The coronoid and the olecranon fossae are located at the distal third of the humerus, and they are usually separated by a thin wall. In some cases, this membrane is perforated, producing the Supratrochlear Foramen (STF), an anatomic variation of great clinical and anthropological interest [1–5].
The STF has a varying incidence among different races, ranging close to 0% up to 60%, as many studies have shown [2,6–9]. Individuals who possess this variation may present overextension of the elbow joint [6,10]. The causes of this variation are not clear, although, its incidence was studied among different ethnic groups, which demonstrated differences between them, with a predisposition on the left side [1,11].
This aperture is one of many areas of the skeleton that can be characterized by relative radiolucency, as such, it can be misinterpreted as an osteolytic or cystic lesion, furthermore, studies have shown that the presence of the STF can be related to a narrower medullary canal, which is of vital importance to intramedullary fixation [2,11,12].
The current study presents the measures of the STF in Brazilian humeri and quantifies the necessary amount of radiation in order to see the presence of this anatomic variation in radiographic images. This was the first study to address the incidence of the STF in Brazilian bones. This research is in accordance with ethical considerations of the Declaration of Helsinki.
Materials and Methods
This study was conducted at the Fluminense Federal University, Gama Filho University and Grande Rio University during 2 years and 3 months (2013-2015). A total of 330 dry humeri (185 pertaining to the left side and 145 pertaining to the right side) were analysed. All bones were from Brazilian cadavers free from any pathology and belonged to three different medical schools from Rio de Janeiro, Brazil. Only adult bones were used in this study.
The humeri were divided in three groups: with STF (Group 1), with a translucent STF (Group 2) and without STF (Group 3). The horizontal and vertical diameters of the foramen were measured using a digital vernier caliper. Random humeri from the three groups were selected and radiological images were taken. All radiological incidences had a thin focus of 100. The kilovoltage (kV) and milliamperage per second (mAs) were adjusted in order to produce images that allowed comparative parameters.
We performed a paired two-tailed student’s t-test (p < 0.05 was considered significant) and obtained descriptive statistics (mean and standard deviation) of both sides were obtained through the Graph Pad 6 Prism software.
Results
In the 330 humeri studied, 74 (22.5%) possessed the STF (Group 1), 46 humeri of this group were left sided (62.1%), and 28 were right sided (37.8%), 136 bones (41.2%) showed a translucent STF (Group 2), 63 (46.3%) belonged to the left side, and 73 (53.6%) belonged to the right side. In 120 bones (36.3%), the STF was absent (Group 3), as shown in [Table/Fig-1].
Incidence of the Supratrochlear Foramen (STF).
| Humeri (n = 330) | % | Left | Right |
|---|
| Group 1 (With STF) | 22.5% (74) | 62.1% (46) | 37.8% (28) |
| Group 2 (Translucid) | 41.2% (136) | 46.3% (63) | 53.6% (73) |
| Group 3 (No STF) | 36.3% (120) | - | - |
The mean vertical diameter (MVD) of the STF in Group 1 (left side) was 2.780 mm, with a Standard Deviation (SD) of 2.050 mm, and the mean horizontal diameter (MHD) 2.332 mm with a SD of 1.234 mm; the MVD of the STF in right sided humeri was 2.778 mm, with a SD of 2.197 mm, and the MHD was 2.365 mm with a SD of 1.396 mm [Table/Fig-2].
Measures of the Supratrochlear Foramen (STF) of the Group 1.
| STF Measures (mm) | VD | SD | HD | SD |
|---|
| Left Side | 2.780 | 2.050 | 2.332 | 1.234 |
| Right Side | 2.778 | 2.197 | 2.365 | 1.396 |
The paired two-tailed student’s t-test showed that there was no significant difference between the VD and HD of the STF in humeri from the left and right sides (p = 0.22 for the HD, and p = 0.19 for the VD).
