Cuspal quantification and morphologic variation has always been a topic of research since long time. These structural variations in tooth are the part of dental anthropological system and should be determined in different population or a race. Tooth morphology may be an indicator of genetic disturbances between populations [1]. Cusp plays an important role in identifying these patterns. The morphological abnormalities has certain clinical implications such as difficulty in band placement, plaque accumulation due to abnormal morphology of the fissures, caries due to presence of deep pits, occlusal disturbances due to abnormal location, difficulties in restorative, surgical and endodontic procedure.
Maxillary first molars are the largest of all the maxillary molars and play an important role in mastication. They also play an important morphometric role in gender differentiation. The anchorage value of first permanent maxillary molar is high that makes it an important tooth from orthodontic treatment point of view. Hence, it is important to know the variation in cusps and different forms of first permanent maxillary molar. Human first maxillary molar provides clue about evolution and is functionally important [2].
Each cusp has an individual growth pattern and different evolutionary background [3,4]. Many studies have reported that mesiodistal width and buccolingual width measured are higher in males than females and the difference is statistically significant [5]. Till date no study has been done to evaluate cuspal variation of first permanent maxillary molar on Malwa population of India.
The aim of this article was to quantify cuspal variation in permanent maxillary first molar and report the variations in its cuspal numbers in the Malwa population of India.
Materials and Methods
A study was conducted at Government College of Dentistry, Indore, Madhya Pradesh, India, to evaluate the number of cusps in permanent maxillary first molars. According to the previous studies [6] on prevalence of permanent maxillary first molar on different cusp the sample size was calculated which came out to be 646. As we had taken samples of both males and females separately we took a sample of approximately twice the number. Out of which, 638 were males and 611were females. The inclusion criteria were as follows:
1) Subjects who had parents and grandparents of Indian origin,
2) Absence of any systemic diseases,
3) No congenital abnormalities or medical problems,
4) Age between 12 -30 years,
5) No severe attrition or abrasion of the molars,
6) Not undergone any previous treatment in their permanent first molars,
7) First permanent maxillary molars bilaterally present.
The impressions were made in alginate for all the participants and immediately poured in dental stone to prevent distortion. The casts were analyzed visually by a single examiner and the data was recorded. The cases with any peculiar features were recalled and examined clinically again to confirm with the findings of the cast. The statistical analysis was performed with SPSS version 20 (SPSS, Armonk, NY, USA). The extent of the association between the number of cusps and gender was assessed using chi-square analysis. A p-value <0.05 was considered significant.
Results
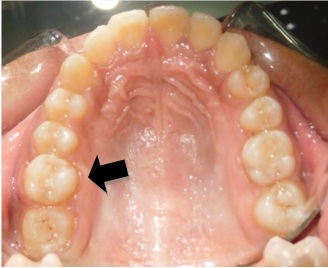
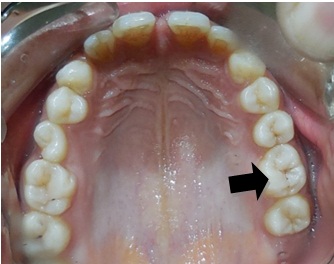
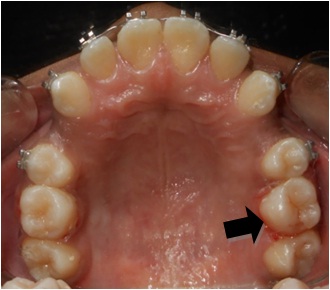
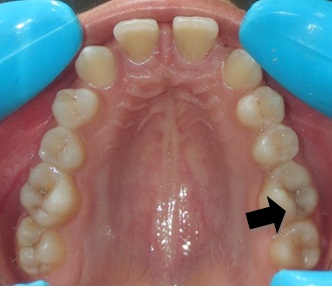
Of the total individuals studied, the permanent maxillary first molars had five cusps in 407 (32.6%) cases while, 838 (67.08%) had four cusps and four (0.32%) cases had three cusps in permanent maxillary first molar. The unique finding of the three cusped permanent maxillary first molar in four individuals was that they were present unilaterally in all the four cases. In one case it was present on the right side and in the remaining three cases it was present on the left side. Incidentally all the four cases were females. The results are illustrated in [Table/Fig-1]. [Table/Fig-2,3,4 and 5] represents the intra-oral photographs of the four cases and [Table/Fig-6] shows the cast with three cusp maxillary first molar present unilaterally on left side. Frequency of occurrence of three cusped and four cusped molars was more in females as compared to males; however the five cusped molars were seen more frequently with males as compared to females [Table/Fig-1].
Association between the number of cusps and gender.
| Number of cusps /Gender | 3 cusp | 4 cusp | 5 cusp | χ2(p-value) |
|---|
| Male | 0 | 411 | 227 | 9.1536 (0.010288) |
| Female | 4 | 427 | 180 |
| Total | 4 | 838 | 407 |
*p value < 0.05
CASE 1 – A 20 year old female with three cusped molar (16).
CASE 2 – A 24 year old female with three cusped molar (26).
CASE 3 – A 19 year old female with three cusped molar (26).
CASE 4 – A 22 year old female with three cusped molar (26).
Cast showing three cusped maxillary first molar unilaterally on left side.

