Piper et al., defined fatigue as “A subjective feeling of tiredness that is influenced by circadian rhythms and can vary in unpleasantness, duration and intensity [10]. Pharmacological treatment for fatigue may sometimes not have satisfactory effects or may cause side effects [11].
In recent years, researchers investigated the role of alternative medicine methods such as acupuncture in the treatment of the chronic diseases [12,13]. Acupuncture is a Chinese ancient medicine in the orient over 2500 years ago. According to the Chinese medicine theory, the human body thrives upon Chi energy which travels along pathways at differing depths of the body known as meridians. Along the meridians are points known as acupoints, which are pumping stations for the chi energy. Fatigue is caused by deficiency or imbalance in life energy (Qi). Applying acupuncture into these points can relieve imbalances by either stimulating or easing the energy flow. Stimulation of the acupoint rectifies qi, stabilizes the body, strengthens bodily functions, and cures disease. This method can be administered by a health care provider or by patients themselves [13,14].
Electroacupuncture (EA) is the newer method of acupuncture that can be more effective than manual acupuncture in the treatment of various type of diseases [15]. Trans Cutaneous Electrical Acupoint Stimulation (TEAS) is an alternative method of acupuncture was suggested by Xing et al., [16]. TEAS is non-invasive, as it does not involve the actual insertion of needles into the body. This method had comparable effects to acupuncture therapy [17]. Therefore, there is a minimal risk with TEAS and it may be suitably applied in ESRD patients. TEAS has been used to treat various clinical conditions, with reports indicating that TEAS appears to be effective in reducing post-operative nausea, vomiting and improvement of fatigue, quality of sleep and depression in haemodialysis patients [17,18]. The findings of other study have shown that on applying acupuncture in cancer patients they could improve fatigue after chemotherapy by 36% [19]. Despite this significant symptom of fatigue in the ESRD patients, no interventional studies have addressed this problem in Iran. Therefore, the current study aimed to evaluate the effects of TEAS on fatigue of ESRD patients who have undergone haemodialysis treatment.
Materials and Methods
This study was done as a single-blind clinical trial, from two dialysis centers in major hospitals in Ahvaz-Iran during 6 months from February to July of 2009, population was chronic haemodialysis patients who admitted to haemodialysis center in Imam Khomeini and Golestan hospitals to perform haemodialysis treatment program. Fifty six participants receiving haemodialysis were recruited as random [Table/Fig-1]. Inclusion criteria were adults aged 15 and above, diagnosed with ESRD, had been treated with haemodialysis for at least 3 months and complained of fatigue. The patients with a lower extremity amputation, having the pacemaker, complications requiring immediate medical intervention, under the psychological medications, hospital admission for any other reason, needed a blood transfusion, surgery, having infection and bleeding were excluded from the study. Patients meeting the inclusion criteria were divided into two groups namely, TEAS (10 females, 18 males) and TEAS-Sham group (8 females, 20 males). TEAS group treated by acupuncture in real points, while, in the TEAS-Sham patients, based on the acupuncture expert opinion, the procedure was implemented for them in the false points, so that the patients were not aware of their grouping and blinded about it.
Flow diagram of the study process.
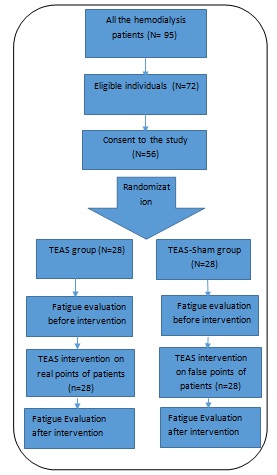
Written informed consent was obtained from all patients before the study. About the study, it was single-blind, sham-controlled, randomized clinical trial that conducted over a six month period. After consenting to participate, subjects were randomly assigned into two groups (TEAS and Sham).