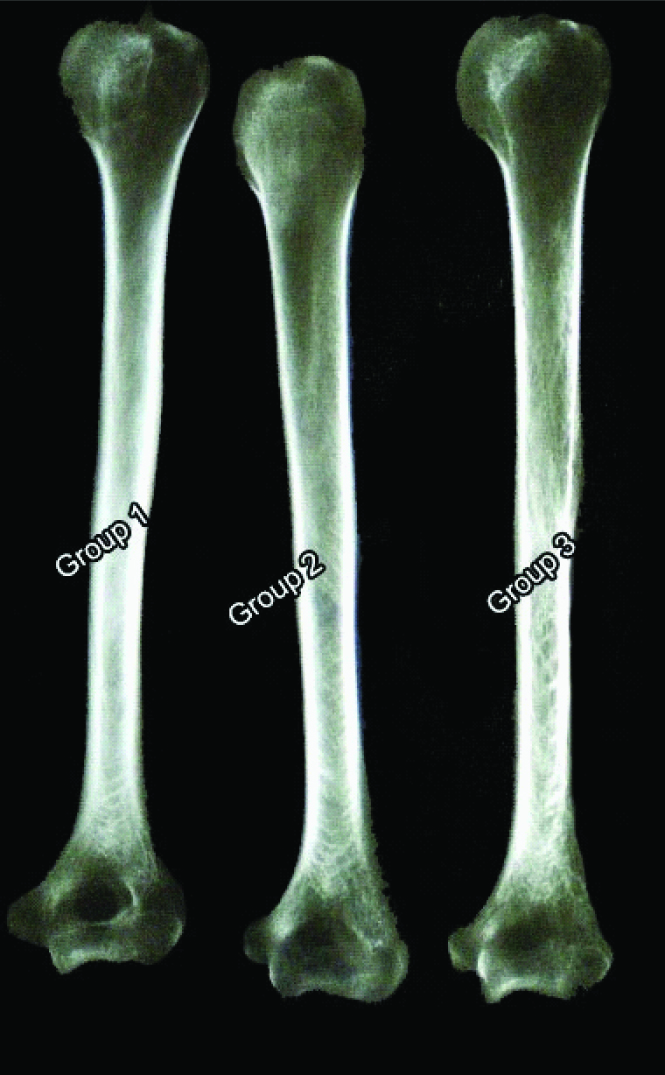
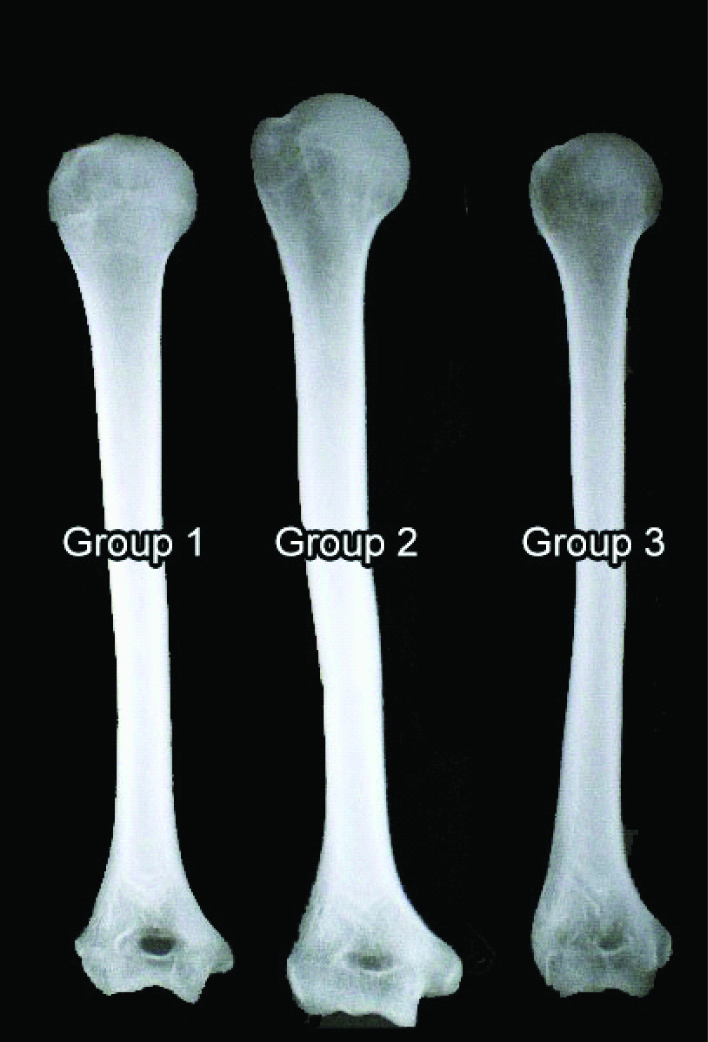
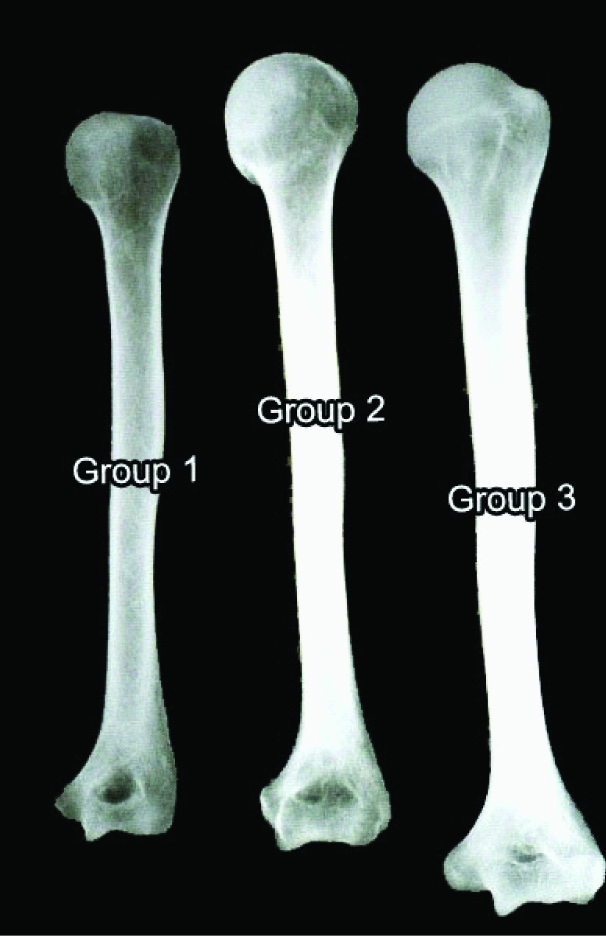
Our radiological analysis showed that using a setup of 45 kV and 0.05 mAs to take the radiographic image did not allowed a precise differentiation between the presence, translucence or absence of the STF [Table/Fig-3]. Afterwards, we increased the mAs in 0.03 (making it 0.08 mAs in total), which demonstrated a better view of the STF and we were able to some degree differentiate the three distinct groups [Table/Fig-4]. In our third attempt, we observed the three groups using a setup of 50 kV and 0.08 mAs, associated with a slight increase in the distance of the x-ray tube. The third method produced an image in which the STF could be easily observed, also, the humeri from the three groups could be precisely distinguished [Table/Fig-5].
STF radiolucency (Radiographic incidence of 45 kV and 0,05mAs).
*There is no difference between the three groups
STF radiolucency (Radiographic Incidence of 45 kV and 0,08mAs).
**Slight difference is seen between groups
STF radiolucency (Incidence of 50 kV and 0,08 mAs, associated with a slight increase in the x-ray tube distance).
*The STF can be easily distinguinshed between groups
Discussion
The supratrochlear foramen (STF), also known as septal aperture, intercondylar foramen or olecranon foramen occurs when the bony wall that separates the olecranon and coronoid fossae of the humerus is absent or perforated [1,2,7,11,12]. The thin, transparent plate of bone that separates both fossae is usually named as the supratrochlear septum and its thickness vary from 0.5mm to 1cm. Invivo this septum is covered by a synovial membrane of the elbow joint. In addition, it was shown that the aperture can be classified in different shapes, such as: oval (the most common), round, triangular and irregular, although some authors found unusual shapes, such as reniform [1–4,8,9,13,14].
