Percutaneous access to the upper urinary tract has become a well established procedure in the last two decades. Percutaneous approach offers a direct and shortest route for diagnosing pathology related to the upper urinary tract. In the era of rapidly evolving endo-urological procedures, Percutaneous Nephro Lithotomy (PCNL) has been a widely accepted and universally practiced endo-urological procedure for management of renal stones.
With increasing expertise gained in percutaneous accesses to the kidney, PCNL has now become an established standard of care in patients with renal stone disease, in terms of morbidity, stone clearance, overall duration of hospital stay and shorter convalescence period.
Urolithiasis affects 5-15% of the population worldwide and 50% of them show recurrence at some point of time [1]. Hence much emphasis is given for aiming at a complete stone free status. Various modifications have been tried and standardized in PCNL procedures. On one hand, the size of the tract has been miniaturized and on the other hand, the level of puncture has been advanced to supra-costal as well.
American Urological Clinical guidelines panel (2005) has recommended PCNL as the procedure of choice for patients with stag horn calculi with larger stone burden [2]. PCNL is also a viable option for stones more than 1 cm, especially in the lower calyx or in a calyceal diverticulum. Various factors play a role in deciding the ultimate success rate and complications in PCNL like stone size, site of initial puncture, number of punctures and duration of procedure [2]. This prospective study on all supracostal punctures performed in our Institution, over the last three and half years, gives an overview of the factors that predict safety and success rate of the procedure.
Hence the aim of the study was to prospectively study the feasibility of supracostal punctures and to analyze its safety, efficacy, complications and stone free rate in our institution.
Materials and Methods
This was a prospective study from July 2012 to Dec 2015 and 376 patients underwent PCNL for renal stone disease. Ninety two (n=92) patients needed supra-costal puncture for primary stone access and clearance. The decision for supra-costal access was made based on the stone location, pelvi-calyceal anatomy, direct access to either the stone or the most favorable calyx for maximal stone clearance in a shorter time period. The study was submitted to publication oversight committee for preliminary and Ethics committee clearance was obtained.
Patients with bleeding diathesis, giant stag horn calculi in which we felt better clearance would be obtained with open stone surgery were excluded from our study.
All 92 patients were subdivided into two groups. Based on the location and type of the stone, they were divided into Group 1 and Group 2. Group 1 included stones located in the renal pelvis with extensions into the calyces (Partial and Complete Stag horn stones) and Group 2 included stones primarily located in the renal pelvis or in the poles or in the juxta Pelvi Ureteric Junction (PUJ) upper ureter that was pushed back into the kidney for push back PCNL.
All patients had a pre-operative assessment in the form of complete blood count, coagulation profile, urine analysis and urine culture. Multi slice non-contrast Computed Tomography (CT) imaging was done in all patients and the longest diameter as seen in the CT imaging is taken as the stone size. Those with a positive urine culture underwent PCNL under adequate antibiotic coverage. For purpose of analysis of operative data and the list of complications in the peri-operative period, patients were grouped into those with stag horn and non-stag horn calculi.
Procedure
All patients received prophylactic antibiotics before the procedure. Those with a positive urine culture were adequately covered with appropriate parenteral antibiotics for at least 48 hours before taking them up for a definitive procedure and continued in the postoperative period until all catheters were removed.
The initial puncture was decided based on the retrograde pyelogram findings and intra renal anatomy of the pelvi-calyceal system. The entry into the calyx was also decided based on the location of the stone and the easiest, shortest and most direct access to the stone.
