Introduction
Oxidative stress is emerging as a causative factor for various diseases, including Cardiovascular Diseases (CVD). Moreover, the antioxidant defence decline, while oxidative stress enhanced by aging especially in geriatrics [1,2].
An oxygen molecule containing an unpaired electron in its outer orbit-produced by different processes of oxidation-is known as Reactive Oxygen Species (ROS). Free radicals are usually unstable and highly reactive due to unpaired electron. ROS contribute to different chemical reactions which eventually escort to divers pathological conditions [3,4]. Moreover, oxidative stress, defined as a disturbance in the balance between the production of ROS and antioxidant defenses [5]. Oxidative stress strongly influence lipids, protein and DNA in the central nervous system; besides ROS generated pathological damage increases with age especially in the last quarter of life span [6]. Furthermore, antioxidant defense system deteriorates while enhancing accumulations of ROS due to lipid peroxidation and altered enzyme activities in old age [7,8]. Essential hypertension is associated with impaired antioxidants status and the formation of free radicals [1]. Oxidative stress is associated with aging, which ultimately causes deterioration of muscles by two fundamental biological processes: increased production of ROS and decline in antioxidant enzymes. However, mild nonexhaustive exercise causes mild oxidative stress that stimulates the expression of certain antioxidant enzymes [9]. Oxidative stress plays an important role in adverse effects of obesity in CVD [10].
Severity of atherosclerosis is directly related to dyslipidaemia, hypertension and lipid peroxidation [11]. Oxidative stress might be considered as a novel therapeutic target for treating essential hypertension [12]. Blood pressure is affected by multiple dietary factors; therefore, modifications of diet can induce positive changes in blood pressure of both hypertensive patients and normotensive subjects [13]. Regular practise of yoga can maintain antioxidant level of the body even, in stressful conditions [14]. Exercise induces Super Oxide Dismutase (SOD) which serves to minimize superoxide anions (O2-) with nitrous oxide (NO) consequently benefits vascular functions [15]. Commencement of moderately sports activities, quitting smoking, maintaining blood pressure and body weight are separately associated with lower rates of death from all causes in middle and old age [16]. Physically unfit men are more likely to suffer from CVD than physically fit ones [17].
Therefore, the present study was designed to assess the effects of lifestyle modifications on oxidative stress, blood pressure and lipid profile in normotensive elderly subjects.
Materials and Methods
Study Population
This interventional study included 74 healthy elderly subjects (43 males and 31 females) between 60 to 80 years of age. All elderly normotensive subjects were selected from Santosh Medical College and Hospital, Ghaziabad Uttar Pradesh, India. The study was conducted in the Santosh Medical College and Hospital, Ghaziabad, India from July 2014 to November 2015. Written consent of the participants in the local language was taken after clearly narrating the purpose and nature of research. Inclusion criteria for the study was normal blood pressure <140/90 mm Hg [18], body mass index 18.5-25 kg/m2, non-smokers and non- alcoholic. Participant suffering with any kind of physical disability, chronic disease or taking any type of medicines was excluded from the study.
Lifestyle Modifications
Lifestyle interventions were implicated for three months time period [19] All participants were assigned to do the Nadi Shodhan Pranayama [20]. (forced one side nostril breathing) on an empty stomach for 20 minutes, early morning 6 days in a week under the supervision of yoga instructor. Along with it morning walk [16] of 2 miles daily for 6 days in a week and minimum sleep [21] of 5 to 6 hours was advised. In addition to it reduced intake of dietary salt [22] up to 100 m eq/day, lowering fat [22] intake up to 44 to 77 g and increased intake of water [23] 2 to 3 liters per day were suggested to all participants. An orientation program was organized before starting the research program for all the participants for better understanding of the lifestyle interventions. All the participants were instructed to come for 1 hour, early in the morning from 6am to 7am for 6 days in a week. The protocol of lifestyle modifications included 20 minutes yoga followed by 2 miles walk under the supervision of an authorized instructor. Investigators made interaction with every participant weekly; in addition, orientation programs were organized every month for the participants to keep their interest in research.
Measurements
All of the measurements and biochemical parameters were recorded early in the morning between 6 to 8 am with an empty stomach, twice, one at baseline and another after three months lifestyle modifications.
Blood Pressure
The participants were requested to sit in supine position comfortably and quietly for 10 minutes. After that blood pressure was recorded three times at the interval of 10 minutes by auscaltatory method with the help of the Sphygmomanometer (manufactured by Diamond Regular, India) [24].
Evaluation of Lipid Profile
Serum concentration of Total Cholesterol (TC), Triglycerides (TG) and HDL were estimated by CHOD-POD method, GPO-PAP method and CHOD-POD/ Phosphotungstate method respectively by using commercial kits manufactured by Erba Mannheim; Low Density Lipids (LDL) was calculated by using Friedewald’s formula [25].
Estimation of Oxidative Stress
Oxidative stress markers Glutathione (GSH) and SOD were investigated by kits (Qayee-Biotechnology Co. Ltd) using Enzyme Linked Immunosorbent Assay (ELISA) [26,27]. Malondialdehyde (MDA) was estimated (TBARS method) by TBARS kit (Cayman chemical company) [28].