The presence of the STF seems to be neglected in anatomy and orthopedics textbooks, despite its increasing clinical significance and its anthropologic aspect. It was first described by Meckel between 1816 and 1825 [1–3,9,11,15]. The STF seems to be more frequent at the left side (as our study showed) and in females, although some studies showed a higher incidence in males [1–3,14,16,17]. In bilateral cases, the septal aperture was reported to have a larger size on the left side [15], in contrast, our data demonstrated that there is no significant difference in the vertical and horizontal diameters of the foramen between the left and right sides.
Our study showed that the STF appears in 22.5% of cases, this is in accordance with studies performed in Indian bones, which showed similar results, such as 21.4% [11], 23.0% [18], 24.1% [19], 24.5% [9] and it seems that there is a significant gap between our results and results from studies performed in Europeans or American Whites: 4.2% [20] and 6.1% [21]. Moreover, studies performed in Asians also showed a large discrepancy in comparison to our results: 9.5% [22] and 10.3% [14]. Investigation on African groups showed that they indeed have a higher incidence of the STF, such as 37%, 39%, 41% [17] and 47% [21]. Even though there is a greater incidence of the STF in Africans, it is worth mentioning that there is discrepancy among ethnic groups of the same race, such as in Indians, there are results that range 19.2% [7] to 58% [20]. Detailed results from other studies are shown in [Table/Fig-6].
