | 9(75) | 0.644 |
| TubulesNo tubules<10%10-75%>75% | 7(20)23(66)5(14)--- | 5(42)5(42)2(16)--- | 0.28 |
| Nuclear pleomorphismModerateMarked | 28(80)7(20) | 11(92)1(8) | 0.63 |
| Shape of cellsPolygonalSpindle | 34(97)1(3) | 12(100)--- | 1.00 |
| ChromatinHyperchromaticVesicularHyperchromatic and vesicular | 12(34)10(29)13(37) | 4(33)4(33)4(33) | 0.95 |
| NucleoliInconspicuous/absentPresentProminent | 2(6)11(31)22(63) | 1(8)4(34)7(58) | 0.93 |
| Cytoplasmic amountModerateAbundant | 33(94)2(6) | 8(67)4(33) | 0.04 |
| Mitotic rate<1010-40>40 | 6(17)18(51)11(32) | 5(42)7(58)--- | 0.09 |
| Squamous metaplasiaPresent | 3(8.5) | --- | 0.72 |
| Other metaplasiasPresent | 1(3) | --- | 1.00 |
| NecrosisPresent | 28(80) | 6(50) | 0.10 |
| Central acellular sclerosisPresent | 5(14) | 1(8) | 0.97 |
| DCISPresent | 13(37) | 3(25) | 0.68 |
| Lymphocytic infiltrateAbsentMildModerateMarked | ---20(57)11(31)4(12) | 1(8)6(50)3(25)2(17) | 0.35 |
| Lymphovascular invasionPresent | 25(71) | 9(75) | 1.00 |
| WHO subtypeInvasive ductal carcinomaOthers | 33(94)2(6) | 11(92)1(8) | 1.00 |
| Histological gradeGrade IIGrade III | 16(46)19(54) | 5(50)5(50) | 0.55 |
| Ishikawa subtypesType AType BType CType D | 6(17)6(17)22(63)1(3) | 1(8)1(8)9(76)1(8) | 0.62 |
Disease free and overall survival outcomes in TNBC cases.
Disease free and overall survival outcomes in TNBC cases basal TNBC.
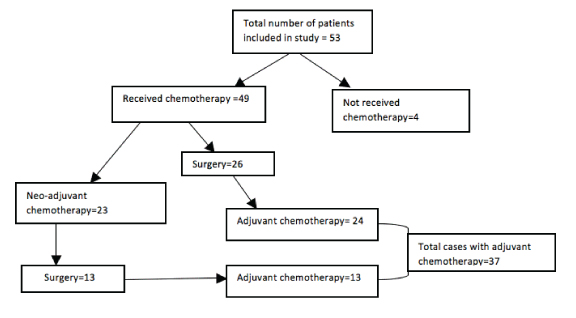
Treatment and follow up: Treatment given is depicted in [Table/Fig-8]. Anthracycline and taxane based chemotherapy was given to all 49 patients. 22 patients received radiotherapy.
Disease free and overall survival outcomes in TNBC cases.
A total of 12 patients presented with metastases, which included 5 of basal and 5 non-basal types and the remaining 2 cases did not have basal markers done due to paucity of tissue. 11 patients relapsed with metastases, of which 7 were of basal type and 3 of non-basal type. Only 1 case did not have basal markers done. The sites for metastases are shown in [Table/Fig-9]. There was no evidence of residual disease in 23 patients, 2 patients had died and 11 patients were lost to follow-up.
Metastases in basal and non basal TNBC.
| Basal (Number of cases) | Non-basal (Number of cases) |
|---|
| Sites of metastasesat presentation | Liver and lung (1)Liver (1)Bone marrow (1)Skin (1)Lymph nodes (1) | Lymph nodes (2)Skin (1)Chest wall (1)Bone marrow and lung (1) |
| Sites of metastasesafter presentation | Ovary (1)Lung (2)Skull (1)Brain, bone marrowand chest wall (1)Lymph node(1)Chest wall and lung (1) | Brain and bone marrow (1)Lymph node and lung (1)Bone marrow |
Discussion
Only few Indian studies on TNBC including the basal like subtype have been published. There is a need to identify these tumours because of its aggressive behaviour, bad prognostic and treatment outcomes as shown in literature [16–23].
The frequency of TNBC in our institution constituted 22.2%. Studies from different parts of the world have shown a varying frequency of 10-20%. Studies from India have shown a slightly higher range, 11.8% to 31.9% [16–24]. The incidence is lower in studies from other parts of Asia, including Korea (14.7%), China (12.6%) and Japan (8.4%) [25–27]. TNBC are more frequent in African Americans (26.5%) and in African women (34%) when compared to Non-African Americans (16.0%) [28].
TNBC patients are usually less than 40 years as compared to the non TNBC [29]. Our study did not show any statistical significance (p-value = 0.776) in age between basal and non-basal subtypes. The average size of TNBC in our study was 4.3± 2.56 cm. There was significant difference in tumour size between basal and non-basal tumours in our study (p-value = 0.023), which is also similar to previous studies [28–30]. Positive family history of breast carcinoma was seen only in the basal like subtype.
