Childbirth is an important event in the life of a woman and her family. Therefore, the quality of support a woman receives during the childbirth and labour is important [1]. Maintaining and improving health and decreasing maternal and neonatal complications and deaths in reproductive healthcare have received insignificant attention. Moreover, providing a high level of reproductive health and safe childbirth is among the rights of women. It should be also noted that lack of proper control of labour leads to complications for mothers and infants [2,3]. Childbirth as the most important consequence of labour is a process during the life of women and support is the key factor which makes it a positive experience [4]. Labour support is a term for caring or social support provided to women during labour and childbirth [5–7] including emotional and physical support and information provision [6]. During labour, the increased anxiety level enhances the pain perception by the mother and therefore, increases the labour duration and secretion of catecholamine which reduces the blood flow in the uterus. Consequently, the effectiveness of uterine contractions decreases [1]. Childbirth duration is one of the effective factors on pregnancy consequences and maternal and neonatal complications. Thus, with excessive prolongation of the childbirth, fetal or neonatal death risk, choking, infection and neural and physical damages in the infant increase and put the mother at risk of postpartum haemorrhage, infection, and psychological distress due to the anxiety, lack of sleep and fatigue [8–11]. The most important midwifery skill is the diagnosis of childbirth initiation and monitoring the process which can be solved through labour chart. Subsequently, low rate of maternal and infant mortality can be achieved by continuously applying a partogram in labour monitoring and giving importance to the role of midwife [12]. The partogram is an inexpensive instrument used as "early warning system" and can be helpful in primary decisions about transferring the mother, childbirth acceleration and pregnancy termination. The instrument increases the quality of maternal and neonatal monitoring and helps early diagnosis of problems. Further, the partogram is effective in the prolonged labour, and also in reducing surgical interventions and improving the neonatal consequences [13].
In order to improve and decrease the stress and anxiety of women during labour and cope with the childbirth pain, the emotional, physical and educational support of doulas can be used [1]. Using a doula is useful for both the mother and child, but the availability and associated costs may be an obstacle [14]. One way to increase the access to doula support is the instruction of midwifery students to serve this role [15] since personnel in maternity wards are insufficient in number [1]. Similar to doulas, midwifery students can provide support and care during childbirth and create a positive and successful experience in the mind of a parturient. It should be noted that the results of this paper were part of the results obtained in a larger study. Part of the results has been published [16].
According to the authors’ best knowledge, no such research has been carried out in the context of Iran. Therefore, we decided to conduct this study with the aims of increasing the rate of successful normal childbirth and reducing the emotional, spiritual, physical, and surgical damages to mothers and their infants.
Materials and Methods
This randomized controlled clinical trial was conducted from October 2013 to June 2015 at Fatemieh Hospital, Shahroud. In this study, supportive care was provided by the trained midwifery students. Forty midwifery students who had passed all the theoretical labour and delivery units were assigned to two groups, each with 20 individuals, using random sampling. The participants in the supportive group were trained for supportive care by a skilled midwife in six sessions of 60 minutes in the supportive care workshop during labour. During the sessions, the importance of continued support and types of supportive methods, including massaging back, belly and legs of the mother during labour, acupressure, aromatherapy, heat and cold therapy, encouraging the mother to walk during labour, and changing position, were pinpointed and taught to the students. In addition, the students participated in a two-hour workshop on how to use the partogram. The students in the non-supportive group (control group) only participated in the partogram workshop and were not trained for the supportive care.
Based on data from a previous study [17], the sample size in this study was selected as 50 women for each group with power = 90% and α = 0.05.
