Hemostasis and Post-operative Care of Oral Surgical Wounds by Hemcon Dental Dressing in Patients on Oral Anticoagulant Therapy: A Split Mouth Randomized Controlled Clinical Trial
K.R. Ashok Kumar1, Jambukeshwar Kumar2, Jagadesh Sarvagna3, Praveen Gadde4, Shwetha Chikkaboriah5
1 Head of the Department, Department of Oral and Maxillofacial Surgery, Sri Siddhartha Dental College, Tumkur, Karnataka, India.
2 Senior Lecturer, Department of Oral and Maxillofacial Surgery, Vishnu Dental Collage, Bhimavaram, Andhra Pradesh, India.
3 Consultant Oral Oncologist, Siddhagiri Hospital, Kolhapur, Maharashtra, India.
4 Senior Lecturer, Department of Public Health Dentistry, Vishnu Dental College, Bhimavaram, Andhrapradesh, India.
5 Postgraduate, Department of Periodontics, Vakkaligara Sanga Dental College, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jambukeshwar kumar, Senior Lecturer, Department of Oral and Maxillofacial Surgery, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India.
E-mail: Jambukeshwarkumar@gmail.com
Introduction
Hemostasis is a fundamental management issue post-operatively in minor oral surgical procedures. To ensure safety and therapeutic efficacy in patients, under oral anti coagulant therapy, is complicated by necessity for frequent determination of prothrombin time or international normalised ratio.
Aim
The aim of the study was to determine whether early hemostasis achieved by using Hemcon Dental Dressing (HDD) will affect post-operative care and surgical healing outcome in minor oral surgical procedures.
Materials and Methods
A total of 30 patients, aged 18 years to 90 years, except those allergic to seafood, who consented to participate, were enrolled into this study. Patients were required to have two or more surgical sites so that they would have both surgical and control sites. All patients taking Oral Anticoagulation Therapy (OAT) were included for treatment in the study without altering the anticoagulant regimens. Institutional Review Board approval was obtained for the same. The collected data was subjected to statistical analysis using unpaired t-test.
Results
All HDD surgically treated sites achieved hemostasis in 1.49 minutes and control wounds in 4.06 minutes (p < 0.001). Post-operative pain at HDD treated sites (1.87,1.27 on 1st and 3rd day respectively) was significantly lower than the control sites (4.0,1.87 on 1st and 3rd day respectively) p-value (0.001, 0.001 respectively). HDD treated oral surgery wounds achieved statistically significant improved healing both at 1st and 3rd post-operative days (p <0.0001).
Conclusion
The HDD has been proven to be a clinically effective hemostatic dressing material that significantly shortens bleeding time following minor oral surgical procedures under local anaesthesia, including those patients taking OAT. Patients receiving the HDD had improved surgical wound healing as compared to controls.
Bleeding, Chitosan dressing, Extraction wound healing, International normalised ratio, Minor oral surgery
Introduction
Post-operative hemostasis in oral and maxillofacial surgery is a fundamental patient management issue [1,2]. Prolonged intra-operative and post-operative bleeding is alarming for the surgeons who treat patients taking anticoagulant medication [1,3]. Effective hemostasis in such situations is very critical. Surgeons either will have a choice of altering/stopping the anticoagulant therapy or continuing the same, but the former carries the risk of thromboembolism while the later has the risk of uncontrolled bleeding [4–9].
Although, others have shown that patients under well-controlled oral anti coagulant therapy (OAT) can safely undergo surgery, the patients’ International Normalized Ratio (INR) can and does vary between laboratory tests and appointments. Surgical patients who have undiagnosed elevated INR will have more post-operative bleeding. Uncontrolled bleeding and subsequent shock are the main causes for the combat related deaths [1,6]. Oral surgeons are sometimes the first to notice clinical signs and symptoms of undiagnosed genetic bleeding disorders [1,7]. Delayed hemostasis of oral surgical wounds may result in increased swelling, pain, delayed post-operative healing, alveolar osteitis, etc. The use of OAT is associated with the necessity for the frequent determination of the Prothrombin Time (PT) or INR to ensure safety and therapeutic efficacy [10]. The other side of research showed that continuing anticoagulant/anti-platelet therapy while doing minor oral surgery will not result in life threatening bleeding complications [4–7,10–15]. To limit post-surgery complications, several protocols have been proposed till date namely pressure packs, conventional suturing techniques, local anti-fribrinolytic therapy, local hemostatic agents, use of local tranexamic acid, human fibrin blue, platelet rich plasma, quick clot powder and fibrin sealant dressing [11,16]. Newly available Hemcon Dental Dressing (HDD) (Hemcon Medical Technologies, Inc.; 10575 Sw Cascade Ave, Suite 130; Portland Or 97223 U.S.A) is a naturally occurring biocompatible polysaccharide derived from exoskeleton of shrimp which usually dissolves within 48 hrs leaving site free of foreign material to allow natural wound healing. It is also very effective in achieving hemostasis without altering the patient’s anti coagulant regimen. [1,12] but there is a dearth of literature to support the effectiveness of HDD in preventing post-operative bleeding in patients with anticoagulant medication. Against this background, we planned a study with the aim to evaluate the efficacy of HDD as a hemostatic agent. The objective of the present study was to determine whether early hemostasis affects post-operative care and surgical healing outcomes following oral surgical procedures.
