Urinary incontinence is a condition causing significant psychological trauma and affects the quality of life of the affected individual. Though common causes of urinary incontinence of non-traumatic aetiology in young adults include detrusor instability and congenital conditions like meningomyelocoele, an ectopic ureter is an important surgically correctable cause of urinary incontinence. The cause of incontinence in an ectopic ureter is insertion of the ureter distal to the internal urethral sphincter. The authors describe a case report of an ectopic ureter arising from a duplex moiety with poor renal function using multiple modalities. This highlights the utility of multiple modalities in arriving at an accurate diagnosis, with adequate clinically useful information. In this case, the formation of a pseudo-diverticulum resulted in diagnostic confusion.
Case Report
A 23-year-old unmarried, Indian lady, presented with a history of intermittent urinary incontinence since childhood, which reduced over her period of adolescence, with mild intermittent incontinence persisting into adulthood. She also gave history of repeated urinary tract infections. The patient had not disclosed the occurrence of incontinence previously because of the fear of social stigma.
On clinical examination the external genitalia was normal. The abdominal examination was normal with no suprapubic tenderness.
On laboratory investigation, the patient had albuminuria and asymptomatic bacteruria, growing >100000 colonies/ml of E.coli. The patient was then referred for ultrasound.
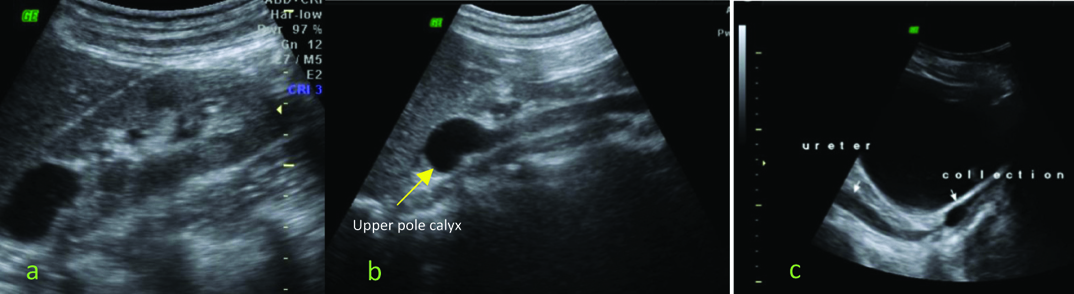
Initial evaluation with ultrasound of the pelvis showed the presence of a duplicated collecting system with dilated right upper pole calyces surrounded by no discernible renal parenchyma, draining into a separate dilated ureter. The ureter was seen to terminate in a fluid collection posterior to the urinary bladder [Table/Fig-1]. This was suspected to be collection of urine in the vagina and a possibility of an ureterovaginal fistula was considered.
Ultrasonography (USG) with: a) Right kidney showing dilated upper pole calyx with thinned out parenchyma; b,c) Upper pole duplex moiety with the ectopically inserting ureter which is noted to terminate in a fluid collection posterior to the urinary bladder in the region of vagina.
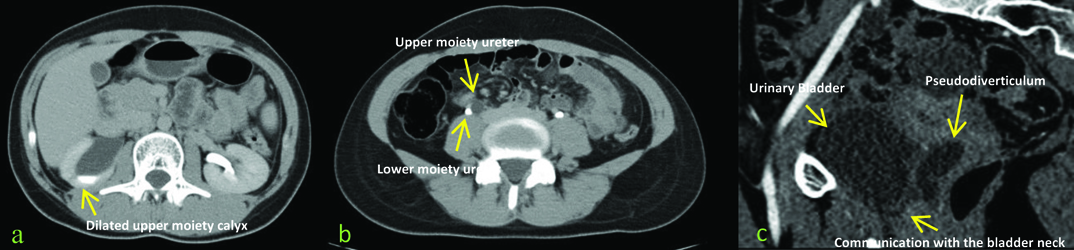
Computed Tomography (CT) Urogram confirmed the finding of dilated right upper pole calyces with no discernible surrounding parenchyma draining into a separate dilated ureter. The ureter was noted to terminate in an irregular fluid-filled sac posterior to the bladder. A communication of this irregular fluid-filled sac with the bladder neck was noted. Minimal excretion of contrast was noted into the upper pole calyx in the CT urogram on delayed images [Table/Fig-2]. These findings suggested a double right collecting system with the ureter of the dilated upper moiety terminating in a pseudodiverticulum, with suspicious communication of the pseudodiverticulum with the bladder neck.