Statistical Analysis
The obtained data was expressed as Mean±SD (Standard deviation). Paired students t-test was used to analysis, statistical significance of data obtained before and after lifestyle modification. An association of oxidative stress markers (GSH, SOD and MDA) and Blood Pressure (SBP, DBP) was analysed using Pearson correlation coefficient test. A p-value < 0.05 was considered statistically significant. IBM SPSS Statistics 21.0 manufactured by IBM USA was used for entire calculations.
Results
Total 74 elderly subjects aged 65.14±4.52 years, both males and females, completed the lifestyle modification program for three months. However, there was no significant change between the findings of males and females.
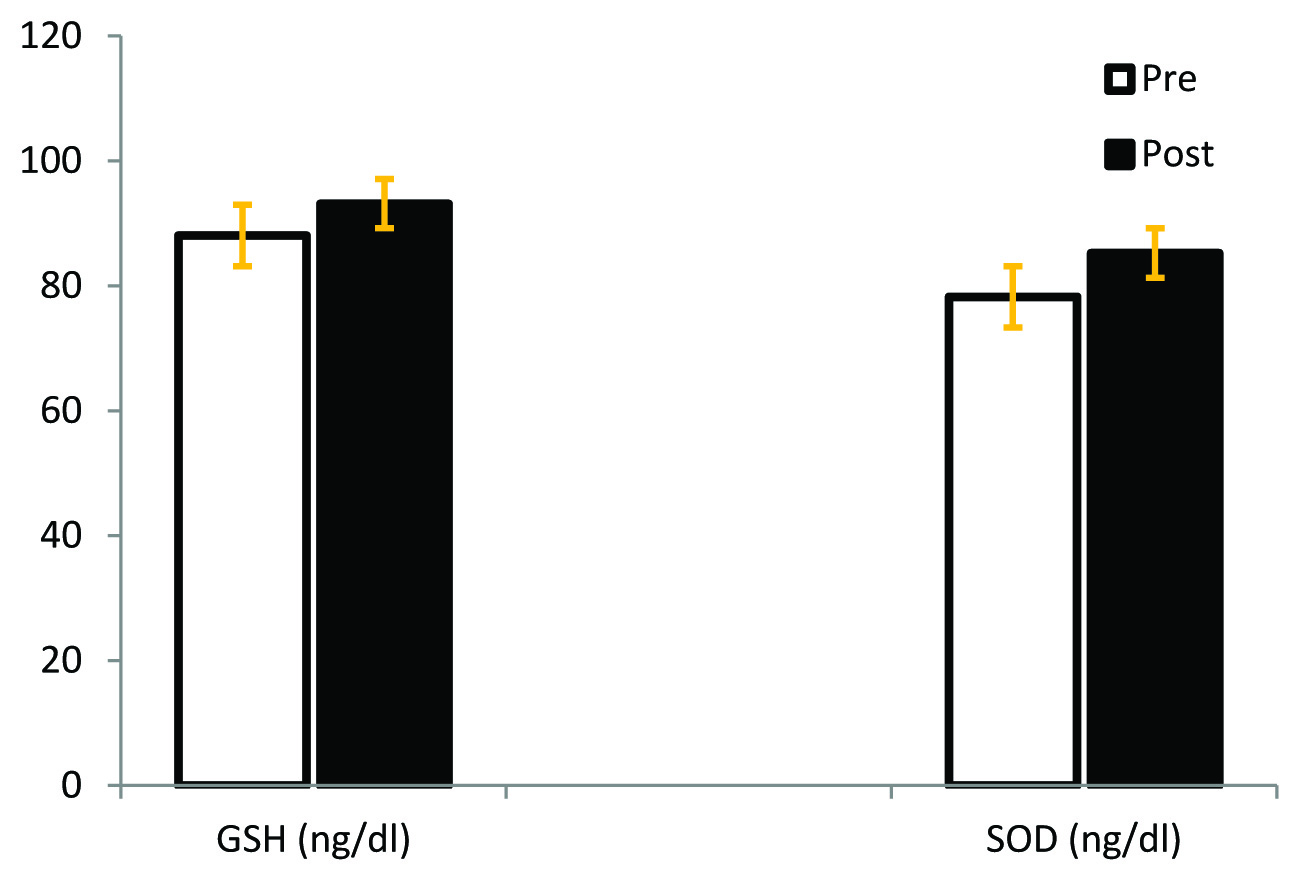
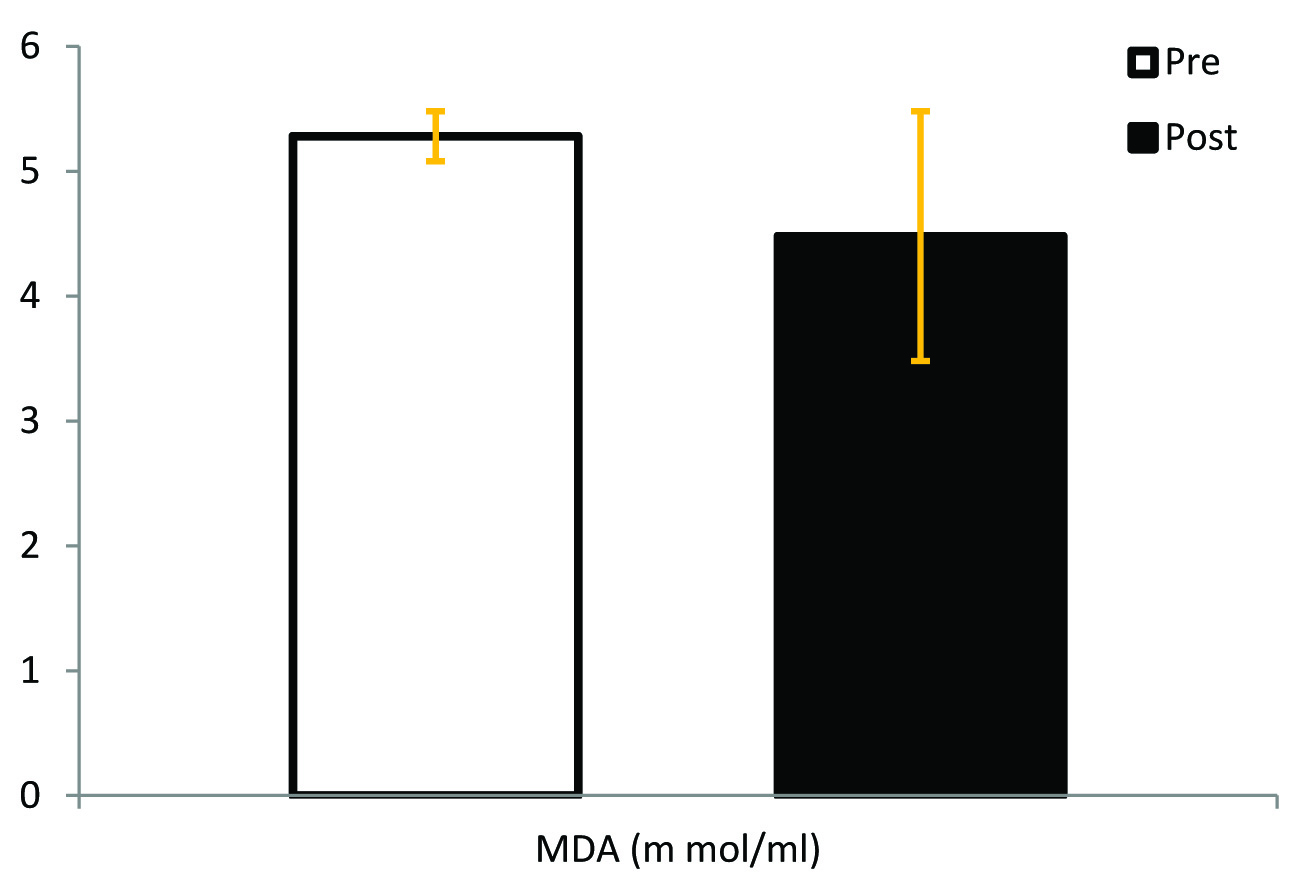
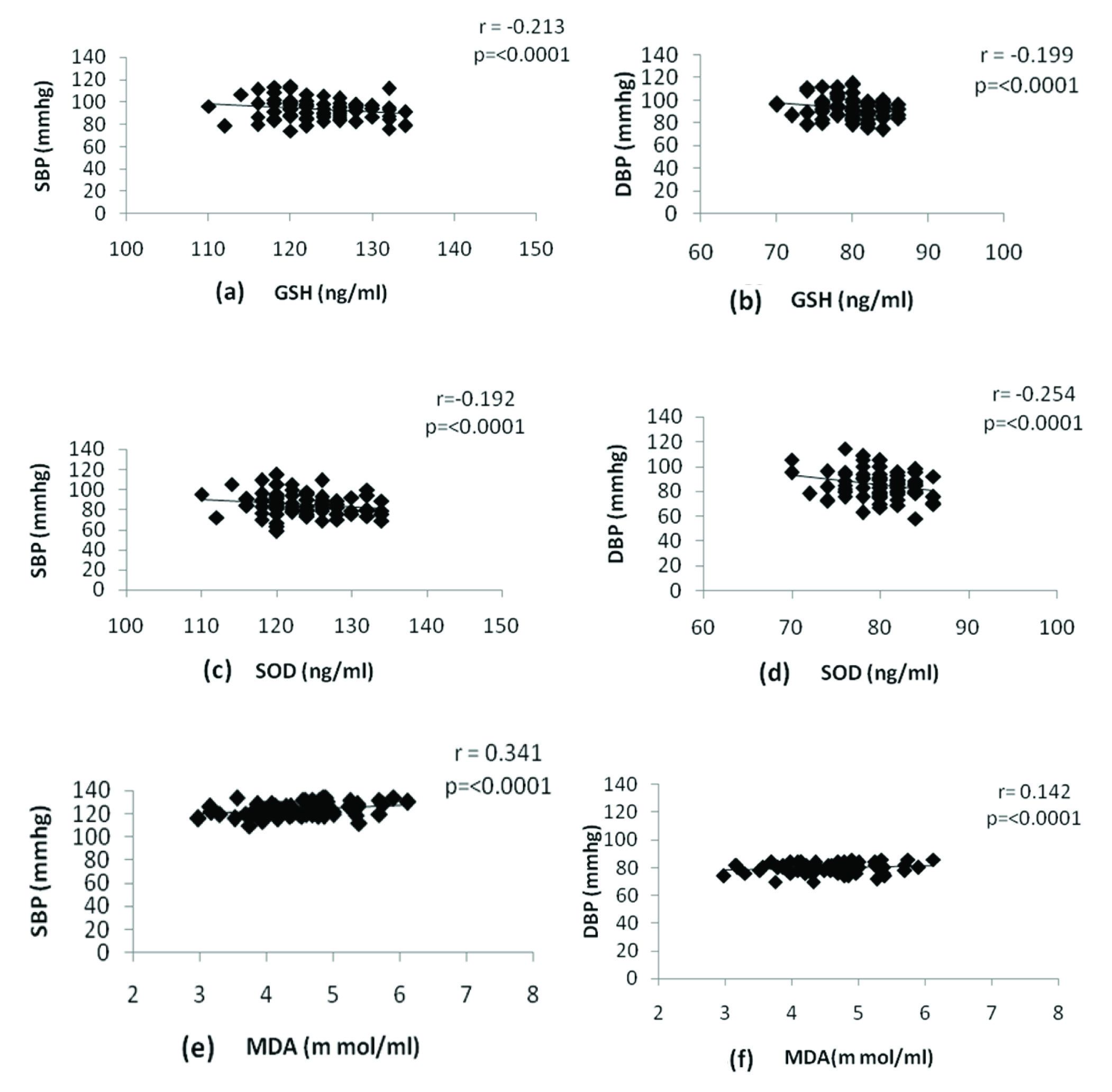
[Table/Fig-1] shows significant reduction in oxidative stress markers as baseline values of GSH increased from 88.03±9.58 ng/ml to 93.12±9.17 ng/ml (p < 0.0001) and SOD enhanced from 78.22±11.97 ng/ml to 85.22±11.08 ng/ml (p<0.0001). On the other hand [Table/Fig-2] demonstrates the baseline values of MDA decreased