Pregnancy is a dynamic state characterized by multiple changes in metabolism including increase in basal oxygen consumption and changes in use of energy substrate specifically by the fetoplacental unit [1]. Continuation of normal pregnancy needs normal placental growth with adequate supply of nutrients and oxygen to the developing fetus.
Early stages of pregnancy are associated with oxidative stress existing between the maternal decidua and villus placenta. This state of hypoxia exists prior to the development of maternofetal circulation. Low oxygen tension at this stage stimulates blastocyst hatching, normal cell differentiation and proliferation of cytotrophoblasts. This enables the establishment of placenta prior to the period of rapid fetal growth occurring in later half of pregnancy [2]. Insufficient blood flow to the placenta may establish a hypoxic environment, which upon reoxygenation results in ischemia/reperfusion injury, characterized by increased free radical generation and subsequent oxidative tissue damage [3]. On and off reduction in oxygenation becomes important as gestation progresses, as both the fetus and placenta extract considerable quantities of oxygen. Placenta being rich in mitochondria is one of the important sources of free radicals [4]. In addition reduction in uterine blood flow related to uterine contraction, changes in posture and activity further aggravate the state of oxidative stress. Hence throughout the pregnancy a constant state of oxidative stress is maintained. Severity of oxidative stress is dependent upon the ability of the tissues to combat free radicals via antioxidants. Mild disturbance in any of the protective mechanism leads to complications of pregnancy like preeclampsia, IUGR, preterm labour, spontaneous abortion etc., [5].
Human serum albumin consists of 585 amino acids forming a single polypeptide with structurally three homologous helical domains. First three amino acids in N – terminal region has specific binding sites for transition metals like cobalt, copper, nickel and is the most susceptible region for degradation compared to other regions of albumin. The mechanisms involved in ischemia/reperfusion induced invivo changes to albumin reduce the transitional metal binding capacity. This new chemically changed albumin is called as Ischemia Modified Albumin (IMA). IMA is a candidate biomarker proposed or used for detection of cardiac ischemia and is a good discriminator between ischemic and non-ischemic patients. IMA is found to be elevated both in cardiac and extra cardiac causes of oxidative stress originating from ischemia reperfusion injury [6–8].
To measure maternal serum IMA in normal pregnancy and correlate it with MDA, which is a well-known product of lipid peroxidation, hence a marker of oxidative stress.
Materials and Methods
This case control study was carried out in Department of Biochemistry in collaboration with the Department of Obstetrics and Gynecology for a period of one year from July 2012 to August 2013 after being accepted by the institutional ethical committee.
Inclusion Criteria
Forty pregnant women with ≥20 weeks of gestation without any major illnesses and not under any medications except supplementation for iron, calcium and multivitamins were selected for the study. Forty one voluntary age matched healthy non-pregnant women were taken as the control.
Exclusion criteria
Pregnant women with bad obstetrical history, previous pregnancy with hypertensive disorders, hypertension before or during gestation, diabetes previous to pregnancy, gestational diabetes mellitus, existing liver, cardiac or renal diseases, recurrent pregnancy loss, multiple pregnancy, history of smoking, ischemic heart disease, peripheral vascular diseases were excluded from the study.
Sample Collection
A 5 ml of fasting venous blood sample was collected for analysis of biochemical parameters after taking written consent from the study group. Blood hemoglobin was estimated by Cyanmethemoglobin method, fasting blood glucose by Glucose Oxidase Peroxidase method, serum urea by Urease, serum creatinine by Modified Jaffe’s, serum uric acid by Uricase method and serum albumin was estimated by Bromocresol green method. All these biochemical parameters were analysed by Cobas integra autoanalyser.
Serum IMA Estimation
Serum IMA was estimated by Bar o et al., method [9]. A known amount of cobalt was added to the serum specimen and unbound cobalt was measured from absorbance of coloured complex by addition of Dithiothreitol (DTT). IMA was reported in absorbance units (ABSU) i.e., 1ABSU= 100* Optical Density. IMA was normalized to serum albumin to minimize the effect of decrease of serum albumin on IMA.
Serum MDA Estimation
Serum MDA was estimated by Thiobarbituric Acid Reactive Substances (TBARS) method [10]. During peroxidation, peroxides are decomposed to aldehydes like malondialdehyde (MDA), which can be detected by thiobarbituric acid that gives an easily measurable pink colour.
Statistical Analysis
Data was analysed using Graph pad prism, Microsoft excel and SPSS 17 version. Results were expressed as mean±SD. Correlation of IMA, IMA/Albumin with MDA was done by Pearson’s correlation analysis. The p <0.05 was considered as statistically significant.