Discussion
Just as the permanent canines are considered to be the cornerstones of each arch in position, form and function, the permanent first molars are thought of as cornerstones in the development of occlusion. This is due to their early eruption date, and location in the arch, compared to the other teeth of both dentitions [7]. Morphology of tooth depends on genes and race. Morphologic pattern of tooth is established by morpho-differentiation. Dentino-enamel and dentino-cemental junctions act as blue print for characteristics of each type of tooth. Vitamin A deficiency and endocrine disturbances like hypopituitarism and hypothyroidism lead to short clinical crown and abnormal root curvature (Dilaceration) [8].
John YK et al., reported sexual dimorphism that males generally showed a lesser tendency than females to reduction in the number of cusps of the upper molars [9]. Moreover females tend to have more cusps for the same crown diameter. Larger teeth of the same class had a greater number of cusps. This finding is in contrast to the finding of present study. John YK et al., in their study on Southern Chinese population found that in upper first molars, five cusp molars were most prevalent in males (39%) while four cusp molars were most prevalent in females (39%) [9]. They also found six, seven and eight cusped upper molars while we did not find cusps more than five in Malwa population.
The maxillary first molar is the largest tooth in the maxillary arch, and in fact, has the largest crown in the mouth. Of all the maxillary molars, the first molar is the least variable in anatomic form, and is thus the standard to which the other maxillary molars are compared. There are four major cusps and one minor, sometimes indistinct cusp, which is the cusp of Carabelli. This cusp of Carebelli was absent on 35.4% of teeth in 489 Hindu children [6]. Woelfel in a study on 1558 maxillary first molars of his students found that 70.5% had some type of Carabelli formation [10].
Mesiobuccal cusp - It is quite sharp, and the second largest in size.
Distobuccal cusp - It is the sharpest and third largest of the four major cusps.
Mesiolingual cusp - It is the largest cusp, but its tip is rounded and blunt.
Distolingual cusp- It is the smallest cusp present.
This article presents with four cases in which three cusped permanent maxillary first molar have been observed. All of these patients reported to the Department of Orthodontics and Dentofacial Orthopedics, Government College of Dentistry, Indore, Madhya Pradesh, India, with a certain esthetic concern requiring orthodontic intervention. All the four individuals were females. The patients were healthy with no significant pathological finding. Complete past medical and dental history along with the nutritional status was noted. No nutritional deficiencies were found and no syndromes were diagnosed in the subjects. On careful examination the permanent maxillary first molar revealed distinct three cusps on the occlusal surface instead of four or five cusps usually seen. The finding was unilateral in all the observed cases. The mesiobuccal and distobuccal cusps were present but the palatal surface had only a large single cusp. The oblique ridge, which is an arch trait of maxillary molars, the distolingual cusp and the cusp of Carabelli were missing in all the cases. The cusp ridges do not join to form the transverse ridge. It can be appropriate to say that these molars resemble the three cusp mandibular second premolars but somewhat larger in size as compared to them. These three cusp maxillary first molars had a heart shaped outline. The palatal cusp nearly lies in the center of the mesiobuccal and distobuccal cusp thereby giving it a heart shape.
Since the present molars were showing minimum number of cusps as compared to the usually found four or five cusps and incidentally the first case reported was in the individual named ‘Mini’ it has been named ‘MINI MOLARS’ by the author. All the cases were present unilaterally and in females.
Dahlberg compared four cusp molars with five cusp molars in the lower arch and found a change only in the mesiodistal dimension, the buccolingual dimension was almost same in both cases [11].
It is believed that the possible etiology of cuspal variation could be either nutritional or genetic. PAX, MSX1, MSX 2 BMP, FGF 4 and Shh (Sonic Hedgehog) genes are responsible for the abnormal shape of the teeth [12].
Clinical Significance
In clinical dentistry the diagnosis of this cuspal variation is important as they may be associated with other anomalies and syndromes. We as dentist should be observant regarding such morphological variations noticed during routine dental examination.
Maxillary first permanent molar is an important tooth in the dentition. It is used for banding in case of fixed orthodontic treatment and its morphology is also important in cases where lingual orthodontic treatment has been planned, also the number of root canals present is important in cases of root canal treatments and proper cavity preparation and restoration.
The cuspal variation if associated with the root number and morphology can affect the clinical outcome during endodontic treatment, periodontal management, extraction, tooth preparation for restorative treatment, as well as orthodontic treatment of such teeth [13,14]. Moreover, the presence of a single large palatal cusp should be observed for its occlusal interferences/premature contact and altered function of equilibrium.
Difference in the morphological shape or size of molars can also lead to difficulty in placement of bands and buccal tubes in both labial and lingual orthodontics.
From an anthropological point of view, the significance of the study of these cusps is that their frequencies differ from population to population. Proper documentation of these variations may help anthropologists in their study of a population [15].
Conclusion
Three cusped permanent maxillary first molars do exist. They should be carefully recorded and reported in the literature. All the four cases of three cusped permanent maxillary first molars were observed in females. This might indicate a female preponderance of such event. All the four cases of three cusped permanent maxillary first molars were present unilaterally. This might indicate a site specific alteration in the morphologic behavior of the developing molar. The large single palatal cusp should be taken into consideration during clinical management.
Further studies may be undertaken in patients having three cusps on the permanent maxillary first molar to evaluate the number and size of roots, canal morphology etc., using IOPAs and/or CBCT.
*p value < 0.05