Instrument
The tools were a checklist of demographic and clinical characteristics and the fatigue scale; Clinical and demographic characteristics of patients consisted of age, sex, level of education, cause and duration of ESRD, blood urea and creatinine according to the latest laboratory results. The Brief Fatigue Inventory (BFI) was used to determine the fatigue rate of the patients [20]. BFI is included 10 questions and each of these questions (except the first one) was measured by a scored scale (from 0 to 10) with higher scores indicating more fatigue. In this Scale 0 means without fatigue; 0.1 – 3.9 means mild; 4 – 6.9 means middle; 7 – 9.9 means severe and 10 means critical fatigue. BFI scale covered five areas of fatigue including fatigue in the last week, fatigue right now, usual level of fatigue during past 24 hours and worst level of fatigue during past 24 hours, How during the past 24 hours, fatigue has interfered with general activity, mood, walking ability, normal work, relations with other people, enjoyment of life, and finally general fatigue were measured. A cross-sectional study was conducted among 249 Chinese cancer patients with multiple diagnoses to validate a Chinese version of the Brief Fatigue Inventory (BFI-C). In the study in Italy Cronbach’s coefficient alpha was 0.92 for fatigue severity items and 0.90 for fatigue interference items. The BFI-I had an overall Cronbach alpha for the nine items of 0.94. The inter-item mean correlation was 0.64, and coefficients ranged from 0.47 to 0.81 for the nine items [21,22].
Intervention
Three acupoints were selected for TEAS treatment after consultation with acupuncturists. These acupoints included, ST36 (Zusanly), below the knee, in the anterior boarder of tibia; SP6 (Sanyinjiao), above the tip of the medial malleolus and posterior to the medial border of the tibia; LI4 (Hegu), on the dorsum of the hand between the first and second metacarpal bones [23]. The sham pseudo-TEAS treatment followed the same protocol as the TEAS treatment except for the positioning of the points electro-stimulation. This arrangement avoided placing the pseudo electrodes on true meridians or acupoints. As noted in the device guideline and its instruction brochure, Acupuncture points were found by an Acupoint finder Electrical Stimulation. Electrical stimulation was applied with Acuhealth (Australia) electrical impulses with Frequency 2.5 Hz and Intensity 500 microamps into 500 Ohms. The time of intervention for all patients was limited to 5 minutes of TEAS (50 seconds per acupoint) six acupoints bilaterally for 10 sessions. Treatments were given 2-3 times per week for 5 consecutive weeks.
Data Collection
Data was gathered with referring to the haemodialysis centers, after explaining the aim and objective of the study, the questionnaires were filled up by the researcher before and after 10th session of intervention. TEAS intervention performed 2 hours after beginning of dialysis treatment session. The study lasted from February to July of 2009.
Ethical consideration
This study was approved by vice-chancellor (with No. 88040) and ethics committee (with approval NO. 1052) of Ahwaz University of medical sciences. The written informed consent was taken from the patients and they were assured of the benefits of the intervention, as well as the anonymity and confidentiality of private information.
Data Analysis
Data was analysed by using The SPSS (Version 16.0) statistical software package and descriptive and inferential statistics, the test included independent and paired t-test, Mann-Whitney and Wilcoxon tests. Kolmogorov-Simonov was used for determining the normality of quantitative variables. The significant level of all statistical analyses was set at p<0.05.
Results
In this study 95 patients were screened, 72 patients met the inclusion criteria and 60 patients agreed and consented to the study. Four patients were excluded over the intervention: 2 in the TEAS group and 2 in the sham group. Finally, 56 cases including 28 cases in the TEAS group and 28 cases in the Sham group completed the research [Table/Fig-1].
Of the 56 patients 38 participants (67.9%) were male and 45 (80.4%) married. The mean and standard deviation of age were 52.29±15.26 years, and 37.5% (21 individuals) of the cases had an education level of elementary school and junior high school. The mean length of dialysis was 32.96±39.28 months. Fifty cases (89.3%) didn’t have a history of kidney transplantation.
The most common causes of renal failure were hypertension (14 people, 25%), diabetes mellitus (11 people, 19.6%) and urologic disorders (9 people, 16.1%). There were no differences in the clinical and the demographic characteristics of patients among two groups (p > 0.05). The clinical and demographic characteristics of patients who completed in this study were listed in [Table/Fig-2].
Demographic and clinical characteristics of study participants.