Contrast Enhanced Computed Tomography (CECT) with: a) Right kidney showing dilated upper pole calyx with minimal contrast opacification; b) Double ureters with no contrast opacification in the ectopic ureter of the upper moeity; c) This ectopic ureter was noted to drain into a pseudodivertivulum with a communication with the bladder neck.
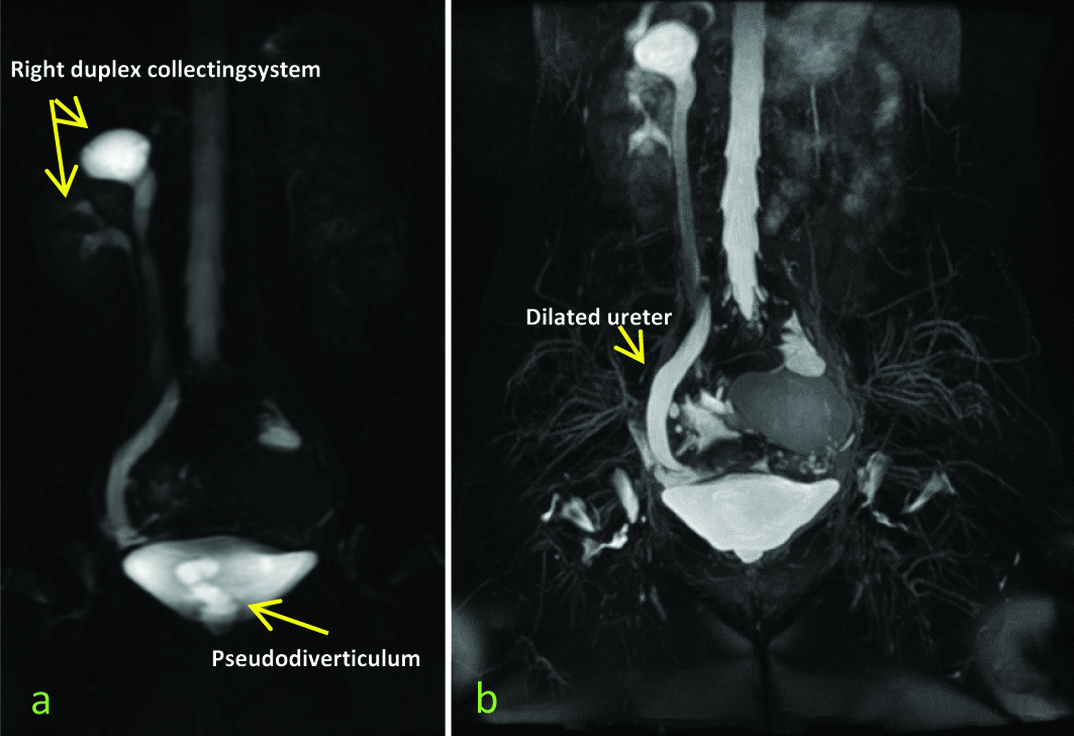
Static Magnetic Resonance (MR) Urogram confirmed the finding of dilated calyces of the upper moeity, with no discernible surrounding parenchyma draining into a separate dilated ureter. The ureter was noted to terminate in an irregular fluid-filled sac posterior to the bladder, with the ectopic ureteric communication not well visualized [Table/Fig-3].
MR Urogram images demonstrating the duplex collecting system with the ectopic ureter draining into a pseudodiverticulum posterior to the bladder.