significantly from 5.28±0.52 m mol/ml to 4.48± 0.69 m mol/ml (p < 0.0001). The results further reveal that GSH and SOD have negative while MDA has a positive correlation with both Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP) [Table/Fig-3].
Changes in antioxidant status after lifestyle modifications. Pre- Before lifestyle modifications, Post – After lifestyle modifications, n= 74, GSH-Glutathione (p<0.0001), SOD- Superoxide dismutase (p<0.0001).
Changes in MDA after lifestyle modifications. Pre- Before lifestyle modifications, Post – After lifestyle modifications, n= 74, MDA- Malondialdehyde (p<0.0001).
Pearson correlation between SBP or DBP and GSH, SOD, and MDA in normotensive elderly subjects after following lifestyle modification. SBP-Systolic blood pressure, DBP-Diastolic blood pressure.
[Table/Fig-4] shows significant decrease of weight (p <0.0001) and body mass index (p <0.0001) after following lifestyle interventions. A significant decline of 4.31±0.57mmHg and 1.73± 1.05 mm Hg has been observed SBP and DBP, respectively. Besides, we observed significant reduction in mean arterial pressure (MAP); however, change in heart rate was not significant (p <0.1259). In addition, we observed a significant decrease of TC (p <0.0001), TG (p <0.0001) and LDL (p <0.0001), whereas a significant increase of HDL (p <0.0001) [Table/Fig-4].
Comparison of pre and post lifestyle modifications values.
| Parameters | Before Lifestyle modifications, n=74 | After Lifestyle modifications, n=74 | p-value |
|---|
| Weight (kg) | 60.73 ± 7.98 | 57.53 ± 7.38 | <0.0001* |
| BMI (kg/m2) | 22.4 ± 2.01 | 21.25 ± 1.76 | <0.0001* |
| Systolic blood pressure (mmHg) | 127.92 ± 6.05 | 123.59 ± 5.48 | <0.0001* |
| Diastolic blood pressure (mmHg) | 81.65 ± 4.73 | 79.92 ± 3.68 | <0.0002* |
| MAP (mmHg) | 97.01 ± 4.48 | 94.51 ± 3.6 | <0.0001* |
| HR (rpm) | 78.3 ± 5.73 | 77.6 ± 6.14 | <0.1259 |
| TC (mg/dl) | 204.31 ± 28.94 | 191.98 ± 23.23 | <0.0001* |
| TG (mg/dl) | 119.36 ± 23.89 | 111 ± 20.2 | <0.0001* |
| HDL (mg/dl) | 44.13 ± 6.53 | 47 ± 7.06 | <0.0001* |
| LDL (mg/dl) | 135.3 ± 24.38 | 122.72 ± 22.45 | <0.0001* |
Data presented as Mean ± SD, MAP= mean arterial pressure, HR= heart rate, TC= total cholesterol, TG= triglycerides, HDL= high density lipids, LDL= low density lipids, SD= standard deviation of Mean. * = highly significant.