| TEAS group(n=28) | Sham group(n=28) | p-value |
|---|
| Variables | Mean±SD | Mean±SD | |
| Age | 48.15±15.5 | 56±14.6 | 0.068 |
| Urea (mg/dl) | 56.6±18.8 | 51.1±17.2 | 0.25 |
| Mean rank | Mean rank | |
| Months of Dialysis | 25.61 | 31.39 | 0.184 |
| Creatinine(mg/dl) | 24.32 | 32.68 | 0.055 |
| Number (%) | Number (%) | |
| Gender (Male/Female) | 20/8 (71.4/ 28.6) | 18/10 (64.3/35.7) | 0.73 |
| Married | 22 (78.6) | 23 (82.1) | 0.73 |
| A history of kidneytransplantation | 2 (7.1) | 4 (14.2) | 0.66 |
| Education |
| Uneducated | 14(50) | 5(17.9) | 0.99 |
| Elementary and juniorhigh school | 6(21.4) | 15(53.6) |
| Senior school and above | 8(28.6) | 8(28.6) |
| Aetiology |
| Hypertension | 6(21.4) | 8(28.5) | 0.53 |
| Diabetes mellitus | 6(21.4) | 5(17.9) | 0.73 |
| Urologic | 4(14.3) | 5(17.9) | 0.71 |
| Hypertension andDiabetes mellitus | 6(21.4) | 1(3.6) | 0.10 |
| Other reasons | 6(21.4) | 9(32.1) | 0.36 |
The mean of pretest score for general fatigue in the revised Brief BFI for the subjects was 4.33± 2.2. This rate was 4.48±1.5 about the TEAS and 4.17±2.7 to Sham groups, which the mean rank of them was not different statistically (p=0.317, Z=1.00). The results of the Mann-Whitney U test indicated that there were significant differences between the Mean rank of the TEAS and Sham groups (p= 0.002) after intervention. Descriptive statistics of fatigue mean rank for the pre-test and post-test for each group are presented in [Table/Fig-3].
Comparison of fatigue between two groups before and after intervention.
| groups → | TEAS group(n=28) | Sham group(n=28) | Statistical tests |
|---|
| time ↓ |
|---|
| Fatigue | Mean rank | Mean rank | p=0.317Z=1.00 |
| Before | 30.68 | 26.32 |
| After | 21.68 | 35.32 | *p=0.002Z=3.13 |
| p-value | *p<0.001 | p=0.731 |
| Z=4.327 | Z=0.343 |
*it is significant
Discussion
The findings revealed the application of TEAS method had produced a better recovery rate of fatigue in these patients. The research results showed that fatigue is a major concern for haemodialysis patients. Participants in the study displayed a moderately severe level of fatigue. These results similar to other studies which indicated moderate feelings of fatigue in haemodialysis patients [24,25]. These findings support the assertion that moderate feelings of fatigue exist commonly in haemodialysis patients.
Our findings revealed application of the TEAS on LI4 (Hegu), ST36 (Zusanly) and SP6 (Sanyinjiao) that had produced a better recovery rate of fatigue in TEAS group than Sham group after a course of ten sessions intervention. This difference in improvement may be mainly due to the effect of TEAS on these various acupoints. The results from this study suggest that TEAS might have an important role in managing fatigue symptoms in patients with ESRD.
There are few studies about the effects of TEAS on fatigue in haemodialysis patients. Tsay reported that TEAS significantly reduces the level of fatigue in haemodialysis patients [17] that is consistent with our study. Results of this study also are consistent with other studies that have shown the effects of acupuncture methods such as TEAS in improving fatigue for patients with chronic illnesses especially cancer [26,27].
TEAS techniques are non-invasive, safe and effective. Health professionals, patients and their families can be easily trained to administer TEAS so that they can manage fatigue, thus decreasing adverse health outcomes and improve their quality of life [28].
Results of this study showed that prevalence of ESRD in men is more than in women, which similar to findings of other studies were done by Kazemi and Sabouhi [29,30]. This may attribute to the differences in men and women physiology, as well as affected risk factors such as obesity, diabetes and cardiovascular diseases [31]. The most aetiologic agent of ESRD in this study was hypertension and diabetes, respectively. This result consistent with other studies as conducted by Tsay and Sabouhi [17,30]. But in all results of this study, there were no differences in the clinical and the demographic characteristics of patients among two groups.
Limitation
Although, the results showed that the effects of TEAS on the improvement of fatigue in haemodialysis patients, however, the sample was drawn from two dialysis centers in Ahvaz, southwest of Iran. Generalizability of these findings to other samples of dialysis patients from other geographical areas in Iran cannot be ensured. Other limitation is related to non-registry in IRCT, because our project was conducted in 2009, and in that time, the registration was optional for the universities, so, my research has not been enrolled in the IRCT. However, we took the permission from the ethics committee of Ahvaz Jundishapur University of Medical Sciences.
Conclusion
The results of this study showed the TEAS procedure could reduce the fatigue level of ESRD patients, so, it is suggested that the method would be applied in the haemodialysis units, hereof, more studies need to be done to consolidate a standardized method and maximize the effectiveness of TEAS. Future research should include the identification of the most effective acupoints and the mechanism behind it. In addition, other variables such as optimal electrode size, electrical power and frequency, waveform, stimulation duration should be investigated.
*it is significant