Small Cell Carcinoma of Anal Canal - A Rare Case Report
Surag1, Chandrashekar Neeralagi2, Arun Prasath3, Puneeth Kumar4, Bharath Reddy5
1 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
2 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
3 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
4 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
5 Junior Resident, Department of Pathology, ESIC Medical College, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Surag, Kamal Dev Daycare Clinic, S.P Road, Sakleshpur, Hassan- 573134, Karnataka, India.
E-mail: surag244@gmail.com
Anal canal malignancy is one of the dreadful conditions. Most of the anal canal malignancies are squamous cell carcinomas for which the treatment is well established and the prognosis is usually favourable. Small cell carcinoma of anal canal is a very rare condition and poorly understood, which can present as haemorrhoids in its early stages and has an aggressive course. We present a case of small cell carcinoma of anal canal who underwent Abdomino Perineal Resection (APR) and chemotherapy. He developed liver metastasis during the course of chemotherapy and succumbed to the condition 4 months later.
Abdomino perineal resection, Lump, Painful, Per-rectal
Case Report
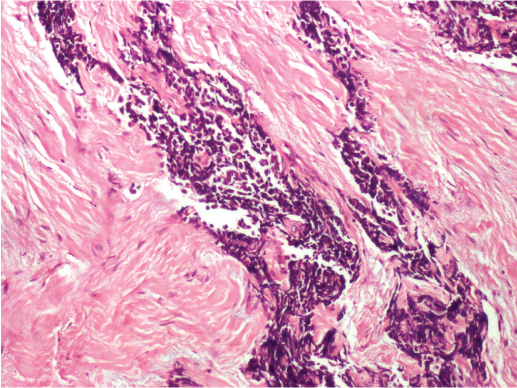
A 46-year-old male patient presented with complaint of painful bleeding and lumps in anal region since 3 months. He had undergone haemorrhoidectomy one year back. He didn’t have any other co-morbid conditions. There was no history of smoking. Per rectal examination couldn’t be done without anaesthesia since he had sphincter spasm. On evaluation under anaesthesia, the patient had a freely mobile, friable growth about 2 cm from the anal verge along posterior and the lateral wall. A biopsy was taken and the histopathological examination revealed small malignant cells with hyperchromatic nuclei and scanty cytoplasm with tumour invading the fibro-collagenous tissue with features of poorly differentiated malignancy [Table/Fig-1,2].
Tumour invading the fibrocollagenous tissue with features of poorly differentiated malignancy (H&E; 10X).
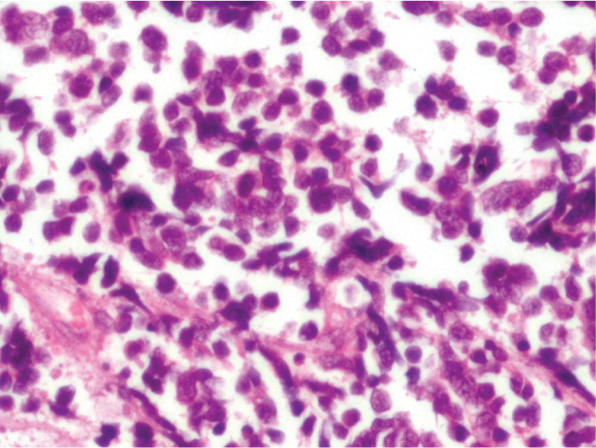
Small malignant cells with hyperchromatic nuclei and scanty cytoplasm (H&E; 40X).