The punctures were done during full expiration through the lower part the of intercostal space in order to avoid injury to the lungs or pleura or the neuro vascular bundle. Serial dilatation was done using coaxial telescopic metal dilators upto the desired caliber, corresponding to the stone size. If multiple punctures were anticipated, guide wires were placed in the desired calyces before dilatation of the initial tract. A 20 unit is not specified French drainage tube was left as a nephrostomy at the end of the procedure. After placement of the nephrostomy tube, an antegrade nephrostogram was done on table in all patients to ascertain the integrity of PUJ. X-ray chest was done in the postoperative ward as a routine in all patients to ensure that there is no hydrothorax. On the second postoperative day, a plain X ray KUB was done in all patients before nephrostomy removal, in order to ensure a complete stone clearance. If there was any evidence of significant residual stone, a relook PCNL or Extra Corporeal Shock Wave Lithotripsy (ESWL) was planned.
Follow-up
All patients were followed up at 2 weeks, three months and 6 months. Repeat urine culture was done in all patients who had been treated for urinary tract infection preoperatively. Intravenous urogram was done in selected patients who had pelvi cayceal tear or residual fragments. A residual fragment size of < 4mm was considered as stone free status.
Statistical Analysis
Univariate and multivariate logistic regression analysis were used to identify factors that predict stone clearance and incidence of complications. Chi-square test and Fischer-Exact test were performed to compare the operative data and complication rate between the two groups. All p-values were two-tailed and a p-value of less than 0.05 was considered to be statistically significant. Data obtained were analyzed using SPSS statistical software package (SPSS version 11.0).
Results
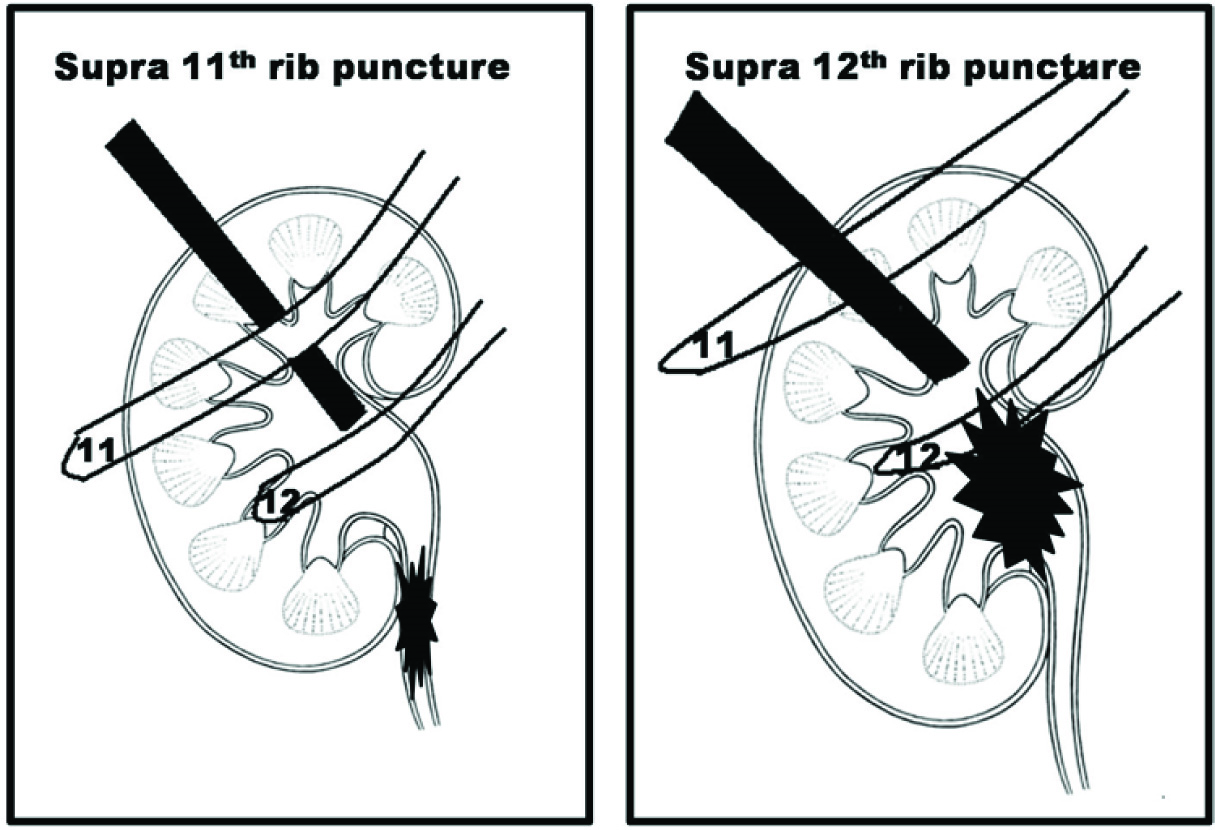
A total of 376 patients underwent PCNL over a period of three and half years from July 2012 to Dec 2015. Ninety-two of them (25%) needed supra-costal punctures and were included in our study. This group of patients included those who required Supra 12th and supra 11th rib punctures [Table/Fig-1]. These patients were further subdivided into two groups. Group 1 included 47 patients with stag horn calculi, of which 20 were complete stag horn stones and the remaining 27 were partial stag horn calculi. Group 2 had 45 patients, of which majority were in the renal pelvis. Descriptive data of the patients’ demographics are summarized in [Table/Fig-2].