Discussion
It is well documented that oxidative stress is a harmful condition in which there is a loss of balance between oxidants and antioxidants as oxidants increased beyond the antioxidant status [4]. Moreover, uncontrolled ROS are the root cause of the diverse pathological conditions; various chronic diseases have been affected by ROS to different degrees [29,30]. The results of the current study showed that three months lifestyle modifications have significantly increased the antioxidant level of healthy elderly subjects [Table/Fig-1]. Previous studies of Gordon et al., Cheong et al., and Sinha et al., have shown similar enhancement in GSH and SOD [14,31,32]. SOD reacts with superoxide radical (O2--) and converts it into hydrogen peroxide (H2O2) and oxygen (O2). However, GSH is an enzyme which detoxifies hydrogen peroxide into water (H2O) and alcohol (ROH); this process is facilitated by reduced GSH which gets converted into oxidized GSH [33]. This enhancement of antioxidants seems to be due to the reason that exercise causes mild increase of ROS, which in turn enhances the expression of various antioxidants by activating redox-sensitive singling pathways [9]. Further, increased SOD causes decreasing O2-- activity which in turn enhances the endothelial derived NO and results enhanced expression of extracellular SOD [15]. Exercise induces various structural changes and remodelling of vascular wall results in improved functioning of endothelial cells [34]. Exercise stimulates endothelium to enhance the production of NO along with increased level of SOD that rectify the O2-- which further increases the bioavailability of NO [35]. Decreased level of antioxidant status has been found to be associated with hypertension since different free radicals while antioxidants play an important role in the progress of CVD [1]. Hence, improvements in SOD and GSH level in the present study after lifestyle modification program may be helpful in reducing the risk of CVD. Moreover, increased level of antioxidant through lifestyle modification might reduce the effects of aging as enhanced antioxidant level leads to decreasing the rate of deterioration of muscles, lipids peroxidation, CVD, target organ disease, DNA damage and aging process [6]. Age related oxidative damage cannot be controlled by antioxidant defense mechanisms; however, changes in lifestyle can reduce the oxidative stress [36]. Apart from this antioxidants level enhancement by lifestyle modifications is more beneficial as the reaction constant of superoxide with vitamin E and vitamin C is far less than the reaction constant of superoxide and SOD [37]. On the other hand, ROS target the lipids and induce lipid peroxidation process; which is a chain reaction and results in cell death.
Moreover, MDA is the end product of polyunsaturated fatty acid peroxidation and leads to further enhancement of lipid peroxidation. Nonetheless, MDA promotes various deteriorating cellular reactions which results in destruction of proteins and DNA. Therefore, increased level of MDA persuades aging process leading to damage to the structure of bio-molecules and various pathological disorders [38,39]. Age related changes cause elevation of ROS which further enhances the level of lipid peroxidation and reduces the level of antioxidants especially in elderly hypertensive. Moreover, there has been found a high level of MDA whereas decrease level of antioxidants Catalase and GSH in elderly people [8]. The reduction of MDA level, as observed in our study, is consistent with findings of previous studies of Patil et al. and Singh et al., [40,41]. This decrease of MDA may be due to improvement of antioxidant defense system as increased level of antioxidants decrease the ROS which reflects a reduction of lipid peroxidation [31]. Further, the decline of MDA may be helpful in decreasing risk for CVD as MDA, represents an independent indicator of risk for patients with stable coronary artery disease [42]. Furthermore, the present findings demonstrate a Negative correlation between SOD and GSH with both SBP and DBP. On the other hand, MDA has shown positive correlation with SBP as well as DBP, which is similar to previous studies where researchers showed the same correlation oxidative stress and blood pressure [12,31,34,40,41]. These changes seem to be due to regular physical exercise which decreases the age induced endothelial dysfunction – dependent vasorelaxation by an increment in nitric oxide release due to decreased oxidative stress [35,43]. In addition, correlation of blood pressure with oxidative stress as observed in our study may be due to increased level of ROS leads to destruction of endothelium, impaired endothelial functions, decrease vascular NO; though, various interventions which increase the NO production and reduce the genesis of superoxide have substantially decreased risk of CVD and vascular functioning in CVD patients in clinical studies [44].
Moreover, the results of the present study showed that lifestyle modifications produced a significant decline in SBP as well as DBP [Table/Fig-3]. The obtained results in the present study are very similar to earlier studies where LP Svetkey et al., Jiro et al., and Murthy et al., have shown a significant reduction in blood pressure after the implications of lifestyle interventions [45–47]. To the best of our knowledge, this is the first study of its kind, including yoga as well as walking modulation together with dietary restrictions. Yoga controls blood pressure by regulating hypothalamic pituitary adrenal axis and sympathetic nervous system; along with it yoga reduces stress, which stimulates parasympathetic activation and alteration in baroreceptors sensitivity that ultimately decreases BP in normotensive and hypertensive [48,49]. Physical exercise helps in the remodelling of arteries, improves bioavailability of NO as well as dilatation of smooth muscles. This may be due to improvement in antioxidants level of the body as ROS interrupt the synthesis and functioning of NO. Moreover, refined vascular function along with up regulated phosphorylation might be the cause of improved blood pressure [50]. Further, best control over blood pressure can be attenuated when multiple lifestyle modifications are integrated simultaneously [51].