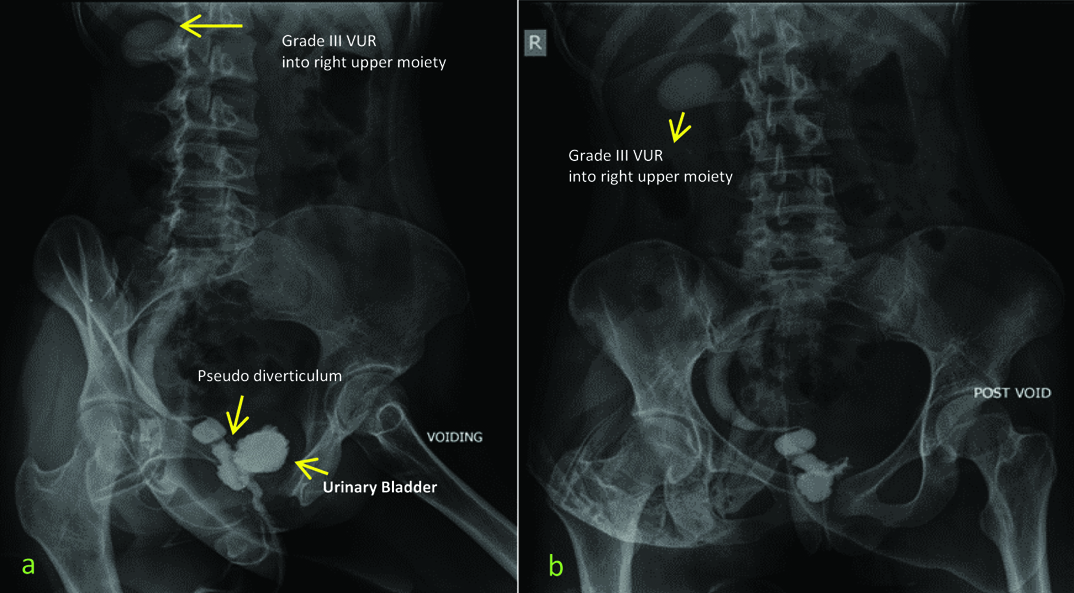
A micturating cystourethrogram (MCUG) was then performed. The study revealed a small capacity bladder with grade III vesicoureteric reflux of the right ectopic ureter with insertion at the bladder neck [Table/Fig-4].
a,b) Micturating cystourethrogram (voiding and post void films) shows a small capacity bladder with Grade III vesicourteric reflux into the upper pole of the right kidney, corresponding to the upper duplex moeity. A smooth tapering of the ureter is noted, beyond which an irregular dilation corresponding to the pseudo-diverticulum is seen, which communicates with the bladder neck.
Thus a diagnosis of refluxing ectopic ureter with pseudo-diverti-culum inserting into bladder neck was made.
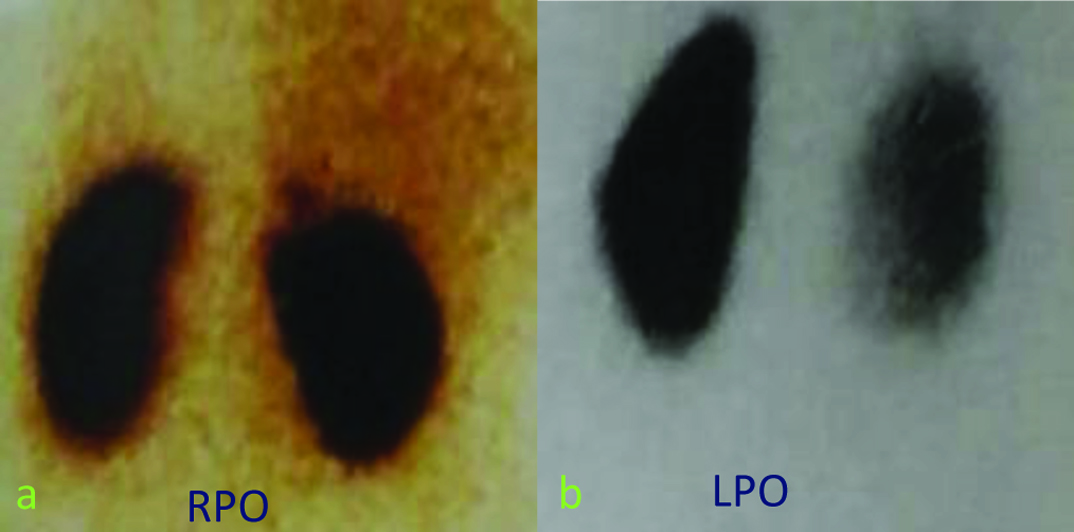
Dimercaptosuccinic Acid (DMSA) showed a poorly functioning right upper moiety [Table/Fig-5]. Differential renal function of the poorly-functioning upper moeity was 3.14%.
a,b) DMSA scan done using 90 MBq of 99m TcDMSA showing faint tracer uptake in the right upper pole corresponding to the poorly functioning right upper moeity, with homogenous tracer uptake in the right lower pole.