Materials and Methods
A split mouth randomized controlled trial was conducted in Department of Oral and Maxillofacial Surgery, Sri Siddhartha Dental College and Hospital, Tumkur, Karnataka, India, among 30 patients (sample size was determined from the findings of a pilot study with 80% power and 95% confidence levels 5 patients were involved in pilot study and were included in the study) aged 18 years to 90 years who required minor oral surgical procedures and were having two or more surgical sites [Table/Fig-1]. All consented patients taking OAT with INR less than 4 were included without altering their anticoagulant regimens. The study was registered under the Clinical Trial Research Institute of India with a registration number CTRI/2016/08/007174. Patients allergic to sea food and with severe medical illness, who were not fit for surgery, were excluded from the study [1]. Ethical clearance was taken from the Institutional Review Board before the start of the study. Two extraction sites, one each in separate quadrant or in same quadrant were randomly allocated into study and control sites [Table/Fig-1]. To reduce the study variability two contralateral sites or tissue in two different sites of any pathology were selected wherever possible. Neither patient nor surgeon could be blinded to the use of HDD versus control method. Patients were randomly divided into two groups by coin toss method.

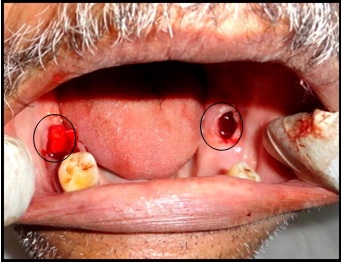
1) Study site: Hemcon dental dressing was applied under finger pressure [Table/Fig-2].
2) Control site: The conventional method of pressure pack with a sterile gauze piece under biting pressure was used.
Under unavoidable circumstances if the hemostasis was not achieved at the control site after normal clotting time, then HDD was used to stop the bleeding. After recording complete history, patients were explained about the surgical procedure. Pre-operatively, bilateral Intra-Oral Periapical Radiograph (IOPAR), OPG, all necessary blood investigations were done. Surgical procedures were performed in single appointment; if possible the same tooth in the opposing quadrant or contralateral or same quadrant will be used as control to further minimize the study variability. Three patients were dropped out as they did not come back for the follow-up.
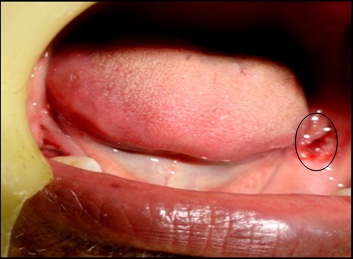
Procedure: HDD shown in [Table/Fig-3], with desired dimension 10mm×12mm was trimmed to fit any bleeding oral wound. Small amount of blood was intentionally left on surface as it was required to facilitate the unique adhesion process. Dressing was placed on the wound site with the dry instrument without packing the site. Direct finger pressure or dry instrument was applied on the dressing until it adheres and wound stabilization was achieved. Finger pressure or instrument was removed by lateral sweeping method to avoid dislodging of material. The top of the dressing should be at the level of crestal gingiva. Duration to achieve hemostasis was noted for HDD site and control site. If the surgical site was larger, then suture was used to stabilize the material if necessary. On the control site sterile cotton gauze dressing placed with biting pressure and time taken for hemostasis was noted. HDD sites were inspected to confirm correct positioning of the dressing on 1st, 3rd and 7th post-operative days [Table/Fig-4,5]. If the material had not dissolved within 48 hours it was washed with irrigation. Post-operative photographs were taken on the 3rd and 7th day from the treatment. At one week post-operative appointment healing was evaluated using a scale as follows: 1(significantly worse than control), 2 (same as control), 3 (significantly better than control). Self reported pain scores were evaluated using Visual Analogue Scale (VAS) of 0 to 10 with 0 being no pain and 10 being the worst pain. Standardized Alveolar Osteitis Assessment Criteria [1,4] was used which included radiating pain, clot loss, dark coloration and fetid odour. All the patients were instructed about the oral hygiene maintenance and post-operative medications were prescribed. Patients were counselled for follow-up visits and then clinical evaluation of various parameters was done.
