Materials and Methods
Detailed history was taken and age, sex, BMI, blood pressure were documented. Complete blood count, renal function test and lipid profile of all the patients were done in the institute laboratory by standard methods.
CAD was defined as patients with angiography proven stenosis of ≥50% in one or more major coronary arteries [21]. These major arteries are left anterior descending artery, left main, left circumflex artery and right coronary artery with right dominant, balanced, or left dominant circulation. The angiography findings was reported as normal coronary artery, insignificant CAD, significant CAD with severity for coronary artery stenosis in the form of 50% to 100% or complete cut-off. In this study angiographic normal and insignificant CAD were included in the normal coronary artery group. The maximum severity of stenosis was considered as final. The severity of stenosis was graded as 50%-70%, >70%-90% and >90%. The number of vessels involved were analysed separately.
Serum 25-hydroxyvitamin D (vitamin D) was measured by Electrochemiluminescence immunoassay (ECLIA) in overnight fasting blood sample, one day prior to the coronary angiography. The intra and inter-assay CVs ranged between 5%-10%. Serum vitamin D level was graded as, normal (>30ng/ml), insufficiency (20-30ng/ml) and deficiency (<20ng/ml) [10]. The severity of vitamin D deficiency was further graded as, moderate deficiency (>10-<20ng/ml), severe deficiency (>3-10ng/ml) and very severe deficiency (≤ 3ng/ml).
Statistical Analysis
Sample size was calculated based on previous study which showed prevalence of vitamin D deficiency around 80% in patients with CAD [22]. Our sample size came out be 246 at a power of 80% and 95% confidence interval. For possible high dropout and to get the desired number of patient with CAD, 315 patients were recruited. The continuous data was represented as mean (±SD) unless otherwise stated, while the categorical data was represented as proportions. Data were analysed using SPSS software package. Parametric data was analysed using unpaired T- test and ANOVA for two and more than two groups and for categorical, nonparametric data Chi-Square test was applied. Mann-Whitney test was used to compare the variables that were not normally distributed. A two-sided p-value of <0.05 was considered as statistically significant with 95% confidence interval.
Results
Baseline Data of the Study Population: Among 315 patients, 75 (23.80%) had normal coronary arteries and 240 (76.20%) had CAD. Out of 240 patients with CAD, 21 (6.70%) had 50%-70% stenosis, 95 (30.20%) had >70% -90% stenosis and 124 (39.40%) had >90% stenosis. According to the number of vessel involved, 70 patients (22.20%) had single vessel disease, 85 (27.00%) had double and 85 (27.00%) had triple vessel disease.
The mean age and BMI of the study population were 54.50 (± 9.50) years and 25.50 (± 3.60) Kg/m2 respectively. The mean age (p=0.10), BMI (p= 0.36), haemoglobin (p=0.48), calcium (Ca) level (p=0.71) and lipid profile (p=0.64) were not significantly different between the study groups [Table/Fig-1].
Base line data of the study population.
