Treatment of an Adult with Skeletal Class III and A Hemimandibular Elongation A Multidisciplinary Approach
Eshan Awasthi1, Nitin Bhola2, Ranjeet Kamble3, Sunita Shrivastav4, Abhilasha Goyal5
1 Senior Lecturer, Department of Orthodontics, Sharad Pawar Dental College, Wardha, Maharashtra, India.
2 Associate Professor, Depatment of Oral Surgery, Sharad Pawar Dental College, Wardha, Maharashtra, India.
3 Professor, Department of Orthodontics, Sharad Pawar Dental College, Wardha, Maharashtra, India.
4 Professor and Head, Department of Orthodontics, Sharad Pawar Dental College, Wardha, Maharashtra, India.
5 Senior Lecturer, Department of Orthodontics, Sharad Pawar Dental College, Wardha, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Eshan Awasthi, Mukut Nagar, Raigarh, Chhattisgarh-496001, India.
E-mail: eshaan.awasthi33@gmail.com
Bilateral saggital split osteotomy, Decompensation, Facial asymmetry, Hemimandibular elongation
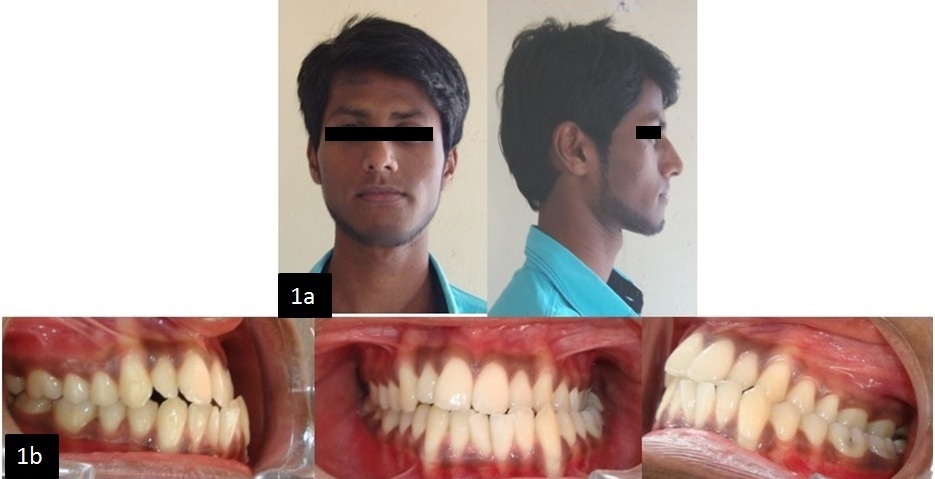
An adult male patient aged 21-year-old reported with the chief complaint of forwardly placed chin and deviation of chin towards the left side. The patient had an asymmetric face (shifted to left) with leptosoprosopic face form. On profile examination patient had a mild concave profile. The facial midline was not coincident with dental midline as chin was deviated towards left [Table/Fig-1]. Class III molar and canine relationship on right side and Class I molar, canine relation on left side was seen. There was an edge to edge overbite and overjet [Table/Fig-1].
(a) Pre treatment extra oral photograph. (b) Pre treatment intra oral photograph.
Diagnosis: Skeletal Class III malocclusion with vertical growth pattern. Angle’s Class III, sub division on left side.
Treatment plan: A comprehensive treatment plan involving pre-surgical orthodontics followed by Bilateral Saggital Split Osteotomy (BSSO) to perform asymmetrical setback with more orientation to the right side in order to correct the shift of lower jaw midline.
Pre-surgical orthodontics: An MBT 0.022" x 0.028" prescription was bonded to both upper and lower arch. Lower single tooth (lower right incisor) extraction for resolving lower anterior crowding along with upper arch expansion was done as the upper arch was constricted. The upper and lower arches were aligned, leveled and were stabilized with 0.021" x 0.025" in stainless steel wire presurgically [Table/Fig-2].
Pre surgical photographs.

Cephalometric prediction and mock surgery: Cast prediction or model surgery and fabrication of occlusal splints for use at surgery were planned. The lower dental cast was repositioned simulating the movement of the jaws for which the guide was manual prediction. [Table/Fig-3a,3b].
(a) Mock surgery. (b) Splint preparation. (c) BSSO surgery. (d) Rigid fixation using mini plates.