Hemcon Dental Dressing (HDD).

Statistical Analysis
Descriptive statistics were done and the data collected were subjected to statistical analysis using IBM SPSS (IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp). Unpaired t-test was used to compare means between the groups. A p-value <0.05 was considered statistically significant for all the comparisons.
Results
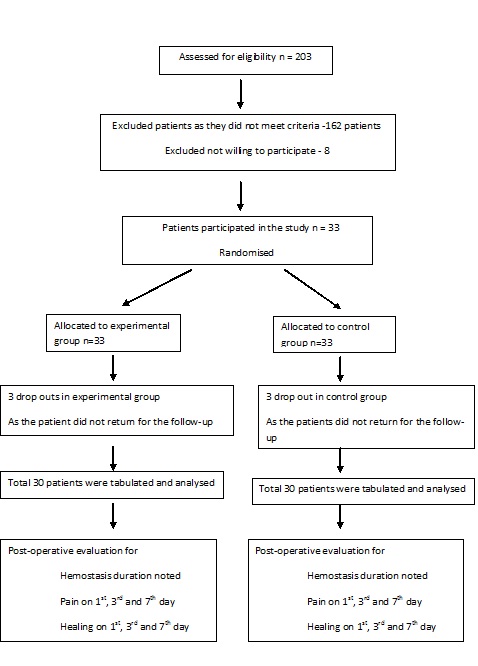
Total 203 patients were assessed for eligibility and 162 patients were excluded as they did not meet the criteria and eight patients were excluded as they were not willing to participate in study and total 33 patients took part in study [Table/Fig-6].
Flowchart for allocation of subjects.
[Table/Fig-7] shows the distribution of study population according to age and gender. Majority of the study population were females with 40% of them were in the age range of 30-50 years.
Distribution of study population according to age and gender same region.
| Characteristics | | Number | Percentage |
|---|
| Age(Years) | < 30 | 3 | 10% |
| 30-50 | 12 | 40% |
| 50-70 | 10 | 33.3% |
| >70 | 5 | 16.6% |
| Total | 30 | 100% |
| Gender | Male | 12 | 40% |
| Female | 18 | 60% |
| Total | 30 | 100% |
Hemostasis: The time to achieve hemostasis was shorter using HDD than using pressure pack. The mean time to achieve hemostasis for control site was 4.06 minutes. Statistical significance was found in respect to hemostasis in HDD sites [Table/Fig-8].
Comparison of mean hemostasis and pain scores between HDD and control sites.
| Characteristics | Group | Mean | Standard Deviation | t-value | p-value |
|---|
| Duration of achievement of hemostats | Study | 1.49 | 0.39 | 7.914 | 0.001* |
| Control | 4.06 | 1.85 |
| Pain score on day 1 | Study | 1.87 | 0.57 | 10.016 | <0.001* |
| Control | 4.00 | 1.34 |
| Pain score on day 3 | Study | 1.27 | 0.69 | 3.525 | 0.001* |
| Control | 1.87 | 1.20 |
| Pain score on day 7 | Study | 0.37 | 0.49 | 1.439 | 0.160 |
| Control | 0.43 | 0.57 |
Unpaired t test, *Statistically significant
Pain scores: Relative pain scores were assessed at day 1, day 3 and on day 7 of post-operative appointments and were based on a 0 to 10 self-reported pain score basis, with 0 being no pain and 10 being the worst pain the patient had ever experienced. HDD relative pain scores were significantly lower than control at day 1 and day 3 but these findings were not statistically significant at day 7 [Table/Fig-8].
Healing: Using a scale of 1 (significantly worse than control), 2 (the same as control), and 3 (significantly better than control), 22 of 30 HDD study sites demonstrated significantly improved healing compared with controls at day 1 and showed complete healing at day 3. HDD study sites healed comparatively better than control sites. There was statistically significant improved healing in HDD study sites compared with control sites [Table/Fig-9].