The patient underwent partial-nephrectomy and the primary diagnosis was confirmed, with postoperative resolution of patient’s symptoms. This case-report illustrates utility of multiple modalities in differential diagnosis. The mistaking of the pseudo-diverticulum for the fluid-filled vagina on ultrasound led to the diagnostic dilemma, which was resolved by micturition cystourethrography and cross-sectional imaging.
Discussion
Urinary incontinence is a condition that impairs the quality of a person’s life, including partner relationship, with significant psychological morbidity [1]. The common causes of non-traumatic urinary incontinence in nulliparous women without pelvic organ prolapse are pure detrusor instability and congenital conditions like myelomeningocoele [2,3]. The authors discuss a surgically correctable cause of urinary incontinence, in a duplicated ureteric system containing an ectopic ureter with reflux. The true incidence of ectopic ureter is not exactly known, but the female to male ratio is believed to be 6:1. In this case report we highlighted the role of multiple imaging modalities in arriving at a diagnosis. Patients having ureteric reflux and ectopic ureters are prone to develop recurrent urinary tract infections [4]. Thus, it is necessary to identify and treat this condition at an early stage.
Early in gestation, at about 4-6 weeks the distal mesonephric duct is absorbed into the urogenital sinus. This results in separation of the ureteral bud and the mesonephric duct orifices. The ureteral orifices migrate to a lateral and cranial position, while the mesonephric duct migrates downward and medially. If the ureteral bud has had a cranial origin it may migrate downward and medially along with the mesonephric duct resulting in its opening along the course of the mesonephric duct. If this opening occurs distal to the internal urethral sphincter continuous incontinence results [5].
Weigert-Meyer rule, which is applicable to a completely duplicated collecting system states that the ureter arising from the lower pole of the kidney inserts more superiorly and laterally into the bladder, resulting in a short intramural course that predisposes the ureter to reflux. The ureter arising from the upper pole moeity, which inserts more inferiorly and medially, frequently forms a ureterocoele and gets obstructed [4,6].
It is important to identify the site of ectopic ureteral insertion to aid pre-operative surgical planning. Further non-identification of ectopic ureteral insertion may result in delay in diagnosis with persisting urinary incontinence despite therapy [7].
Further, in case a partial nephrectomy is planned, it is important to know whether the ectopic ureter shows reflux. In case of duplex ureter, with an ectopic inserting beyond the internal urethral sphincter, it is difficult to dissect the ureter distally. Hence, if there is no reflux the ureteric stump can be left open, else, a suture will have to be safely placed to occlude the ureteric lumen during surgery.
It is also important to know whether the native ureter shows reflux. In salvageable or functional ectopic moieties with the absence of ureteric reflux a ureteropyelostomy is performed. However, in the presence of ureteric reflux usually a (distal) common sheath ureteric reimplantation is performed [5].
This case was also unique because of the presence of a large distal ureteral pseudodiverticulum. Duplex moeities may be associated with bladder neck diverticula, but they are usually transient and disappear with age [8]. However, in this case we call the lesion a pseudo-diverticulum of the distal ureter because the Magnetic Resonance Imaging (MRI) as well as the MCU [Table/Fig-3,4] shows a distal ureteric narrowing continuous with an irregular fluid-filled sac posterior to the bladder. Further, the CT Urogram image shows a narrow distal communication from the irregular sac which continues to insert into the bladder neck. In a case report of an ectopic ureter in a duplicated collecting system, masquerading as a urethral diverticulum, Curry NS reported a 54-year-old woman with recurrent urinary tract infections who denied history of incontinence. This patient had a duplicated collecting system, with an apparent urethral diverticulum and renal parenchymal atrophy. A MCU demonstrated the diverticulum which was confirmed by urethroscopy. When the diverticulum was opened and contrast was injected through it, it was found to be continuous with a markedly dilated ectatic distal ureter. Curry NS stated that despite several reports of ectopic duplicated ureters draining into diverticula, it was likely that they were partially filled dilated distal ureters [9] This view is strongly supported by our case report. Further, she stresses that a constriction of the ectopic ureter may be present as it passes anterior to the vagina which may prevent reflux during voiding [9]. This finding was also observed in our patient, and supported both intraoperatively and by cystoscopy.
