Masquerading Bundle Branch Block: A Poor Prognostic Sign Revisited
Suheil Dhanse1, Hashir Kareem2, Tom Devasia3, Mugula Sudhakar Rao4
1 Registrar, Department of Cardiology, KMC Manipal, Manipal University, Manipal, Karnataka, India.
2 Associate Professor, Department of Cardiology, KMC Manipal, Manipal University, Manipal, Karnataka, India.
3 Professor, Department of Medicine, KMC Manipal, Manipal University, Manipal, Karnataka, India.
4 Registrar, Department of Cardiology, KMC Manipal, Manipal University, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M Sudhakar Rao, Registrar, Department of Cardiology, Kasturba Medical College, Manipal University, Manipal-576104, Karnataka, India.
E-mail: msudhakar88@gmail.com
Masquerading bundle branch block is a rare but important finding on the Electrocardiogram (ECG). It is an indication of severe and diffuse conduction system disease and usually indicates poor prognosis. The precordial leads show a Right Bundle Branch Block (RBBB) pattern while the limb leads resemble a Left Bundle Branch Block (LBBB). This finding on an ECG is almost invariably associated with severe underlying heart disease. It is extremely important to be aware of this finding as it is a marker of poor cardiac outcomes. We report the case of a 68-year-old gentleman, who presented with progressive dyspnoea on exertion over three months. ECG showed a broad QRS complex with a RBBB pattern on the precordial leads and a LBBB pattern on the limb leads (suggestive of masquerading bundle branch block). A coronary angiogram revealed severe Triple Vessel Disease (TVD). The patient was scheduled for an early Coronary Artery By-Pass Grafting Surgery. However, his clinical condition deteriorated and he died while awaiting the surgery.
Congestive heart failure, Left anterior hemi fascicular block, Triple vessel disease
Case Report
A 68-year-old gentleman, a diabetic, presented with shortness of breath on exertion since 1 year. He reported progression of symptoms from New York Heart Association (NYHA) functional Class II to Class III over three months prior to presentation. His vital signs, at admission, were stable and a general physical examination was notable for an elevated jugular venous pressure. No cyanosis or pedal oedema was noted. A review of cardiovascular system revealed a systolic murmur best heard at the mitral area and a third heart sound. Auscultation of the lung fields revealed bilateral basal rales.
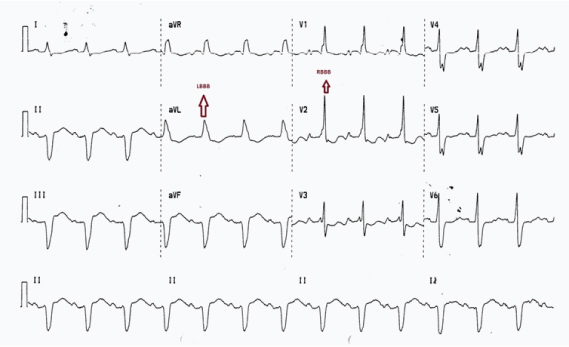
An ECG showed sinus rhythm with broad QRS complexes. The precordial leads showed a RBBB pattern with prominent R waves in leads V1 to V3 and deep S waves in V6. The limb leads however, resembled a LBBB with left axis deviation and negative, broad QS complexes in leads II, III and aVF. The S wave in lead one was blunted and lead aVL showed positive broad complexes with a faint M pattern [Table/Fig-1]. A review of another ECG, taken three months prior to presentation, showed narrower QRS complexes and more prominent S waves in lead I proving that the ECG findings had progressed over the duration [Table/Fig-2].
ECG showing broad QRS complexes with an RBBB pattern (rsR pattern) in the precordial leads V1 to V3. The limb leads show an LBBB pattern with left axis deviation and QS complexes in Leads II, III, aVF and M pattern in lead aVL. Blunting of the S wave in lead I noted.