Comparison of healing between Hemcon dental dressing (HDD) versus control sites.
| | Improved healing | Mean HDDImprovedHealing VersusControl | p-value |
|---|
| HDD | Control |
|---|
| At day 1 | Improved healing | 22 | 0 | 2.73 ± 0.449 | < 0.0001* |
| Same as control | 8 | 30 |
| At day 3 | Improved healing | 30 | 0 | 2.4 ± 0.498 | < 0.0001* |
| Same as control | 0 | 30 |
Unpaired t test, *Statistically significant
Discussion
The possibility of post-surgical hemorrhage is a concern in any patient who is undergoing minor surgical procedure such as extraction, excision of oral lesions, etc. This possibility increases even more in patients taking anti-coagulant or anti-platelet therapy. The new generation HDD of hemostatic medical devices can achieve early hemostasis and improve post-operative healing in patients undergoing minor oral surgical procedures [1]. In the past, stopping anticoagulant treatment for 2-6 days before dental extractions has been suggested since severe hemorrhage may occur post-operatively. Recent research had advocated the continuation of anticoagulant therapy in oral surgical procedure which had gained more attention in the literature, emphasizing the role of local hemostasis [4]. Ferraris and Swason suggested that aspirin need not be stopped before any surgery [17]. Lawrence et al., recommended the continuation of aspirin therapy before elective dermatologic surgery if bleeding time is within normal limits [18]. Inspired by the above studies supporting our view point, we decided to conduct our own which, study included all patients of age group 18-90years taking anti-platelet therapy as well as who required minor surgical procedures. Investigations of PT, INR, bleeding time and clotting time were performed pre-operatively in all the patients. In the present study, sites receiving the HDD had improved post-operative wound healing with minimal complications when compared to the control site. In all sites receiving HDD had showed improved hemostasis (mean 1.49) and reduced pain (mean 1.87 and 1.27) on 1st and 3rd days respectively, but on 7th day there was no significant difference in pain scores. The study also includes taking biopsy to the peripheral gaint cell granuloma in which two sites of the lesion was selected for biopsy out of which in one site HDD achieved hemostasis in 2 min10 sec, and in the other site even after 11 min 40 sec hemostasis was not achieved and later HDD material was used and achieved hemostasis in 2 min, which shows that HDD is a clinically effective haemostatic agent for arresting vessel bleed encountered during minor oral surgical procedures. The results of this study are similar to the study reported by Malliquist JP et al., which reaffirms the efficacy of HDD over conventional methods [1].
The use of antibiotics in conjunction with the HDD had no untoward effect on hemostasis, healing or pain scores. There was no incidence of dry socket, liver clot and untoward incidents in our study at the HDD site. The result of this study proved the fact that Hemcon is a new generation hemostatic agent with which facilitates early hemostasis, better pain control, along with improved wound healing and reduced post-operative pain. Chitin (poly-N acetylglucosamine) is a polysaccharide that is found in arthropod skeletons and produced by algae during fermentation. Both chitin and its deacetylated form chitosan have haemostatic properties. For chitin dressings, haemostatic properties are believed to result from vasoconstriction and mobilization of erythrocytes, clotting factors and platelets to the site of injury [1]. One of the most prominent chitin dressings is the Rapid Deployment Hemostat (RDH) made by marine polymer technologies. In animal studies, chitin is effective in treating minor wounds [2].
In one study, RDH applied to splenic lacerations in swine led to coagulation in 23 seconds, significantly faster than the 173 seconds with fibrin glue. In contrast other studies in swine indicated that RDH gave no statistically significant improvement in survival over a standard gauze dressing [2]. Chitosan dressing such as Hemcon appear to function through mechanically sealing wounds and adhering to surrounding tissue. Advantage of chitosan is natural antimicrobial property. Another advantage of chitosan is that its polycationic nature at acidic pH (like in Hemcon bandages which includes acetic acid) allows it to disrupt the membranes of gram-negative bacteria, giving it natural antimicrobial properties. It is worth noting that all the failures of Hemcon in that animal study were due to bandage not adhering to the tissue to which it was applied. Hemcon can effectively reduce blood loss when applied properly to a wound and has the added benefit of antimicrobial properties [2]. No side effects were reported in the present study and previous studies done. Further studies can be conducted with more number of subjects without keeping INR limitations. The present study material shows better hemostasis reduced pain, and good healing, in patients on AOT which can be used regularly.