In a case report by Michelotti B et al., the authors desribe a case of a bladder diverticulum arising from the lateral wall of the bladder adjacent to an ectopic ureter. They proposed that high pressure voiding was responsible for the diverticulum. Since the patient had an enlarged prostate gland, he underwent a trans-urethral resection of the prostate, to relieve the obstruction followed by diverticulectomy. The origin of the diverticulum from the bladder wall was confirmed by surgery [10].
In our case report, ultrasound was used for the identification of the duplex moeity. However, it imaged what appeared to be a fluid-filled collection which was suspected to be the vagina. The CECT enabled the establishment of a normal vagina. However, in view of poor functioning of the upper moeity, contrast was not seen to delineate the ectopic upper moeity, which was seen to be in close proximity to the bladder neck. Static MR Urogram, by using heavily weighted T2 sequences used the residual urine within the ectopic ureter as intrinsic contrast for imaging. This was useful in the clear delineation of the pseudo-diverticulum and its course. Finally, the dynamic MCUG showed reflux into the ectopic ureter which was inserting into the bladder neck. DMSA showed a poorly functioning upper moeity. This resulted in a surgical decision to perform a partial nephrectomy.
Conclusion
In a patient with urinary incontinence, when a dilated irregular fluid-filled structure is seen on ultrasound posterior to the bladder in a patient where insertion of the ureter into the bladder is not visualized, a diagnosis of pseudo-diverticulum with ectopic ureter must be considered. Further, this case illustrates the importance of cross-sectional imaging in arriving at the diagnosis of a pseudo-diverticulum. Cases diagnosed previously as bladder neck diverticula may in fact be ureteral pseudo-diverticula. High resolution cross-sectional imaging can aid in the differential diagnosis. A dynamic contrast study like MCUG is invaluable in demonstrating reflux and site of ectopic ureteric insertion.
Informed consent authorizing the multiple modalities of investigations, to publish this case (including images and data) was obtained and is held on record.
[1]. Nilsson M, Ann L, Othon L, The impact of female urinary incontinence and urgency on quality of life and partner relationshipNeurourol Urodyn 2009 28(8):976-81. [Google Scholar]
[2]. Harris RL, Cundiff GW, Coates KW, Bump RC, Urinary incontinence and pelvic organ prolapse in nulliparous womenObstet Gynecol 1998 92(6):951-54. [Google Scholar]
[3]. Woodhouse CR, Myelomeningocele in young adultsBJU Int 2005 95(2):223-30. [Google Scholar]
[4]. Siomou E, Papadopoulou F, Kollios KD, Photopoulos A, Evagelidou E, Androulakakis P, Duplex collecting system diagnosed during the first 6 years of life after a first urinary tract infection: a study of 63 childrenThe Journal of Urology 2006 175(2):678-82. [Google Scholar]
[5]. Handler TF, Shapiro E, Incontinence in a child with a duplex kidney: case reportRev Urol 2002 4(1):44-48. [Google Scholar]
[6]. Bisset GS, Strife JL, The duplex collecting system in girls with urinary tract infection: Prevalence and significanceAm J Roentgenol 1987 148(3):497-500. [Google Scholar]
[7]. Borer JG, Bauer SB, Peters CA, Diamond DA, Decter RM, Shapiro E, A single-system ectopic ureter draining an ectopic dysplastic kidney: delayed diagnosis in the young female with continuous urinary incontinenceBr J Urol 1998 81(3):474-78. [Google Scholar]
[8]. Berrocal T, López-Pereira P, Arjonilla A, Gutiérrez J, Anomalies of the distal ureter, bladder, and urethra in children: embryologic, radiologic, and pathologic features 1Radiographics 2002 22(5):1139-64. [Google Scholar]
[9]. Curry NS, Ectopic ureteral orifice masquerading as a urethral diverticulumAmerican Journal of Roentgenology 1983 141(6):1325-26. [Google Scholar]
[10]. Michelotti B, Tomaszewski JJ, Smaldone MC, Benoit RM, Bladder diverticulum arising adjacent to an ectopic ureter presenting as a cystic massThe Canadian Journal of Urology 2008 15(2):4024-26. [Google Scholar]