| Base line data | Population(N= 315) | Normal coronary (N=75) | CAD (N= 240) | 50-70% stenosis (N= 21) | >70-90% stenosis (N= 95) | > 90% stenosis (N= 124) | p-value |
|---|
| Age (years) | 54.50(9.50) | 52.30 (9.00) | 55.30(9.50) | 55.50(8.50) | 55.70(9.20) | 54.80(10.00) | 0.10 |
| Male (%) | 247(78.40) | 42(56.00) | 205(85.40) | 18(85.70) | 79(83.10) | 108(87.10) | 0.001 |
| Female (%) | 68(21.60) | 33(44.00) | 35(14.60) | 3(14.30) | 16(16.90) | 16(12.90) |
| BMI(Kg/m2)(± SD) | 25.50(3.60) | 26.00(3.70) | 25.30(3.50) | 24.60(3.90) | 25.40(4.00) | 25.40(3.10) | 0.36 |
| Smoker (%) | 99(31.40) | 15(15.10) | 84(84.80) | 5(5.00) | 34(34.30) | 45(45.50) | 0.04 |
| Non-smoker (%) | 216(68.60) | 60(27.80) | 156(72.20) | 16(7.40) | 61(28.30) | 79(36.60) |
| Alcoholic (%) | 83(26.30) | 19(22.90) | 64(77.10) | 2(2.40) | 28(33.70) | 34(41.00) | 0.32 |
| Nonalcoholic (%) | 232(73.60) | 56(24.10) | 176(75.90) | 19(8.20) | 67(28.90) | 90(38.80) |
| Hypertensive (%) | 232(73.70) | 49(65.30) | 183(76.30) | 11(52.40) | 73(76.90) | 99(79.80) | 0.02 |
| Non hypertensive | 83(26.30) | 26(34.70) | 57(23.70) | 10(47.60) | 22(23.20) | 25(20.20) |
| Diabetic (%) | 72(22.80) | 11(15.30) | 61(84.70) | 8(11.10) | 23(32.00) | 30(41.70) | 0.38 |
| Non diabetic | 243(77.10) | 64(26.30) | 179(73.70) | 13(5.30) | 72(29.60) | 94(38.70) |
| Dyslipidemia (%) | 55 (17.5) | 16 (21.3) | 39 (16.2) | 3 (14.3) | 15 (15.8) | 21 (16.9) | 0.64 |
| Hb (g/dl) (± SD) | 14.00(5.80) | 13.30(0.80) | 14.20(6.60) | 13.60(0.8) | 13.80(0.7) | 14.60(9.20) | 0.48 |
| Ca (mg/dl) (± SD) | 9.20(0.7) | 9.24(0.9) | 9.22(0.8) | 9.32(0.5) | 9.15(0.5) | 9.18(0.8) | 0.71 |
The frequency CAD and severity of CAD were not significantly different [Table/Fig-1] in diabetic or non-diabetic (p= 0.38) and alcoholic or non-alcoholic (p= 0.32). In our study [Table/Fig-1] as compared to female (21.60%), male (78.40%) had more severe CAD according to severity of stenosis and as well as the number of vessels involved (p=0.001). According to our study the patients with history of smoking and hypertension [Table/Fig-1] both had more severe CAD according to the angiographic percentage of stenosis, as compared to the patients without history of smoking (p= 0.043) and hypertension (p=0.020). The details of these observations are beyond the scope of discussion in this article.
Vitamin D level: The mean serum vitamin D level of 315 patients was 13.40ng/ml (±10.40) with minimum value of ≤3ng/ml and maximum value of ≥70ng/ml. There was no statistically significant difference in the vitamin D level of different age groups, 11.20ng/ml (±5.90), 14.10ng/ml (±11.20), 11.30ng/ml (±7.40) and 15.10ng/ml (±12.20) in 30-39 years, 40-49 years, 50-59 years and 60-70 years age groups respectively (p=0.151). The mean vitamin D levels were similar in male and female (p=0.73), smoker and non-smoker (p=0.37), alcoholic and non-alcoholic (p=0.61), diabetic and non-diabetic (p=0.062), hypertensive and non-hypertensive (p=0.25) patients and the differences were not statistically significant [Table/Fig-2].
Base line vitamin D level of the study population.