Conclusion
The present study provides evidence that HDD can be used as a clinically effective haemostatic dressing material that significantly shortens bleeding time following minor oral surgical procedures. HDD also had better pain control, wound healing rates, improved surgical wound healing and reduced pain score compared to control sites. It also meets most of the criteria’s of ideal haemostatic agent. Furthermore, prospective clinical studies are required to study its efficacy in patients who are on OAT with higher INR values.
Unpaired t test, *Statistically significant
Unpaired t test, *Statistically significant
[1]. Jay MP, Stephen CC, Hal OJ, Sharon WL, Hemostasis of oral surgery wounds with the hemcon dental dressingsJ Oral Maxillofac Surg 2008 66:1177-83. [Google Scholar]
[2]. Harden AE, Banatayehu S, Rayan JM, Oavid AM, Shapiro M, Jeffrey LH, A comprehensive review of tropical hemostatic agents efficacy and recommendations for useAnn Surg 2010 251:217-28. [Google Scholar]
[3]. Cunningham L, Bernalt TM, Eron A, Perioperative treatment of patients taking anticoagulation medicationOral Maxillofacial Surg Clin N Am 2006 18:151-59. [Google Scholar]
[4]. Blinder D, Manor Y, Martinowitz U, Taicher S, Dental extractions in patients maintained on oral anticoagulant therapy: Comparison of INR value with occurrence of post-operative bleedingInt J Oral Maxillofac Surg 2001 30:618-21. [Google Scholar]
[5]. Ross BO, Evidence to continue oral anticoagulant therapy for ambulatory oral surgeryJ Maxillofac Surg 2005 63:540-45. [Google Scholar]
[6]. Aframian DJ, Lalla RV, Peterson DE, Management of dental patients taking common hemostasis altering medicationOral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 103:S45.e1-11. [Google Scholar]
[7]. Campbell JH, Alvarado F, Murray RA, Anticoagulation and minor oral surgery: Should the anticoagulation regimen be altered?J Oral Maxillofacial Surg 2000 58:131-35. [Google Scholar]
[8]. Devani P, Lavery KM, Howell CJ, Dental extractions in patients on warfarin: Is alteration of anticoagulant regime necessary?Br J Oral Maxillofac Surg 1998 36:107-11. [Google Scholar]
[9]. Beirne OR, Koehler JR, Surgical management of patients on warfarin sodiumJ Oral Maxillofacial Surg 1996 54:1115-18. [Google Scholar]
[10]. Sunil S, Jyotsna G, Contemporary management of patients on Warfirin, Aspirin, and Clipidogrel requiring dentoalveolar surgeryJ Contemp Dent 2011 1:22-25. [Google Scholar]
[11]. Madan GA, Madan SG, Madan G, Minor oral surgery without stopping daily low-dose aspirin therapy: A study of 51 patientsJ Oral Maxillofacial Surg 2005 63:1262-64. [Google Scholar]
[12]. Tejraj KP, Amit kumar S, Kotrashetti SM, Abhishek K, Effectiveness of hemcon dental dressing versus conventional method of hemostasis in 40 patients on oral antiplatlet drugsSultan Qaboos University Med J 2012 12:330-35. [Google Scholar]
[13]. Salam S, Yousuf H, Milosevic A, Bleeding after dental extractions in patients taking warfarinBrit J Oral Max Surg 2007 45:463-66. [Google Scholar]
[14]. Miracle P, Jose AM, Dental management of patients receiving anticoagulation or antiplatlet treatmentJ Oral Sci 2007 4:253-58. [Google Scholar]
[15]. Evans IL, Sayers MS, Gibbons AJ, Price G, Snooks H, Sugar AW, Can warfarin be continued during dental extraction? Results of a randomized controlled trialBrit J Oral Max Surg 2002 40:248-52. [Google Scholar]
[16]. Valle AD, Sammartino G, Prevention of post-operative bleeding in anticoagulated patients undergoing oral surgery: Use of platelet-rich plasma gelJ Oral Maxillofacial Surg 2003 61:1275-77. [Google Scholar]
[17]. Ferraris VA, Swanson E, Aspirin usage and perioperative blood loss in patients undergoing unexpected operationsSurg Gynecol Obstet 1983 156:439-42. [Google Scholar]
[18]. Lawrence C, Sakauntabhai A, Tiling Grosse S, Effect of aspirin and nonsteroidal anti inflammatory drug therapy on bleeding complications in dermatological surgical patientsJ Am Acad Dermatol 1994 31(6):988-92. [Google Scholar]