Schaematic diagram depicting the puncture sites.
| Characteristics | Group 1 | Group 2 | Total |
|---|
| Number | 47 | 45 | 92 |
| Mean Age | 29.6 | 35.4 | |
| Sex distribution |
| Male | 29 | 25 | 54 |
| Female | 18 | 20 | 38 |
| Laterality |
| Right | 20 | 22 | 42 |
| Left | 27 | 23 | 50 |
| Anomalies of kidney |
| Previous open stone surgery | 9 | 1 | 10 |
| Horse shoe kidney | 1 | 1 | 2 |
| Bilateral duplex kidney | 2 | 0 | 2 |
| Bifid pelvis | 9 | 3 | 12 |
| Malrotated kidney | 8 | 4 | 12 |
| Stone size (Longest diameter) |
| 10-20 mm | 2 | 40 | 42 |
| 20-30 mm | 15 | 5 | 20 |
| 30-40 mm | 22 | 0 | 22 |
| More than 40 mm | 8 | 0 | 8 |
| Average stone size (mm) | 28.3 | 17.2 | |
| Stone opacity |
| Radio opaque | 43 | 31 | 74 |
| Radio lucent | 4 | 14 | 18 |
| Stone type |
| Partial stag horn | 27 | | |
| Complete stag horn | 20 | | |
| Upper ureter | | 14 | |
| Renal pelvis | | 20 | |
| Lower calyceal | | 11 | |
| Site of Initial puncture (n=92) |
| Upper calyceal | 18 | 14 | 32 |
| Mid calyceal | 4 | 12 | 16 |
| Lower calyceal | 25 | 19 | 44 |
Males were more commonly affected than females. Both sides were almost equally involved with a slight left preponderance. Bifid renal pelvis and mal rotated kidney constituted the most common associated renal anomalies. Previous stone surgery or anomalies of the kidney did not have any impact on the ultimate stone free rate. However, one patient with horse shoe kidney had pelvi-calyceal tear and two other patients with malrotated kidney had prolonged time to gain access to pelvi-calyceal system, puncture related bleeding and haematuria with clot retention. Ten patients had a previous open stone surgery of which 9 of them were from group 1. Majority of the stones were in the range of 1-2 centimeters. This high number of relatively small stones is probably because most of the juxta PUJ and upper ureteric and lower pole renal calculi were all subjected for PCNL. Most of the stones in both the groups were radio opaque (80%).
The details of the number and level of punctures, duration of the procedure, complications encountered during and after the procedure and the need for any form of ancillary procedures are illustrated in [Table/Fig-3].