| Base line data | Population(N= 315) | Vitamin D level (ng/ml) (±SD) | p-value |
|---|
| Male (%) | 247(78.40) | 13.20 (9.6) | 0.73 |
| Female (%) | 68(21.60) | 14.20 (12.9) |
| Smoker (%) | 99(31.40) | 14.00 (10.6) | 0.37 |
| Non-smoker (%) | 216(68.60) | 13.20 (10.4) |
| Alcoholic (%) | 83(26.30) | 14.40 (12.3) | 0.61 |
| Non-alcoholic (%) | 232(73.60) | 13.10 (9.7) |
| Hypertensive (%) | 232(73.70) | 13.80 (10.3) | 0.25 |
| Non-hypertensive | 83(26.30) | 12.30 (10.8) |
| Diabetic (%) | 72(22.80) | 12.60 (11.8) | 0.062 |
| Non-diabetic | 243(77.10) | 13.70 (10.0) |
| Normal coronary (%) | 75 (23.80) | 11.30 (9.5) | 0.011 |
| CAD (%) | 240 (76.20) | 14.10 (10.7) |
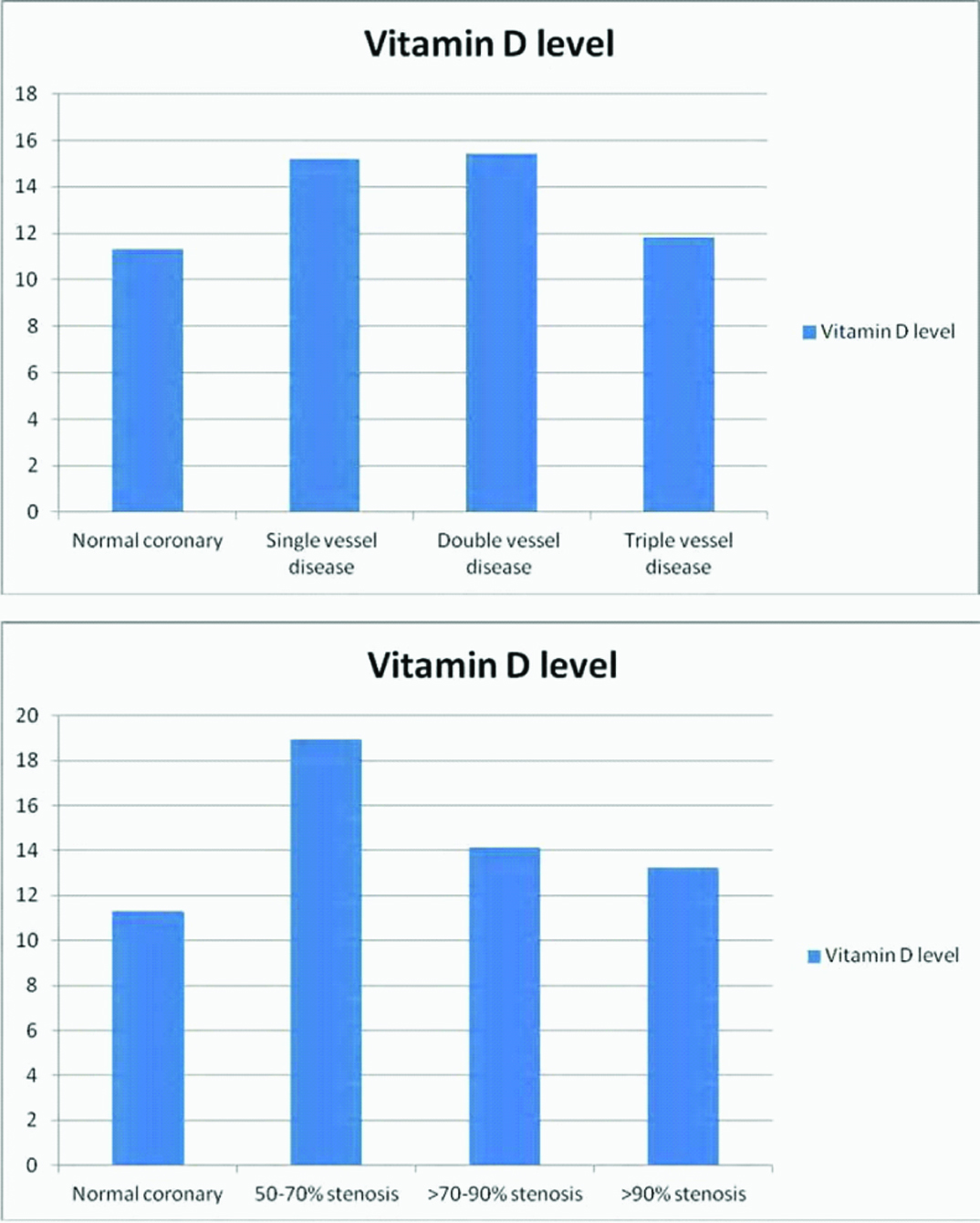
| 50-70% stenosis (%) | 21 (6.70) | 19.00 (16.5) | 0.46 |
| >70-90% stenosis (%) | 95 (30.20) | 14.10 (11.1) |
| > 90% stenosis (%) | 124 (39.40) | 13.20 (8.8) |
| Single vessel disease (%) | 70 (22.20) | 15.20 (13.0) | 0.14 |
| Double vessel disease (%) | 85 (27.00) | 15.50 (11.30) |
| Triple vessel disease (%) | 85 (27.00) | 11.80 (7.0) |
In our study, the patients with angiographically normal coronary artery and CAD both had low vitamin D level. However, the patients with normal coronary artery had much lower mean vitamin D as compared to the patients with CAD (p=0.011) [Table/Fig-2]. But, the mean vitamin D levels according to the severity of stenosis (p=0.46) and as well as the number of vessel involved (p=0.14) were not significantly different [Table/Fig-2]. As the severity of angiographic stenosis increased the mean vitamin D level was also decreasing [Table/Fig-2,3] and the patients with CAD with 50%-70% stenosis had much higher mean vitamin D level as compared to other study groups (p= 0.46). But this difference was statistically significant only when we compared it with mean vitamin D level of the patients with normal coronary artery (p= 0.018).