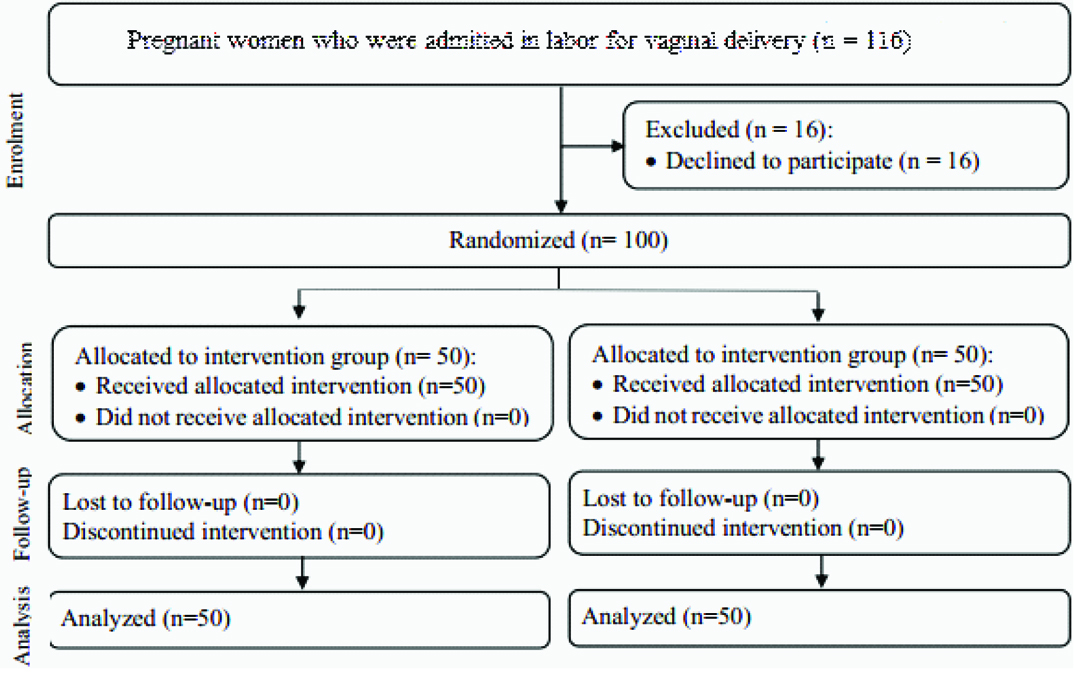
Pregnant women with expected normal childbirth were randomly assigned into the test and control group. Before starting the study, the allocation sequence was determined by one of the members of the research team, not involved in the sample selection, using a four-block randomized design. The participants were randomly assigned to the test and control group with a ratio of 1:1. The codes related to each participant were specified in opaque envelopes in order not to reveal the assignment procedure. Thus, the subjects were in A and B group according to the specified sequence [Table/Fig-1]. It should be noted that, prior to be assigned into groups, the students were randomly ordered. The data analyser was not aware of the interventions provided to the groups.
Flow diagram of the participants.
The inclusion criteria was, pregnant women aged 18-45 years, singleton live fetus and reactive NST on admission and the exclusion criteria was, presence of any other disease, psychological and depression, pregnancy complications such as preeclampsia, placental abruption and placenta previa vessels, fetal anomaly and the record of previous surgery on the uterus.
Data was collected using a four-section check list on demographic and obstetric characteristics, including the evaluation forms of the first and second stage of childbirth, infant information form and partogram form. To determine the content validity, the checklist was evaluated by ten members of the Faculty of Nursing and Midwifery academic staff and their opinions were applied. Moreover, the test-retest method was used to determine the reliably and the correlation coefficient was 0.92.
First, the researchers obtained two letters of introduction from Shahroud University of Medical Sciences and the Ethics Committee (IRCT2013111815443N1). A written consent was also obtained from every pregnant woman participating in the study. Then, the participants were assigned to one of the two groups based on the specified sequence and subsequently, asked to fill in the questionnaire on demographic and obstetric characteristics. In the test (supportive) group, students chose one of the 9 supports (massage, heat therapy, cold therapy, concentration and distraction, creative visualization, birth ball, acupressure, aromatherapy and music) as the mother wished and performed the support at least for 30 minutes in the active phase of labour. The routine care was performed in the control group. In both the groups, the partogram diagram was drawn to the subjects and the durations of the first and second stages were determined. Finally, the other parts of the questionnaire were completed by the end of the childbirth. The labour process was monitored by one of the midwifery personnel on the shift and the childbirth was performed by another midwife.
Statistical Analysis
Data analysis was performed using SPSS-21.0. Furthermore, the Kolmogorov-Smirnov test was used for normalized examination of the data. The descriptive statistics were used to describe the personal characteristics of the participants and the chi-square test, Fisher-exact test, independent t-test and Mann-Whitney test were used to compare the studied variables in the both groups. The significance level was considered less than 0.05.
Results
The information shown in [Table/Fig-2] indicates that both the study groups were homogeneous in terms of all the studied variables, except for age and instruction. The average age of the participants in the supportive and non-supportive group was 25.60 ± 4.51 years and 23.42 ± 4.51 years, respectively, and the difference was significant (p= 0.01). In addition, participants with high school diploma and higher education was significantly more in the supportive group than in the non-supportive group (p <0.001).