Perioperative parameters.
| Characteristics | Group 1 | Group 2 | Total | p-value |
|---|
| Level of puncture (n=92, 132 punctures in total) |
| Supra 12th | 76 | 28 | 104 | 0.0014 |
| Supra 11th | 11 | 17 | 28 |
| Number of punctures (n=92, 132 punctures in total) |
| Single puncture | 17 | 45 | 62 | |
| Two punctures | 20 | 0 | 40 | |
| Three punctures | 10 | 0 | 30 | |
| Duration of procedure (n=92) |
| Less than 60 min | 5 | 35 | 40 | |
| 60-90 min | 24 | 6 | 30 | |
| 90-120 min | 13 | 4 | 17 | |
| More than 120 min | 5 | 0 | 5 | |
| Stone Free Rate |
| Complete clearance | 33 | 43 | | |
| Incomplete clearance | 14 | 2 | | |
| Clinically Insignificant residual fragments (<4 mm) | 8 | 2 | | |
| More than 4 mm, (needing ancillary procedures) | 6 | 0 | | |
| Need for Ancillary procedures (n=6) |
| ESWL | 4 | 0 | | |
| Relook PCNL | 1 | 0 | | |
| Ureteroscopy | 1 | 0 | | |
| Complications as per Clavein Dindo classification |
| Grade I: |
| Transient fever >100O F | 7 | 1 | 8 | 0.0008 |
| Transient Haematuria | 10 | 2 | 12 |
| Grade II: |
| Peri Nephrostomy Catheter Urine leak | 1 | 0 | 1 | 0.0004 |
| Blood Transfusion | 8 | 0 | 8 |
| Post op Ileus | 5 | 1 | 6 |
| Grade IIIa: |
| Bacteraemia/sepsis | 4 | 0 | 4 | 0.0009 |
| Pelvi-calyceal tear/perforation | 6 | 2 | 8 |
| Hydrothorax requiring Intercostal drain insertion | 2 | 0 | 2 |
| Urinary retention due to blood clots | 3 | 0 | 3 |
| Grade IIIb: |
| Need for PCD | 1 | 0 | 1 | 1.000 |
| Grade IV a, IV b, V | NIL | NIL | NIL | NIL |
| Total | 47 | 6 | 53 | |
In all, 132 tracts were established in 92 renal units. 20 (22%) needed two punctures and 10 needed three punctures. The duration of the procedure was calculated from the time of placement of the ureteric catheter upto the placement of nephrostomy after complete stone retrieval. Stone free status was ascertained postoperatively under image intensifier guidance. In about 76% (n=70), the procedure required only less than 90 min. The maximum time taken was for a complete stag horn stone, which needed 165 minutes to clear the stone, leaving behind a one centimeter upper calyceal fragment that was cleared by ESWL.
[Table/Fig-3] also illustrates the list of complications of supracostal PCNL, as per Clavein Dindo classification. Grade I, II and IIIa complications were found to be significantly seen in Group 1 patients. Transient haematuria was the most common postoperative finding observed in 10 patients. Nephrostomy tract bleed was observed in three patients. Immediate relook nephrostomy could not identify any specific bleeding point in any of the three patients. However, all these three patients developed clot retention in the postoperative period, needing a bladder wash and a change of catheter.
Two patients developed hydrothorax. Both were complete stag horn stones, needing three punctures to clear the fragments. One of them needed intercostals drainage tube placement in the postoperative recovery room and the other settled with needle aspiration.
About 83% (n=76) of patients achieved a complete stone free rate after initial PCNL. Sixteen of them had incomplete clearance, of which 10 of them had only tiny fragments and were deemed insignificant. Four patients needed ESWL and one each required Relook PCNL and Ureteroscopy.
[Table/Fig-4] summarizes the univariate analysis of factors that predispose to complications after PCNL. Fifteen patients (16%) had complications related to the procedure, of which 13 were in group 1 (87%). The high percentage of complications in patients with larger stone burden has been found to be statistically significant (p=<0.0037). Also, in those 22 patients in whom the duration of procedure exceeded 90 minutes, 12 of them had complications, with a p-value of <0.0001. Stones needing multiple punctures also had a higher incidence of complications. Patients with higher stone burden needed more ancillary procedures. About 25% of those (n=7) with Supra 11th puncture developed complications, which was statistically significant (p=0.0178). Both the hydrothorax in our study were seen in supra 10th punctures.