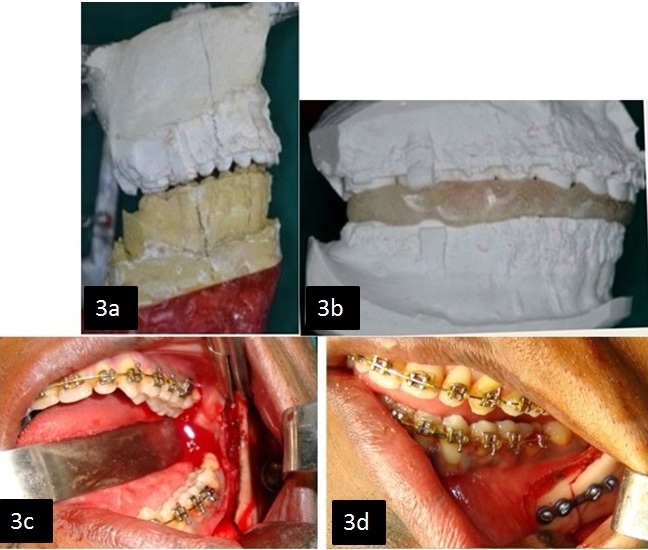
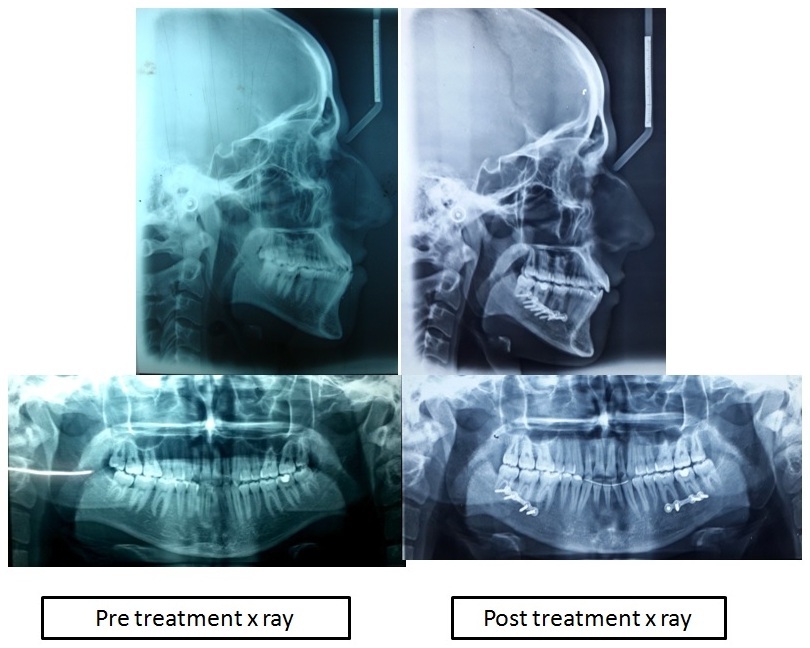
Surgical procedure: BSSO was performed successfully, with 6mm of mandibular setback on right and 2mm on left side for correction of the mandibular shift, thereby improving facial and dental symmetry [Table/Fig-3c]. Rigid type fixations were used in both jaws using four-hole manipulates and screw on both sides [Table/Fig-3d].
Post-surgical orthodontics: Post-surgical orthodontic phase was done four weeks after surgery for achieving optimum teeth intercuspation with the opposing dentition by segmental settling inter-maxillary elastics.
Results: The profile of the patient improved, facial asymmetry was resolved [Table/Fig-4,5 and 6], Class I molar and canine relationship with optimum overjet and overbite was achieved.
(b) Post treatment extra oral photograph. (b) Post treatment intra oral photograph.

| Variables | Pre treatment | Pre surgical | Current |
|---|
| SNA | 79° | 79° | 79° |
| SNB | 78° | 78° | 76° |
| SND | 76° | 76° | 74° |
| Effective mandibular length | 123mm | 123mm | 121mm |
| Go-Pog | 81mm | 81mm | 79mm |
| ANB | 1° | 1 | 3° |
| Go-Gn to SN | 37° | 38° | 37° |
| FMA | 30° | 31° | 30° |
| U1 to SN | 110° | 108° | 108° |
| 1 to NA(angular) | 30° | 26° | 26° |
| 1 to NA(mm) | 6mm | 5mm | 5mm |
| IMPA | 106° | 98° | 96° |
| 1 to NB(angular) | 38° | 33° | 31° |
| 1 to NB(mm) | 8mm | 6mm | 5mm |
| E line (-4/-2)mm | -7/-2mm | -6/-2mm | -6/-3mm |
Discussion
Class III malocclusion is one of the most difficult orthodontic condition to be treated [1]. Achieving objectives and treatment outcome of planned surgical orthodontic therapy requires multidisciplinary team approach [2]. The components involved are maxillary retrognathism, mandibular prognathism or combination of both. Class III asymmetry with mandibular component involved may be due to hemi-mandibular elongation (horizontal enlargement) or hemi-mandibular hyperplasia (vertical elongation) [3].
In the present case lower right incisor was extracted for alignment of lower arch. Matsumoto et al., stated extracting lower incisor tooth extraction as a viable treatment option in cases with malocclusions that tend towards a Class III malocclusion [4].
In this case manual predictions were employed at the end of pre-surgical phase. Post-surgical orthodontics was done in this case primarily for finalization of the occlusion and retention. The duration of the final orthodontic phase depends on the degree of intercuspation in pre-surgical phase of treatment. In order to attain long term stability for the results achieved in complex malocclusion such as Class III, the final occlusion achieved (intercuspation) post surgically and the occlusal stability acts as a retention factor i.e., a good dental retention will have a long term effect on stability of the results achieved.
[1]. Liu Z, McGrath C, Hagg U, The impact of malocclusion orthodontic treatment need on the quality of life a systematic reviewAngle Orthod 2009 79(3):585-91. [Google Scholar]
[2]. Jakobsone G, Stenvik A, Espeland L, Soft tissue response after class III bimaxillary surgeryAngle Orthod 2013 83(3):533-39. [Google Scholar]
[3]. Kawakami M, Yamamoto K, Inoue T, Kajihara A, Fujimoto M, Kirita T, Disk position and temporomandibular joint structure associated with mandibular setback inmandibular asymmetry patientsAngle Orthod 2009 79(3):521-27. [Google Scholar]
[4]. Matsumo to MA, Romano FL, Ferreira JT, Tanaka S, Morizono EN, Lower incisor extraction: An orthodontic treatment optionDental Press J Orthod 2010 15(6):143-61. [Google Scholar]