Vitamin D level and angiographic severity of CAD.
Vitamin D deficiency: The frequency of vitamin D deficiency was higher in patients with normal coronary artery (89.30%) as compared to the patients with CAD (81.70%), but statistically insignificant (p= 0.29) [Table/Fig-4]. The frequency of vitamin D deficiency was also very high in all the study groups of CAD according to severity of stenosis as well as the number of vessel involved, but lower than the patients with normal coronary artery [Table/Fig-4]. This difference was statistically significant only in between the patients with normal coronary artery and CAD with 50%-70% stenosis (p= 0.013). There was no statistically significant difference in frequency of vitamin D deficiency when we compared it between patients with normal coronary artery and CAD with >70%-90% stenosis (p= 0.49) or >90% stenosis (p=0.39) and in between the severity groups (p= 0.41). Frequency of vitamin D deficiency was also not significantly different according to the number of vessels involved (p= 0.075) [Table/Fig-4].
Vitamin D status according to the angiographic severity of CAD.
| Vitamin D status | Normal | Insufficiency | Deficiency | p |
|---|
| Normal Coronary (N=75) | 2(2.70%) | 6(8.00%) | 67(89.30%) | 0.29 |
| CAD (N=240) | 12(5.0%) | 32(13.3%) | 196(81.7%) |
| 50-70% stenosis (N=21) | 4(19.00%) | 3(14.30%) | 14(66.70%) | 0.41 |
| >70-90% stenosis (N=95) | 5(5.30%) | 11(11.60%) | 79(83.20%) |
| >90% stenosis (N=124) | 3(2.40%) | 18(14.50%) | 103(83.10%) |
| Single vessel disease (N=70) | 6(8.60%) | 7(10.00%) | 57(81.40%) | 0.075 |
| Double vessel disease (N=85) | 6(7.10%) | 11(12.90%) | 68(80.00%) |
| Triple vessel disease (N=85) | 0(0.00%) | 14(16.50%) | 71(83.50%) |
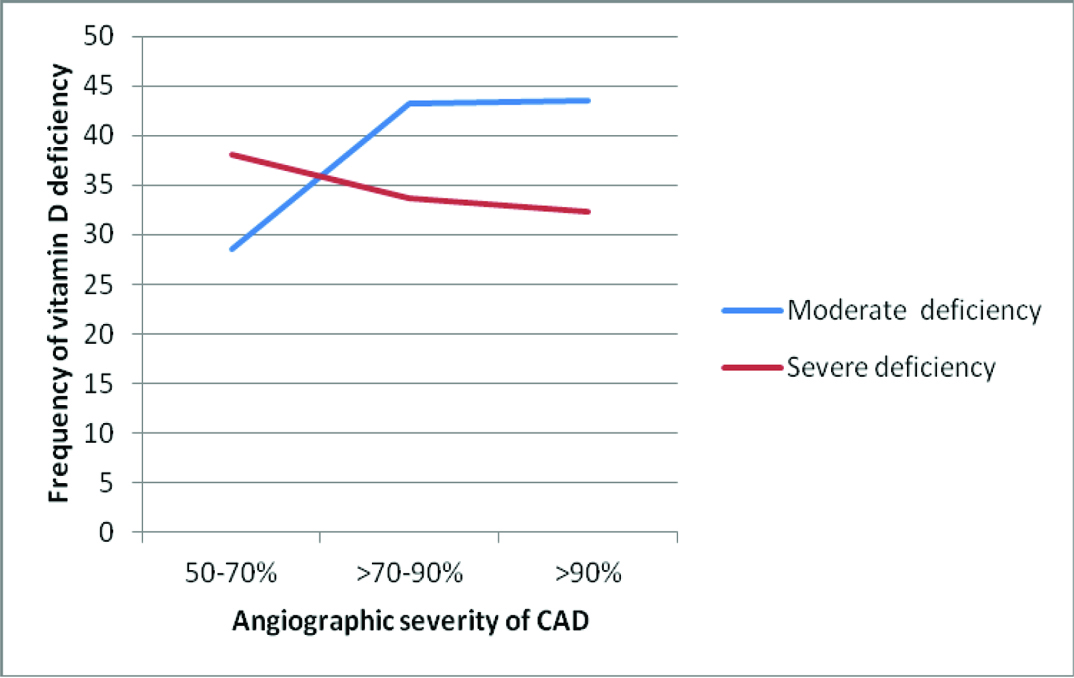