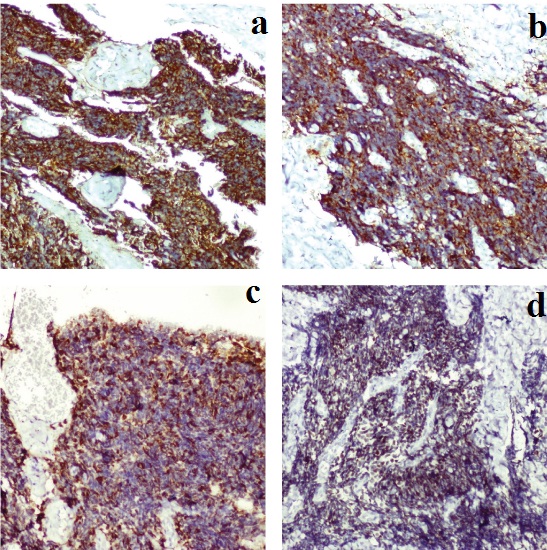
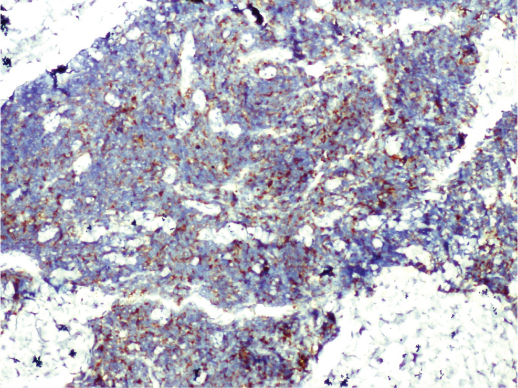
On Immunohistochemistry, neoplastic cells were strongly positive for CK 7, synaptophysin, chromogranin, TTF1 [Table/Fig-3a-d] and negative for S-100, LCA, CK20 and CDX2 [Table/Fig-4,5]. All the above features were suggestive of small cell neuroendocrine carcinoma.
Immunohistochemistry: (a) positive for CK 7 (10X); (b) positive for synaptophysin (10X); (c) positive for chromogranin (10X); (d) positive for TTF1 (10X).
Immunohistochemistry showing negativity for S-100 (10X).
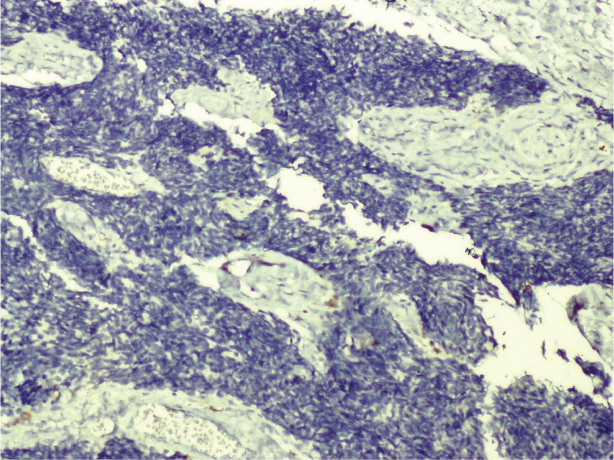
Immunohistochemistry showing negativity for LCA (10X).
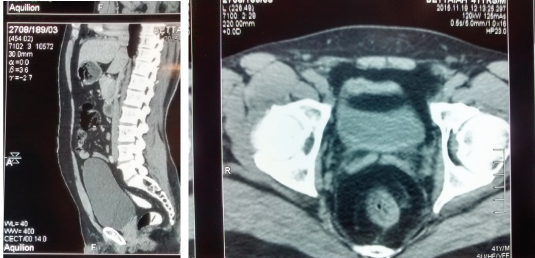
Colonoscopy was done which showed lesion in the posterior and lateral wall measuring about 4cm and 2cm from anal verge. Rest of the colon appeared normal. CECT abdomen showed circumferential irregular wall thickening about 4cm proximal to anal verge with enlarged left inguinal, mesorectal and left internal iliac lymph node enlargement without perianal fat stranding [Table/Fig-6a,b]. Chest X Ray showed no evidence pulmonary carcinoma. Bone scan was normal and tumour marker i.e., Carcinoembryonic antigen was not elevated. The patient was negative for HIV, HbsAg and HCV.
CECT showing circumferential irregular wall thickening about 4 cm proximal to anal verge with enlarged left inguinal, mesorectal and left internal iliac lymph node enlargement without perianal fat stranding (a = Coronoal section; b= Axial section).