Demographic and obstetric characteristics of participants.
| characteristics | supportive group *n= 50 | non-supportive group *n= 50 | Statistic | p-value |
|---|
| Mother age, (year) | 25.60 ± 4.51 | 23.42 ± 4.51 | t= 2.41 | 0.01𠈂 |
| BMI | 25.14 ± 4.57 | 25.07 ± 3.91 | t= 0.08 | 0.93𠈂 |
| Occupation | | | χ2= 0.12 | 0.72§ |
| Housewife | 46 (92) | 45 (90) | | |
| Employed | 4 (8) | 5 (10) | | |
| Education | | | χ2= 14.49 | <0.0001§ |
| < Diploma | 17 (34) | 36 (72) | | |
| ≥ Diploma | 33 (66) | 14 (28) | | |
| Gestational age, week | 39.18 ± 1.01 | 39.42 ± 1.02 | z= -1.18 | 0.23‡ |
| Parity | 0.69 ± 0.95 | 0.65 ± 0.90 | z= 0.21 | 0.82‡ |
| Cervical dilation at admission time, cm | 2.96 ± 1.68 | 2.56 ± 0.74 | z= 1.54 | 0.12‡ |
* Mean ± SD, number (percent), 𠈂 independent t-test, ‡ Mann-Whitney test, § chi-square test
Comparison of the average labour time in both the groups showed that the average duration of the first stage was significantly shorter in the supportive group than in the non-supportive group (p<0.001). Also, the average duration of the second stage was shorter in the supportive group than in the non-supportive group, but this difference was not significant (p=0.06). Analysis of the results of the partogram showed that the number of participants in the supportive group who passed the alert line in their partogram diagram was significantly lower than that in the non-supportive group (p=0.002). The results of examining the Apgar score showed that the participants’ infants in the supportive group obtained better scores at minutes 1 and 5 compared to those in the non-supportive group(p<0.001 and p=0.04, significantly). However, no further differences were evident between the groups with regard to the other study variables [Table/Fig-3].
Comparing the groups in terms of labour and delivery outcomes.
| Outcome variables | supportive group *n= 50 | non-supportive group *n= 50 | Statistic | p-value |
|---|
| Duration of first stage of labour (from admission time to 10 cm cervical dilatation), in hours | 7.90 ± 3.55 | 11.46 ± 3.71 | t= -4.90 | <0.001𠈂 |
| Duration of second stage of labour, in minute | 52.47 ± 28.97 | 64.14 ± 34.67 | z= -1.82 | 0.06‡ |
| The need for oxytocin | | | χ2= 0.07 | 0.77§ |
| Yes | 7 (14) | 8 (16) | | |
| No | 43 (86) | 42 (84) | | |
| On the right side of the alert line | | | χ2= 9.33 | 0.002§ |
| Yes | 8 (16) | 22 (44) | | |
| No | 42 (84) | 28 (56) | | |
| Reached or crossed the action line | | | | 0.36|| |
| Yes | 1 (2) | 3 (6) | | |
| No | 49 (98) | 47 (94) | | |
| Type of delivery | | | | 0.36|| |
| Normal vaginal delivery | 49 (98) | 47 (94) | | |
| Caesarean section / vacuum | 1 (2) | 3 (6) | | |
| Apgar score in the first minute | 8.49 ±0.81 | 7.82 ± 0.93 | z= 3.84 | <0.001‡ |
| Apgar score in the fifth minute | 9.25 ± 0.70 | 8.92 ± 0.90 | z= 2.04 | 0.04‡ |
* Mean ± SD, number (percent), 𠈂 independent t-test, ‡ Mann-Whitney test, § chi-square test, || Fisher’s exact test
Discussion
In this study, the supportive care of the midwifery students shortened the durations of the first stage of labour, but had no significant effect on the duration of the second stage. Shahshahan et al., studied the effect of the presence of a support person and routine intervention on women during childbirth and concluded that the presence of a support person during labour decrease length of labour and improves labour outcomes [18], which was in line with the results of other studies (Khavandizadeh et al., Keshavarz et al., Kamali et al., [19–21]). In another study, Behmanesh et al., investigated the effect of heat therapy on pain intensity and duration of childbirth stages in 64 nulliparous patients and found that heat therapy significantly decreased the duration of the first stage of labour but had no significant effect on the duration of the second stage [22]. Yet in another study, Khresheh showed that there were no statistically significant differences in duration of labour between women who had support during labour and those who received no help (control group) [23]. The reason for the difference between the results of Khresheh’s study and those obtained in the present study is that, in Khresheh’s study, the duration of the first and second stages of labour were not considered separately. Further, Gentz et al., showed that complementary therapies such as massage therapy and music therapy were only influential on the labour first stage and their effectiveness on the second stage was controversial [24].