Severity of vitamin D deficiency: As the frequency of vitamin D deficiency was very high, 83.50% of the study population (263 out of 315), we sub-graded the severity of vitamin D deficiency [Table/Fig-5]. In our study the frequency of moderate vitamin D deficiency was increasing and the frequency of severe vitamin D deficiency was decreasing as the severity of stenosis increasing [Table/Fig-6], but statistically not significant (p=0.06). The patients with angiographic normal coronary artery had higher frequency of severe vitamin D deficiency as compared to the patients with CAD [Table/Fig-5] but statistically insignificant (p=0.15). The patients with CAD with single and double vessel disease had higher frequency of moderate vitamin D deficiency as compared to the patients with triple vessel disease and normal coronary artery [Table/Fig-5] but statistically insignificant (p=0.07). So the severity of vitamin D deficiency was also not significantly different in patients with normal coronary artery and CAD as well as in between the severity groups.
Severity of vitamin D deficiency according to the angiographic severity of CAD.
| Vitamin D level | >10-<20ng/ml (Moderate deficiency) | >3-10ng/ml (Severe deficiency) | ≤3ng/ml (Very severe deficiency) | p |
|---|
| Normal coronary (N=75) | 26(34.70%) | 32(42.70%) | 9(12.00%) | 0.15 |
| CAD (N=240) | 101(42.10%) | 80(33.30%) | 15(6.30%) |
| 50-70% stenosis (N=21) | 6(28.60%) | 8(38.10%) | 0(0.00%) | 0.06 |
| >70-90% stenosis (N=95) | 41(43.20%) | 32(33.70%) | 6(6.30%) |
| >90% stenosis (N=124) | 54(43.50%) | 40(32.30%) | 9(7.30%) |
| Single vessel disease (N=70) | 31(44.30%) | 24(34.30%) | 2(2.90%) | 0.07 |
| Double vessel disease (N=85) | 38(44.70%) | 26(30.60%) | 4(4.70%) |
| Triple vessel disease (N=85) | 32(37.60%) | 30(35.30%) | 9(10.60%) |
Severity of CAD VS. frequency of moderate and severe vitamin D deficiency.