Prognosis of the condition was explained to the patient along with the morbidity and mortality associated with surgery. After obtaining informed consent, Abdomino Perineal Resection (APR) was done with permanent end colostomy. Post-op he was admitted in ICU for a day and was shifted to the ward. Post-op stay in hospital was uneventful. He was started on chemotherapy after 2 weeks. During the course of chemotherapy patient developed liver metastasis and he eventually succumbed to the condition 4 months later.
Discussion
Extrapulmonary small cell carcinomas are rare condition with incidence of 0.4% [1]. Oesophagus followed by colorectum is the most common primary site for small cell carcinomas [2]. Majority of anal canal malignancies are squamous cell carcinomas followed by adenocarcinoma and small cell carcinomas constitutes less than 1% [3]. Small cell carcinomas arise from argyrophilic cells in the basal layer of the squamous epithelium. They may be associated with ectopic production of a variety of hormones, including parathormone, secretin, granulocyte colony stimulation factor, and gastrin – releasing peptide and these cancers often present with systemic disease.
Most of the patients will have previous history of radiation and association with HIV infection has also been reported [4]. Conventional light microscopy reveals poorly differentiated malignancy but doesn’t reveal its organ of origin. This can further be diagnosed by Immunohistochemistry (IHC). Neuro endocrine markers like synaptophysin, CD 56 and CD57 and Thyroid Transcription Factor (TTF) – 1 are positive in such cases [5].
They are very aggressive tumours and most of the patients i.e., about 70% present with lungs and liver metastasis at the time of presentation even though the primary tumour involves mucosa or submucosa only [6]. The overall survival rate is less compared to squamous cell carcinoma [7].
Due to the rarity of this tumour entity, no standard treatment has been defined for gastrointestinal small cell cancers. Treatment is mainly done by chemoradiotherapy. It includes etoposide, cyclophosphamide, doxorubicin and cisplatin. Usually, there is good response to chemotherapy following which sometimes there is a relapse leading to rapid progression of the condition with median survival of 6 to 12 months. Radiotherapy is for palliation and loco regional control. Radical resection in the form of APR can be considered however it doesn’t significantly impact the progression of the disease. During the course of chemotherapy patient developed liver metastasis and succumbed to the condition 4 months later.
Conclusion
Small cell carcinoma is a very rare condition for which diagnosis is made by immunohistochemistry. Chemotherapy remains the best modality of treatment although there are chances of recurrence. Radiotherapy can be considered for local control of the disease. Prognosis remains poor because of the aggressive nature of the malignancy.
[1]. Cicin I, Karagol H, Uzunoglu S, Uygun K, Usta U, Kocak Z, Extra pulmonary small cell carcinoma compared with small-cell lung carcinoma: a retrospective single-centre studyCancer 2007 110(5):1068-76. [Google Scholar]
[2]. Huncharek M, Muscat J, Small cell carcinoma of the oesophagus. The Massachusets General Hospital experienceChest 1995 107:179-81. [Google Scholar]
[3]. Beahrs OH, Wilson SM, Carcinoma of the anusAnn Surg 1976 184(4):422-28. [Google Scholar]
[4]. Nakhara H, Moriya Y, Shinkai T, Hirota T, Small cell carcinoma of the anus in a HIV carrier: report of a caseSurg Today 1993 23(1):85-88. [Google Scholar]
[5]. Bernick PE, Klimstra DS, Shia J, Minsky B, Saltz L, Shi W, Neuro endocrine carcinomas of the colon and the rectumDis Colon Rectum 1994 37(7):635-42. [Google Scholar]
[6]. Balchandra B, Marcus V, Jass JR, Poorly differentiated tumours of the anal canal: a diagnostic strategy for the surgical pathologistHistopathology 2007 50(1):163-74. [Google Scholar]
[7]. Glynne-Jones R, Mawdsley S, Anal cancer: is neoadjuvant cisplatin chemotherapy or chemoradiotherapy friend or foe?Nat Clin Pract Oncol 2008 5(12):692-93. [Google Scholar]