Incidence of the Supratrochlear Foramen in Different Populations.
| Population/Country | Author(Year) | Sample (n) | Incidence (%)/(n) | Left Side | Right Side |
|---|
| Greeks | Papaloucas et al., (2011) [15] | 1312 | 0.304% (4) | 2 | 2 |
| American Whites | Hirsh (1927) [20] | - | 4.2% | - | - |
| Netherlands | Glanville (1967) [21] | 299 | 6.1% (18) | 10 | 8 |
| Turkish | Öztürk et al., (2000) [16] | 114 | 7.9% (9) | 5 | 4 |
| Turkish | Koyun et al., (2011) [23] | 709 | 8.6% (61) | 35 | 26 |
| Chinese | Ming-Tzu (1935) [22] | 264 | 9.5% (25) | 14 | 11 |
| Chinese | Li et al., (2015) [14] | 262 | 10.3% (27) | 18 | 9 |
| Turkish | Erdogmus et al. (2014) [8] | 166 | 10.8% (18) | 14 | 4 |
| Europeans | Ndou et al. (2013) [17] | 100 | 16% (16) | - | - |
| Indians | Raghavendra et al. (2014) [7] | 260 | 19.2% (50) | 32 | 18 |
| Indians | Arunkumar et al., (2015) [11] | 355 | 21.4% (76) | 39 | 37 |
| Indians | Krishnamurthy et al., (2011) [18] | 180 | 23.0% (42) | - | - |
| Northern Indians | Diwan et al., (2013) [19] | 1776 | 24.1% (428) | 245 | 183 |
| Southern Indians | Mathew et al., (2016) [9] | 244 | 24.5% (60) | 41 | 19 |
| Eastern Indians | Chatterjee (1968) [1] | - | 27.4% | 35 | 22 |
| Northern Indians | Singh and Singh (1972) [1] | - | 27.5% | 31 | 24 |
| Nigerians | Sunday et al., (2014) [2] | 65 | 27.7% (18) | 14 | 4 |
| Southern Indians | Singhal and Rao (2007) [1] | 150 | 28.0% (42) | 20 | 22 |
| Indians | Bhanu and Sankar (2012) [3] | 121 | 30.5% (37) | 24 | 13 |
| Indians | Ananthi et al., (2011) [10] | 214 | 31.3% (67) | 48 | 19 |
| Central Indians | Kate and Dubey (1970) [1] | - | 32.0% | 35 | 28 |
| Xhosa (Africans) | Ndou et al., (2013) [17] | 100 | 33% (33) | - | - |
| Indians | Nayak et al., (2009) [6] | 384 | 34.4% (132) | 59 | 73 |
| Indians | Jadhav and Zambare (2015) [4] | 222 | 34.6% (77) | 38 | 39 |
| Zulu (Africans) | Ndou et al., (2013) [17] | 100 | 37% (37) | - | - |
| Tswana (Africans) | Ndou et al., (2013) [17] | 64 | 39% (25) | - | - |
| Sotho (Africans) | Ndou et al., (2013) [17] | 100 | 41% (41) | - | - |
| Tellem (Africans) | Glanville (1967) [21] | 170 | 47.0% (79) | 47 | 32 |
| Arkansas Indians | Hirsh (1927) [20] | - | 58.0% | - | - |
| Present study | Chagas et al., 2016 | 330 | 22.5% (74) | 46 | 28 |
*Note: Bilateral cases were counted as 1 on each side. Some data were not reported by the authors.
Many different species, such as dogs, hyenas, cattle, pigs and primates present this anatomic variation. In order to feed, those mammals adopt a different posture with the purpose of tearing the flesh of its prey, this fact could explain the existence of the STF in these animals, as they would increase the pressure of the area. In dogs, the STF connects the olecranon fossa and the radial fossa, which could explain high rates of bicondylar fracture [2,3,10]. Darwin theorized that the STF in humans seems to link man’s origin to lower primates, as this aperture is more commonly found in primates and it appears that the incidence of the septal aperture is decreasing in comparison to the Paleolithic and Neolithic eras, thus, making this variation an important feature to study anthropology and evolution, also, the STF can be described as a phylogenetic and atavistic feature, since it is suppressed by the stronger limb and exhibited in the weaker limb (the left side) [1–4,6,7,19], in accordance to our findings.