Univariate analysis of factors that predispose to complications after PCNL.
| Complications, if any | Total | p-value |
|---|
| Stone type (n=92) | Yes | No |
|---|
| Group 1 | 13 | 34 | 47 | 0.0037 |
| Group 2 | 2 | 43 | 45 |
| Duration of procedure (n=92) |
| <90 min | 3 | 67 | 70 | 0.0001 |
| >90 min | 12 | 10 | 22 |
| No. of punctures (n=132) | | | | |
| Single puncture | 4 | 58 | 62 | 0.1076 |
| Multiple punctures | 11 | 59 | 70 |
| Need for Ancillary procedures (n=92) |
| Group 1 | 6 | 41 | 47 | 0.0265 |
| Group 2 | 0 | 45 | 45 |
[Table/Fig-5] describes the factors that affect the stone clearance rate after PCNL. Larger stones, more than 3 cm, were found to be associated with significant residual stones. There was no significant difference between the two genders or between the two sides. Radio opacity as seen under image intensifier also had a significant impact on the ultimate stone free status. Nearly 30% of the radiolucent stones had inadequate clearance and this difference was found to be statistically significant. About 23% of those (n=5/22) who needed longer duration of surgery had a clinically significant residual stones, needing ancillary procedures. This number was found to be statistically significant (p= 0.0027). Moreover, 4 out of 6 patients (67%) with residual stones also had some complication or the other in the peri-operative period. The number of punctures or the level of puncture did not have a statistically significant impact on the ultimate stone free status.
Univariate analysis of factors that affect stone free rate after PCNL.
| Characteristics | Stone free status | Clinically significant Residual stones | p-value |
|---|
| Number of patients | 86 | 6 | |
| Stone Size |
| <3 cm | 62 | 0 | 0.0008 |
| >3 cm | 24 | 6 |
| Stone opacity |
| Radiopaque | 72 | 2 | 0.0125 |
| Radiolucent | 14 | 4 |
| Number of access |
| Single | 60 | 2 | 0.0859 |
| Multiple | 26 | 4 |
| Duration of surgery |
| Less than 90 min | 69 | 1 | 0.0027 |
| More than 90 min | 17 | 5 |
| Complications |
| Yes | 11 | 4 | 0.0044 |
| No | 75 | 2 |
Discussion
From the time PCNL has been introduced in the management of renal calculi, there has been a constant and a continuous progression and refinement in the technique of PCNL. Clayman and colleagues first published in 1983 their experience on PCNL in treating staghorn stones [3]. Currently PCNL is a safe and an effective treatment modality for treating branched and staghorn calculi [4].
The primary goal of treatment of renal calculi is complete stone clearance with minimal morbidity to the patient [5]. In order to achieve an adequate stone clearance, various improvisations in the standard PCNL procedure have been carried out. Desai et al., introduced the concept of Multiperc – Multi tract approach, where multiple tracts are being made, aiming at complete stone clearance. In his series, in over 834 renal units, Desai et al., concluded that achieving a complete stone clearance continued to be a challenging task, despite multiple punctures and multiple tracts [6].
In majority of patients, access to the desired calyx is possible by an infra costal puncture. But in managing patients with staghorn stones, it may be required to adopt a supracostal approach aiming at direct access to stone and at complete clearance [7,8]. The aim of our study has been to prospectively study the feasibility of supracostal punctures and to analyse the efficacy, complications and stone free rate following supra-costal punctures.