These findings suggest that reduction in oxidative stress has a positive effect on blood pressure; and lifestyle modifications would be beneficial for elderly normotensive people. Lifestyle modification technique-even of short span has been found effective in reducing in TC, Triglycerides, LDL and increasing HDL [52]. Similarly, our study has shown a considerable decrease in lipid profile except increase in HDL levels. Previous studies have shown similar results as Paeolatti V et al., Yukihito H et al., recorded remarkable decreases in TC, TG and LDL while enhancement in HDL after life style modifications [35,53]. Similarly, Agarwal et al., Agte et al., and Lorengo AG et al., showed decrease in lipid profile after yoga practice [30,36,54]. Further, this decline of lipid profile may be due to a low caloric diet which induces weight loss reduces oxidative stress through improving glucose metabolism which may lead to decreased adiposity and cytokines secretion [55]. Moreover, the decrease of lipids profile might reduce the risk for CVD in elderly subjects as increased levels of lipids are independent risk factors of coronary heart disease; however, reducing lipids with exercise can decrease risk for coronary heart disease [37].
Limitation
In the present study, the small sample size was the most important limitation in assessment of lifestyle modifications in male and females separately. It warrants for more number of studies on a large number of populations to examine the effect on male and female individually to provide guidelines for lifestyle modifications.
Conclusion
The findings of the present study show that lifestyle modification is helpful in reducing cardiovascular disease risk but also assuring for good health by decreasing oxidative stress level along with lipid profile. Further, all these modifications are easy to follow. However, more studies are required to make a generalized lifestyle modification program for normotensive elderly subjects.
Data presented as Mean ± SD, MAP= mean arterial pressure, HR= heart rate, TC= total cholesterol, TG= triglycerides, HDL= high density lipids, LDL= low density lipids, SD= standard deviation of Mean. * = highly significant.
[1]. Kashyap M K, Yadav V, Sherawat BS, Jain S, Kumari S, Khullar M, Different antioxidants status, total antioxidant power and free radicals in essential hypertensionMolecular and Cellular Biochemistry 2005 277:89-99. [Google Scholar]
[2]. Banarjee S, Bhattacharya S, Oxidative stress parameters and antioxidant status in middle aged amd elderly subjects: an age-related comparative studyInt. J. Bioassays 2014 3(07):3131-36. [Google Scholar]
[3]. Kunwar A, Priyadarsini KI, Free radicals, oxidative stress and importance of antioxidants in human healthJ Med Allied Sci 2011 1(2):53-60. [Google Scholar]
[4]. Yoshikawa T, Naito Y, What is oxidative stress?JMAJ 2002 45(7):271-76. [Google Scholar]
[5]. Betteridge DJ, What is oxidative stress?Meatbolism 2000 49(2 Suppl 1):3-8. [Google Scholar]
[6]. Radak Z, Zhao Z, Goto S, Koltai E, Age-associated neuro degeneration and oxidative damage to lipids, proteins and DNAMolecular Aspect of Medicine 2011 32(4-6):305-15. [Google Scholar]
[7]. Hybertson BM, Gao B, Bose SK, McCord JM, Oxidative stress in health and disease: The therapeutic potential of Nrf 2 activationMolecular Aspects of Medicine 2011 32:234-46. [Google Scholar]
[8]. Prashant AV, Harishchandra H, D’souza V, D’souza B, Age related changes in lipid peroxidation and antioxidants in elderly peopleIndian Journal of Clinical Biochemistry 2007 22(1):131-34. [Google Scholar]
[9]. Ji LL, Exercise-induced modulation of antioxidant defenseNY Ascad Sci 2002 959:82-92. [Google Scholar]
[10]. Keaney JF, Larson MG, Vasan TS, Wilson PW, Lipinska I, Corey D, Obesity and systemic oxidative stress: clinical correlates of oxidative stress in the Framingham StudyArterioscler Thromb Vasc Biol 2003 23(3):434-39. [Google Scholar]
[11]. Ogunru PS, Balogun WO, Fadero FF, Idogun TS, Oninla SO, Elemile PO, Plasma lipid peroxidation and total antioxidant status among dyslipidaemic and hypertensive Nigerians with high risk of coronaryc heart diseaseWest Afr J Med 2009 28(2):87-91. [Google Scholar]
[12]. Rodrigo R, Prat H, Passalacqua W, Araya J, Guichard C, Bachler JP, Relationship between oxidative stress and essential hypertensionHypertens Res 2007 30:1159-67. [Google Scholar]