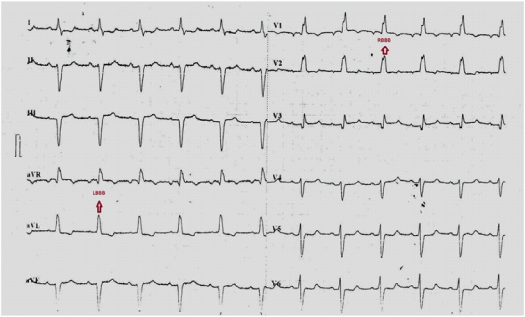
An older ECG of the same patient showing narrower QRS complexes with a more prominent S wave in lead I. The RBBB pattern in the precordial leads (rsR in V1,V2) and the LBBB pattern (M pattern in lead aVL & QS complexes in leads II, III, aVF) in the limb leads can be appreciated.
A 2D echocardiogram done, showed regional wall motion abnormality involving the anterior, and lateral walls and the interventricular septum. Severe Left Ventricular (LV) dysfunction was noted with an ejection fraction of 25% – 30% in addition to moderate mitral regurgitation. A chest X-ray revealed cardiomegaly with a Cardio Thoracic Ratio (CTR) of more than 55%. He underwent a coronary angiogram which revealed severe TVD. He was started on treatment for coronary artery disease and heart failure. He was scheduled for an early CABG Surgery. While still in the hospital, awaiting CABG, the patient’s clinical condition deteriorated rapidly and he developed a cardiac arrest. He could not be revived despite resuscitative measures.
Discussion
Electrocardiographic complex referred to as “masquerading bundle branch block” consists of the pattern of LBBB in the limb leads and RBBB in the unipolar precordial leads [1]. This pattern is actually a variation of a RBBB with LAFB. In typical cases of RBBB with Left Anterior Fascicular Block (LAFB), the QRS axis lies between -80 and -120 degrees. However, in some cases, due to predominant left ventricular forces, the axis remains around -60 degrees. In such cases the S wave in lead I tend to be small or absent so that the ECG resembles an LBBB on the limb leads. Usually this is the result of an advanced LAFB or focal block on the anterolateral wall of the LV due to myocardial infarction or fibrosis. Similarly, in some cases, the S wave may be absent in the precordial leads V5 and V6. This is often referred to as “precordial masquerading” while absent S in lead I is called “standard masquerading” [2]. The S wave in RBBB represents the terminal forces produced by the delayed activation of the Right Ventricles (RV). If the conduction of the anterosuperior wall of the LV is significantly delayed (due to the diseased LV), the terminal forces from the LV will prevail over those from the RV, thereby diminishing the S wave [2]. This explains why patients with masquerading bundle branch block have poor prognosis as would be expected in a patient with severe disease of the LV. Kaimoto et al., reports a similar case of a patient who died suddenly 9 months after the diagnosis of a masquerading Bundle Branch Block (BBB) [3]. Unfortunately, our patient had an even worse prognosis, probably because the condition went undetected and untreated. This report highlights the importance of identifying this poor prognostic marker correctly and providing early treatment for these patients.
Conclusion
Masquerading bundle branch block is a condition in which the limb leads of the ECG show an LBBB pattern and the precordial leads show an RBBB pattern. It is usually associated with severe disease of the left ventricle and is a marker for poor prognosis. It is important to promptly identify and treat this condition at the earliest.
[1]. Unger PN, Lesser ME, Kugel VH, Lev M, The concept of masquerading bundle-branch block: an electrocardiographic–pathologic correlationCirculation 1958 17:397-409. [Google Scholar]
[2]. Elizari MV, Baranchuk A, Chiale PA, Masquerading bundle branch block: A variety of right bundle branch block with left anterior fascicular blockExpert Rev Cardiovasc Ther 2013 11(1):69-75. [Google Scholar]
[3]. Kaimoto S, Kawasaki T, Taniguchi T, Kawasaki S, Kamitani T, Sugihara H, Masquerading bundle branch block as a marker of poor prognosisJournal of Cardiology Cases 2013 8(1):57-59. [Google Scholar]