Hossain et al., considered the upper calyceal approach to be ideal for management of upper ureteric, upper calyceal and stag horn stones [9]. Though technically more demanding and challenging, they claimed that entry through upper calyx provided a straight access along with a better visualization of upper and lower calyces, renal pelvis and PUJ. In their study on 28 patients who needed supracostal punctures, 68% of them needed upper calyceal entry tract. In our study, majority of them (48%) needed a lower calyceal entry and only 35% needed upper calyceal punctures. Rohit Singh et al., concurred with this view point and further emphasized that with due precautions, one should not hesitate to go even for an upper calyceal puncture, if indicated [10].
Cephalad movement of the kidneys has been observed in upto 80% of the patients especially when turned to prone position [11]. This makes it imperative on many occasions to opt for supra-costal punctures, especially when aimed at a direct access to the stone. In such instances, there is a higher chance of injury to pleura and lung parenchyma [12]. Injury to intercostals vessels and pleura may cause severe bleeding and hydrothorax respectively, necessitating an intercostals drain placement. The overall incidence of hydrothorax, as reported by various authors is around 0 to 12% [13–16]. Rajiv Yadav, in his study of 762 cases, noted the incidence of hydrothorax to be around 3.3% [17]. However, in our study, the overall incidence was only 2.17%.
Stone free status after PCNL has been reported to be so variable. Various factors including overall stone burden, degree of hydronephrosis, ability of the stone to be appreciated under image intensifier and the choice of initial puncture have all been shown to alter the final outcome [18,19]. Ancillary procedures like ESWL, Relook PCNL and Flexible Ureteroscopy have all been shown to decide the ultimate stone free status.
Tarek et al., in his study on 40 renal units observed a 78% stone free status after PCNL monotherapy [20]. In our study, 93% of patients achieved complete stone free status, with only 6 patients needing ancillary therapy. This apparently high stone free status may partly be also due to inclusion of stones ranging from 1 to 2 cm, especially in the lower calyx, in the upper ureter or in the renal pelvis, which were all mostly removed without the need for much fragmentation. The other reasons could be a higher number of radio opaque stones, usage of multiple punctures wherever required in order to achieve a complete stone clearance and readily going for supra 11th rib puncture, if it offers a most direct and easy access to complete stone clearance.
The total duration of the procedure is also shown to have a significant impact on the overall outcome. In our series, 12 out of 22 patients who had a prolonged surgery for more than 90 minutes developed complications, which was statistically significant. Those who had malrotated kidney (n=2 out of 12, 17%) took a longer time to puncture and developed intra operative bleeding, haematuria and clot retention.
Stone burden was also identified to be a significant factor that predisposes to complications. Size of the stone and the duration of the procedure were directly correlating with the overall incidence of complications after PCNL. Patients who needed supra 11 puncture had a relatively higher incidence of complications (25%) compared to supra 12 punctures. Both patients who had hydrothorax were of supra 11 punctures and needed either Intercostal tube drainage or needle aspiration. Moreover, supra 11 punctures were also associated with intraoperative bleeding and clot retention which were considered to be statistically significant.
With regards to stone free rate, stone burden and its radio opacity were identified to be the main factors that decided the ultimate stone free rate. The level of puncture (either supra 11 or supra 12 punctures) did not have any significant impact on the ultimate stone free rate.
Limitation
Comparison between supra and infra costal punctures is a good option, but beyond the scope of this paper. Moreover, this paper only highlights the safety and efficacy of supracostal punctures and hence the authors feel that there is no need for such a comparison.
Conclusion
Supracostal punctures via the 10th and 11th intercostals spaces is a very safe, effective and a viable option in selected group of patients. The overall results are almost on par with that of the infra costal punctures, with an acceptable morbidity. The complication rate, stone free status and the need for ancillary procedures are directly related to the stone burden, its radio opacity and the duration of the procedure. Overall complication rate was significant in patients with supra 11th rib punctures. By careful adherence to the basic principles of PCNL during the puncture and by maintaining a close surveillance during the perioperative period, one will to a greater extent be able to minimize the overall incidence of complications that arise from supracostal punctures.