The point that distinguished the present study from other studies performed in this field was the inclusion of midwifery students to provide supportive care during labour. The supportive behaviors are one of the simplest, cheapest and most accessible methods to help pregnant women in labour progress and relieve their pain. Although, the best option to support mothers in childbirth stages is the presence of a trained attendant, considering the limited facilities and equipment available in hospitals in Iran, the educational and therapeutic staff and especially, the midwifery students, should undergo basic midwifery trainings related to the above mentioned cases and be responsible for these measures [21]. Since, the supportive cares are not included in the curriculum of midwifery students, training them in this field can promote the quality of clinical trainings and also the quality of provided health care. In the study conducted by Haghighi et al., the effect of infant resuscitation training on the knowledge and skills of midwifery students was investigated and the results confirmed that training can have a positive effect on their performance [25].
Another highlight of the present study was using the partogram in evaluation of labour progress. Students in both the supportive and non-supportive groups were trained, how to use the partogram before the start of the study. The findings showed that the number of participants whose partogram diagram passed the alert line was significantly lower in the supportive group than the in non-supportive group, indicating the fact that normal labour process in the supportive group subjects was higher than that in the non-supportive group subjects. Moreover, no significant difference was observed in prolonged labour between the supportive and non-supportive group (the partogram curve passed the action line), although 6% of subjects in the non-supportive group compared to 2% in the supportive group had prolonged labour. Kamalifard et al., showed in their study that the partogram curve has passed the action line in 2.5% of subjects in the control group, as compared to 0% of subjects in the intervention group [26]. It can be concluded that the use of support during labour reduces the childbirth process by decreasing length of labour.
In relation to the type of childbirth, the results show no significant difference between the two study groups. In support of this finding, the United States College of Obstetrics and Gynecology also found that active management of childbirth may decrease the labour duration, but cannot reduce the cesarean rates in all cases [8]. Although, the results of a few studies show the decreased cesarean rates in the supportive group [6,27], the lack of significant difference in terms of the childbirth type between the two study groups can be due to the use of the partogram and preventive measures, so that Vlachos et al., showed in their study that the new type of partogram have potential benefits such as decreasing the caesarean section rates [28]. Inconsistently, Lavender et al., in a review stated that there was no evidence of any benefit of using a partogram in caesarean section and suggested that further research is required to be conducted to evaluate the efficacy of partogram usage [29].
The other finding in this study was the improvement of Apgar scores at minutes 1 and 5 in the supportive group. In the studies by Khavandizadeh et al., and Keshavarz et al., the use of the supportive therapy was proved to significantly increase the Apgar score in the first minute [19,20]. It should be noted that the use of partogram was the strength of this study in evaluating labour process.
Limitation
The limitations of the present study were to perform unnecessary interventions by doctors and midwives in the maternity ward including amniotomy, vaginal exam, labor induction and episiotomy and the limited space in the maternity ward that these problems were partly resolved by negotiation and presentation explaining about the study.
Conclusion
The findings of this study showed that supportive care provided by the midwifery students can reduce duration of the first stage of labour and improve labour progress. It also has a positive impact on Apgar scores at minutes 1 and 5. Since the care was provided by the midwifery students, it seems that this low-cost strategy can be presented as an appropriate model for curriculum planning of midwifery students. In addition, the personnel performance during labour can be improved by the use of partogram. In fact, with a graphic image of the partogram, labour events become more substantial and quality of childbirth care can be improved. Therefore, it is recommended to train midwifery students on how to use partogram and consider them as supportive measures during labour.
Conflict of Interest
The authors declare that there is no conflict of interests regarding the publication of this paper.
* Mean ± SD, number (percent), 𠈂 independent t-test, ‡ Mann-Whitney test, § chi-square test
* Mean ± SD, number (percent), 𠈂 independent t-test, ‡ Mann-Whitney test, § chi-square test, || Fisher’s exact test