Discussion
Multiple studies showed that, vitamin D deficiency is directly or indirectly associated with CAD [8,9]. Most of these studies were retrospective type and included patients with already diagnosed CAD. Our study was prospective, we measured vitamin D in patients who were undergoing coronary angiography and we included only angiography proven CAD and normal coronary artery. Our study also showed that prevalence of vitamin D deficiency is very high in patients with CAD. In addition it showed that, the prevalence of vitamin D deficiency is also very high in patients with normal coronary artery. So far none of the previous studies compared the serum vitamin D level and severity of vitamin D deficiency with the angiographic severity of CAD, according to the percentage of stenosis as well as the number of vessels involved. Data regarding association of vitamin D deficiency with CAD are also very less in South-east Asian and Indian population, where prevalence of vitamin D deficiency is very high. Two recent studies [22,23] in Indian population concluded that low vitamin D was associated with increased risk for CAD and endothelial dysfunction and the patients with lower vitamin D had higher prevalence of double or triple vessel and diffuse CAD. But the sample size was small, vitamin D was graded as deficiency (<20ng/ml) or non-deficiency (≥20ng/ml) only and the angiographic severity was not graded as percentage of stenosis. According to our study vitamin D deficiency and severity of vitamin D deficiency was not associated with angiographic severity of CAD according to percentage of stenosis and as well as the number of vessel involved. Recently published studies, conducted upon the population of Australia and Israel also found that vitamin D deficiency was significantly associated with CAD but the sample size was small [24,25]. The only Indian study [23] that showed association of vitamin D deficiency with CAD did not reveal the mean vitamin D of patients with normal coronary artery; neither compared it with other severity groups. The data regarding vitamin D status in normal healthy Indian population is still lacking. So far one study showed mean vitamin D level of 52.9ng/ml in summer and 31.8ng/ml in winter which was quite higher in comparison to our study population [26]. But this study included only young healthy age group of 18-25 years and minimum age of our study population was 30 years. At the same time few authors reported prevalence of vitamin D deficiency in Indian population as high as 70%-90% [27]. Further study may be needed to know the vitamin D status in normal healthy Indian population and our study data may be compared for further evaluation of the association of Vitamin D with CAD.
In our study almost whole population had vitamin D deficiency. According to our study, the patients with angiography proven normal coronary artery and CAD, both had high frequency of vitamin D deficiency, however the patients with normal coronary artery had much lower mean vitamin D (11.30ng/ml) as compared to the patients with CAD (14.10ng/ml). It may appear that lower vitamin D level may have protective role in developing CAD or patients with higher vitamin D level are more prone to have CAD, but it is not correct, as very high percentage (83.50%) of study population had vitamin D deficiency and very low percentage (4.40%) of study population had normal vitamin D level. These may be the cause that the patients with normal vitamin D showed higher frequency of CAD, as the patients who were suspected to have CAD underwent coronary angiography. The sample size of CAD with 50%-70% stenosis is also very low, only 6.70% of the study population. This may be the reason that, the patients with CAD with 50%-70% stenosis differ from the patients with angiographic normal coronary artery for vitamin D level, as well as vitamin D deficiency. Further study with larger sample size is needed for more appropriate comparison of different study groups.
According to our study, there was no significant difference of vitamin D deficiency and severity of vitamin D deficiency, between the patients with normal coronary artery and the different severity of CAD. But this cannot deny the association of vitamin D deficiency with CAD as the patients with angiographic normal coronary artery or insignificant CAD may not be the true representative of healthy population as they all had some symptom and sign for CAD and they all underwent coronary angiography as per indications and guide line [18]. They might be in the very early phase of the active disease and they required or utilized more vitamin D to prevent further progression of disease process, which resulted in lower vitamin D level, due to lack of supply or consumption. If we consider the patients with angiographic normal coronary artery as non-diseased or normal population then the association of vitamin D deficiency with CAD is really doubtful. In other words, it may be that the vitamin D deficiency may present with CAD symptoms, like angina on exertion or rest, chest pain, atypical chest pain. As observational studies yield only association and do not prove causality, the conflicting data on CAD and vitamin D can be elucidated better by randomized trials only.
Limitation
Control group of healthy population was not available. It is very difficult to prove association of vitamin D deficiency with CAD in a population, where prevalence of vitamin D deficiency is itself very high (70%-90%) [27].
Conclusion
Prevalence of vitamin D deficiency was very high in patients with CAD but vitamin D deficiency and the severity of deficiency does not correlate with angiographic severity of CAD. Vitamin D deficiency was also very high in patients with angiography proven normal coronary artery. If we consider the patients with angiography proven normal coronary artery as normal healthy population then the association of vitamin D deficiency with CAD is doubtful.
Funding: This research received no grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosures: The authors declare that there is no conflict of interest.