[13]. Appel LJ, Brands MW, Daniels SR, Karanja N, Elmer PJ, Sacks FM, Dietary approaches to prevent and treat hypertension a scientific statement from the American heart associationHypertension 2006 47(2):296-308. [Google Scholar]
[14]. Sinha S, Singh SN, Monga YP, Ray US, Improvement of glutathione and total antioxidant status with yogaThe Journal of Alternative and Complementary Medicine 2007 13:1085-90. [Google Scholar]
[15]. Fukai T, Siegfried MR, Fukai MU, Cheng Y, Kojda G, Harrison DG, Regulation of the vascular extracellular superoxide dismutase by nitric oxide and exercise trainingJ Clin Invest 2000 105:1631-39. [Google Scholar]
[16]. Paffenbarger RS, Hyde RT, Wing AL, Lee IM, Jung DL, Kampert JB, The association of changes in physical-activity level and other lifestyle characteristics with mortality among menN Eng J Med 1993 328(8):538-45. [Google Scholar]
[17]. Blair SN, Kohl HW, Barlow CE, Paffenbarger RS, Gibbons LW, Macera CA, Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy menJAMA 1995 273(14):1093-98. [Google Scholar]
[18]. Head GA, Mihailidous AS, Duggan KA, Beilin LJ, Berry N, Brown MA, Definition of ambulatory blood pressure targets for diagnosis and treatment ofhypertension in relation to clinic blood pressure: prospective cohort studyBMJ 2010 340:c1104 [Google Scholar]
[19]. Ohta M, Nanri H, Matsuhima Sato Y, Ikeda M, Blood pressure-lowering effects of lifestyle modification: possible involvement of nitric oxide bioavailabilityHypertens Res 2005 28(10):779-86. [Google Scholar]
[20]. Subbalakshmi NK, Saxena SK, Urmimala D’Souza UJA, Immediate effect of ‘nadi-shodhan pranayama’ on some selected parameters of cardiovascular, pulmonary and higher functions of brainThe Journal of Physiological Sciences 2005 18(2):10-16. [Google Scholar]
[21]. Tochikubo O, Ikeda A, Miyajima E, Ishii M, Effects of insufficient sleep on blood pressure monitored by a new multi biomedical recorderHypertension 1996 27(6):1318-24. [Google Scholar]
[22]. Whelton PK, Apeel LJ, Espeland MA, Applegate Wb, Etinnger WH, Kostis JB, Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of nonpharmacologic interventions in the elderlyJAMA 1998 279(11):839-46. [Google Scholar]
[23]. Spigt MG, Knottnerus JA, Westerterp KR, Olde Rikkert MG, Schayck CP, The effects of 6 months of increased water intake on blood sodium, glomerular filtration rate, blood pressure, and quality of life in elderly (aged 55-75) menJ Am Geriatr Soc 2006 54(3):438-43. [Google Scholar]
[24]. Ogedegbe G, Pickering T, Principles and techniques of blood pressure measurementCardiol Clin 2010 28(4):571-86. [Google Scholar]
[25]. Burtis CA, Ashwood ER, Bruns DE, Teitz fundamentals of clinical chemistry6th ed:422-24. [Google Scholar]
[26]. Emokpae MA, Uadia PO, Gadzama AA, Correlation of oxidative stress and inflammatory markers with the severity of sickle cell nephropathyAnn African Med 2010 99(3):141-46. [Google Scholar]
[27]. Onorato JM, Thorpe SR, Baynes JW, Immunohisto chemical and ELISA assays for biomarkers of oxidative stress in aging and diseaseAnn N Y Acad Sci 1998 854:277-90. [Google Scholar]
[28]. Mossa MM, Bushra MM, Salih MR, May NY, Estimation of malondialdehyde as oxidative factor & glutathione as early detectors of hypertensive pregnant womenTikrit Medical Journal 2009 15(2):63-69. [Google Scholar]
[29]. Alfadda AA, Sallam RM, Reactive oxygen species in health and diseaseJ Biomed Biotechnol 2012 2012:936486 [Google Scholar]
[30]. Aggarwal NT, Makielski JC, Redox control of cardiac excitabilityAntioxid Redox Singal 2013 18(4):432-68. [Google Scholar]
[31]. Gordon LA, Morrison EY, McGrowder DA, Young R, Fraser YT, Zamora EM, Effect of exercise therapy on lipid profile and oxidative stress indicators in patients with type 2 diabetesBMC Complement Altern Med 2008 8:21 [Google Scholar]
[32]. Cheong KJ, Lim SA, Antioxidant effects of regular yoga training on the healthy university students controlled clinical trialJ Yoga Phys Ther 2012 2(6):2157-7595. [Google Scholar]
[33]. Powers SK, Jackson MJ, Exercise-induced oxidative stress: cellular mechanisms and impact on muscle force productionPhysiol Rev 2008 88(4):1243-76. [Google Scholar]
[34]. Kojda G, Hambrecht R, Molecular mechanism of vascular adaptations to exercise. Physical activity as an effective antioxidant therapy?Cardiovasc Res 2005 67:187-97. [Google Scholar]