The most common histological subtype in our study was that of infiltrating ductal carcinoma (NOS), similar to other studies [2–5,31]. In the present study, 3 cases (6%) showed focal squamous cell differentiation. All cases in our study were classified as grade II or III and none were classified as grade 1. There was no significant difference between basal and non-basal TNBC (p-value = 0.546), in congruence with literature [29,30,32].
Majority (37.8 %) of our cases had a predominantly pushing border, 31.1% had both pushing and focally infiltrating borders and 31.1% cases had an infiltrating border. Most studies have shown TNBC to have a pushing non-infiltrative border of invasion [29,32].
Central acellular sclerosis was seen in 12% of TNBC cases as compared to 27.9% in a study done by Choi et al., [33]. Central acellular sclerosis and necrosis was more common in basal (14% and 80%) than non-basal (50% and 8%), but was not statistically significant.
In our study, 98% cases had shown lymphocytic infiltrate, of which 54% had mild infiltrate, 33% had moderate infiltrate and 11% had a marked infiltrate. There was no statistically significant difference in the degree of lymphocytic infiltrate between basal and non-basal tumours (p-value-0.346). Literature has shown that most TNBC cases with a dense lymphocytic infiltrate either intra-tumoural or within the vicinity of the tumour [29,32].
Of 17 cases of DCIS in our study, 8 (47%) cases were found to be triple negative, of which 3 cases were found to be basal like, both in the DCIS and invasive components. Literature has shown that TNBC and basal like cancers often lack an in-situ component due to rapid disease progression [32]. Ishikawa et al., found 29 cases (30%) of DCIS out of 97 cases of TNBC [10]. Thike et al., found 295 (45.2%) cases of DCIS out of 653 TNBC cases [34]. Doval et al., found 35.6% cases of DCIS among TNBC cases [35].
In our study, majority of TNBC had a Type C (67.3%) pattern which corresponds to invasive ductal carcinoma (NOS) according to Ishikawa classification. There was no statistically significant difference in the Ishikawa histological types between the basal and non-basal subtype (p-value-0.623).
Of 53 cases of TNBC in our study, 35 cases (74.4%) were of basal like subtype. Studies show the basal like subtype to be the most common in TNBC. Bertucci et al., identified 71.5% basal like subtypes among TNBC [36]. Rakha et al., used a combination of 4 basal markers and identified 71% of basal like types among TNBC [37].
The combination of CK5/6 and EGFR in our study identified all basal like TNBC cases. Nielsen et al., used a panel of 4 markers, ER, PR, EGFR, CK5/6 to identify basal subtype and found a sensitivity and specificity of 76% /100% [6]. Similarly, Thike et al., used a panel of 3 markers, CK14, EGFR, 34ße12 and found a sensitivity and specificity of 78%/100% [8]. Majority of TNBC are found to over-expresses EGFR and could respond to anti-EGFR therapies [37–39].
Similar to findings of Rakha et al., our study also has not shown any significant morphological differences between basal and non basal subtypes except for the amount of cytoplasm (p-value= 0. 49) [40].
TNBC are associated with a worse prognosis, develop early and are seen more often in premenopausal women. A characteristic peak of recurrence is seen within first 3 years after initial treatment and declines rapidly thereafter. In contrast, in ER positive breast cancers, more than 50% of recurrences are seen between 5 and 10 years after the first surgery. After 5 years of therapy the survival rates equals those of the non-TNBC subtypes. This suggests that the poor prognosis of TNBC may be due to effects that occur during the first 5 years after surgery [37–39].
TNBC are characterized by higher relapse rates compared to ER positive breast cancers, including an increased risk of loco-regional recurrence, lung, and brain involvement, but lesser risk for recurrence in bone. After metastatic relapse, survival is shorter in TNBC compared to other subtypes, due to their predilection for visceral and lung metastasis compared with ER-positive breast cancers that are more likely to relapse in bone and skin [37–39].
Limitation
The sample size of our cases was relatively small due to a short study period. A few cases in our study were received as consults without paraffin blocks. Therefore basal immunohistochemical markers could not be performed on those cases. Survival of Ishikawa subtypes in basal and non- basal TNBC could not be analyzed due to small numbers in each subtype.
Conclusion
Frequency of TNBC in our institution was found to be 22.2%. Identifying TNBC, only by the use of ER, PR and HER2 is not enough, as the poor prognostic outcomes in TNBC is mainly accounted by the basal like subtype, which dominates the majority of TNBC.
Our study has demonstrated that high grade morphological features, hormonal markers with additional use of basal markers can help identify the basal like subtype of TNBC, thereby predicting breast cancer survival. The combination of CK5/6 and EGFR identified all cases of the basal subtype. EGFR in addition also has potential therapeutic implications and can benefit these patients.