There were significant difference between the size of the foramina, ours being smaller than in other studies [6,18,19], and we believe that this is due to miscegenation process that happened in Brazil during its colonization and still happens in its current era.
The cause of the STF still seems to be unknown, hypothesis such as: failure of the ossification process; mechanical pressure caused by an enlarged olecranon process during hyperextension of the elbow; atrophy of the bone after ossification; disturbance in the calcium metabolism; decrease in blood supply caused by pressure; furthermore, atavistic and phylogenetic characteristics were described in the literature in order to explain the septal aperture origin [1–8,19,23–25]. The thin bony membrane between the olecranon and coronoid fossa is always present until the age of seven years, after which the bony septum occasionally becomes absorbed to form the STF, additionally, studies have shown that the humerus is not perforated during the embryonic development phase, usually developing in adolescence or adulthood [2–4,8,14,25].
Clinically, the presence of the STF is of great interest, as it was shown that the width of the medullary canal is smaller in humeri presenting this aperture than in humeri without it. This canal seems to be wider in the proximal third and circular in shape, while it is narrower in the distal third. Thus, the medullary canal should be analysed in cases of traumatic injuries or pathologic lesions, since procedures such as intramedullary fixation are becoming a popular choice of treatment [1–3,6–9,26].
The intramedullary fixation is the standard treatment of supracondylar fractures (the most common elbow fracture in pediatric patients) and pathological disorders. Nevertheless, there is controversy among surgeons regarding the route of the pin entry while treating this condition. This needs proper consideration, since iatrogenic lesions are the most severe form of complication during this procedure. Thus, the surgeon must have knowledge about the septal aperture in order to avoid damage of the area and nail incarceration. Moreover, some authors reported that the STF is located near to the medial epicondyle, which results in a more difficult approach to the intramedullary nailing and the best point for the nail insertion seems to be an area located anteromedially between the greater tubercle and the caput humeri [1–3,6,8,26,27]. The STF can be associated with other anatomical variations of the humerus, such as the supracondylar process and the Struther’s ligament, which, could cause neurovascular compression of the median or ulnar nerve and the brachial artery [13]. Furthermore, Roaf, in 1957, reported a case where the median nerve ran through the STF on the left side, causing pain and weakness of the hand [28], also, cases of osteochondritis dissecans - a necrotic process of the bone - involving the supratrochlear septum have been described [29].
In radiographic images, the STF can be misdiagnosed as an osteolytic or cystic lesion, causing confusion among physicians [1,4,11,12,17,20]. Our study demonstrated that the aperture can be easily visualized in a specific radiological setting, thus diminishing chances of misdiagnosis. Koyun et al., performed a study of the STF with the use of X-ray and Computerized Tomography (CT) in living subjects, although the parameters of the X-ray were not reported, they found that in some images, the STF couldn’t be seen because of its size or because there was presence of trabecular bone in the septum - our studies proposes to clarify those issues by setting standard values when performing the radiography [23]. Karthikeyan et al., published a paper in which they analysed the radiographic aspects of the STF, they stated that there is indeed an area of radiolucency in the distal extremity of the humerus, in accordance to our results. Also, their results showed that the intramedullary canal in fact gets narrower as it gets closer to the STF, and humerus with septal aperture have a narrow canal in comparison to humeruswithout the STF [30], in accordance with Paraskevas et al., and Akpinar et al., as it was previously stated [26,27].
Limitation
Our study was limited on the sense that we only collected humeri from one state (Rio de Janeiro) of many, as Brazil is a large country which has 26 states and measurements from either the x-ray machine or a CT scan directly would have been more accurate. Furthermore, studies on younger bones would have been more useful to describe the embryological aspects of such foramen.
Conclusion
We found that the incidence of the STF in a Brazilian sample of 330 humeri was 22.5%, being more common at the left side (62.1%). The data analysed showed that the STF is of great importance, as it has clinical, anatomical, radiological and anthropological relevance. The STF can be mistakenly diagnosed as an osteolytic lesion in radiographi, we report that the best x-ray setup to prevent this misdiagnosis was 50 kV and 0.08 mAs, associated with a slight increase in the distance of the x-ray tube, as it shows a clear view of the aperture. Besides, the STF possess an unknown mechanism of formation and a varying incidence among races, which requires further investigation in order to clarify those aspects.
*Note: Bilateral cases were counted as 1 on each side. Some data were not reported by the authors.