[35]. Higashi Y, Sasaki S, Kurisu S, Yoshimizu A, Regular aerobic exercise augments endothelium-dependent vascular relaxation in normotensive as well as hypertensive subjects role of endothelium-derived nitric oxideCirculation 1999 100:1194-202. [Google Scholar]
[36]. Lorenzo AG, Errol YM, Donovan AM, Ronald Y, Yeiny TPF, Effect of exercise therapy on lipid profile and oxidative stress indicators in patients with type 2 diabetesBMC Complementary and Alternative Medicine 2008 8:21 [Google Scholar]
[37]. Stefanick ML, Mackey S, Sheehan M, Ellsworth N, Haskell WL, Wood PD, Effects of diet and exercise in men and postmenopausal women with low levels of HDL cholesterol and high levels of LDL cholesterolN Eng J Med 1998 339(1):12-20. [Google Scholar]
[38]. Gawl S, Wardas M, Niedworok E, Wardas P, Malondialdehyde (MDA) as a lipid peroxidation markerWiad Lek 2004 57(9-10):453-55. [Google Scholar]
[39]. Ayala A, Munoz MF, Arguelles S, Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenalOxidative Medicine and Cellular Longevity 2014 2014:36043831 pages [Google Scholar]
[40]. Patil SG, Dhanakshirur GB, Aithala MR, Naegal G, Das KK, Effect of yoga on oxidative stress in elderly with grade-I hypertension: a randomized controlled studyJ Clin Diabn Res 2014 8(7):BC04-07. [Google Scholar]
[41]. Singh S, Malhotra V, Singh KP, Sharma SB, Madhu SV, Tandon OP, A preliminary report on the role of yoga asanas on oxidative stress in non-insulin dependent diabetes mellitusIndian J Clin Biochem 2001 16(2):216-20. [Google Scholar]
[42]. Walter MF, Jacob RF, Jeffers B, Ghadanfar MM, Preston GM, Buch J, Serum levels of thiobarbituric acid reactive substances predict cardiovascular events in patients with stable coronary artery disease A longitudinal analysis of the prevent studyJ Am Coll Cardiol 2004 44(10):1996-2002. [Google Scholar]
[43]. Taddei S, Galetta F, Virdis A, Ghiadoni L, Salvetti G, Franzoni F, Physical activity prevents age-related impairment in nitric oxide availability in elderly athletesCirculation 2000 101(25):2896-901. [Google Scholar]
[44]. Munzell T, Goril T, Bruno RM, Taddei S, Is oxidative stress a therapeutic target in cardiovascular disease?European Heart Journal 2010 31:2741-49. [Google Scholar]
[45]. Svetkey LP, Erlinger TP, Vollmer WM, Feldstein A, Cooper LS, Appel LJ, Effect of lifestyle modifications on blood pressure by race, sex, hypertension status, and ageJournal of Human Hypertension 2005 19:21-31. [Google Scholar]
[46]. Jiro M, Hiroshi I, Sanae H, Kazuo T, Tsuguru H, Tetsuo N, Susumu S, Low frequency regular exercise improves flow- mediated dilatation of subjects with mild hypertensionHypertens Res 2005 28:315-21. [Google Scholar]
[47]. Murthy SN, Rao NS, Nandkumar B, Kadam A, Role of naturopathy and yoga treatment in the management of hypertensionComplement Ther ClinPract 2011 17:9-12. [Google Scholar]
[48]. Sieverdes JC, Mueller M, Gregoski MJ, Brunner–Jackson B, McQuade L, Matthews C, Effects of Hatha yoga on blood pressure, salivary α-amylase, and cortisol function among normotensive and prehypertensive youthJ Altern Complement Med 2014 20(4):241-50. [Google Scholar]
[49]. Tyagi A, Cohen M, Yoga and hypertension: a systematic reviewAltern Ther Health Med 2014 20(2):32-59. [Google Scholar]
[50]. Green DJ, Maiorana A, O’Driscoll G, Taylor R, Effect of exercise training on endothelium-derived nitric oxide function in humansJ Physiol 2004 561(Pt 1):1-25. [Google Scholar]
[51]. Frisoli TM, Schmiender RE, Grodzicki T, Messerli FH, Beyond salt: lifestyle modifications and blood pressureEur Heart J 2011 32(24):3081-87. [Google Scholar]
[52]. Bijlani RL, Vempati RP, Yadav RK, Ray RB, Gupta V, Sharma R, A brief but comprehensive lifestyle education program based on yoga reduces risk factors for cardiovascular disease and diabetes mellitusJ Altern Complement Med 2005 11(2):267-74. [Google Scholar]
[53]. Paeolatti V, Loricchio DP, Basili S, Cavina G, Labaddia G, Pacelli M, Lifestyle and global cardiovascular risk: a prospective study on a borderline hypertensive populationClin Ter 2010 161(1):13-23. [Google Scholar]
[54]. Agte VV, Jahagirdar Tarwadi KV, The effects of Sudarshan Kriya Yoga on some physiological and biochemical parameters in mild hypertensive patientsIndian J Physiol Pharmacol 2011 55(2):183-87. [Google Scholar]
[55]. Tumova E, Sun W, Jones PH, Vrablik M, Ballantyne CM, Hoogeveen RC, The impact of rapid weight loss on oxidative stress markers and the expression of the metabolic syndrome in obese individualsJournal of Obesity 2013 2013:72951510 pgs [Google Scholar]