Results
[Table/Fig-1] shows that both the cases and control groups were age matched. There was no significant difference observed for hemoglobin, serum urea and creatinine. Uric acid was found to increase in pregnant women compared to non-pregnant healthy control (p<0.001). Serum albumin was significantly decreased in cases (3.66±0.48gm/dl)compared to the controls (4.63±0.48gm/dl).
Biochemical parameters in the study group.
| Parameters | Normal Pregnancy(N=40) | Non-Pregnant(N=41) |
|---|
| Age(in yrs) | 26.78±2.60 | 26.92± 1.94 |
| Hb (gm/dl) | 10.75±1.02 | 11.13±0.97 |
| FBS (mg/dl) | 81.42±12.84 | 78.59±10.57 |
| Ur (mg/dl) | 24.7±7.54 | 24.14±4.64 |
| Cr (mg/dl) | 1.06±0.18 | 1.03±0.18 |
| UA (mg/dl) | 5.19±0.67 | 4.09±0.72* |
| S. Alb (gm/dl) | 3.66±0.48 | 4.63±0.48* |
| IMA (IU/l) | 72.54±9.89 | 48.47±8.30* |
| IMA/Alb | 20.16±3.94 | 10.51±1.76* |
| MDA(ng/ml) | 2.87±1.24 | 1.00±0.38* |
*p-value <0.001.
Serum IMA and IMA/Albumin was found to be significantly (p < 0.001) increased (72.54± 9.89IU/L, 20.16±3.94) compared to the non-pregnant healthy controls (48.47±8.30 IU/L, 10.51±1.76). Similarly serum MDA was observed significantly higher in normal pregnancy compared to controls.
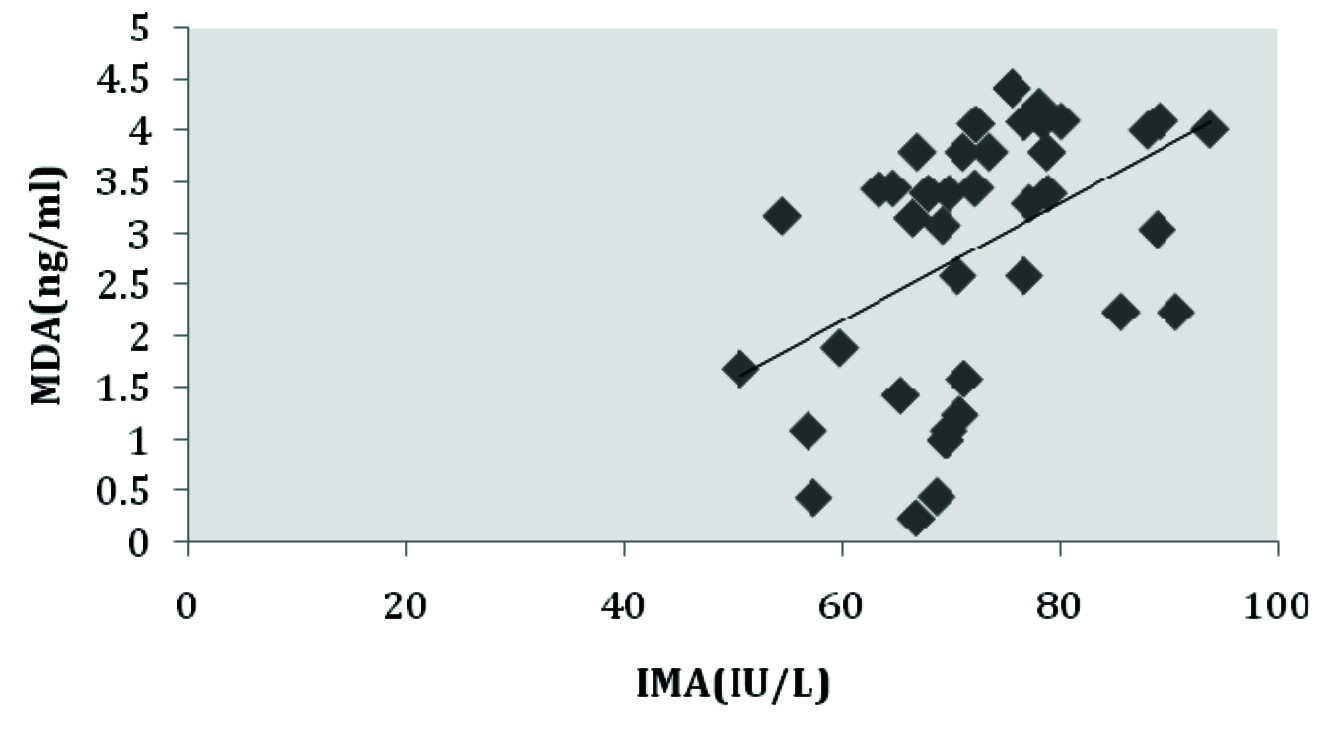
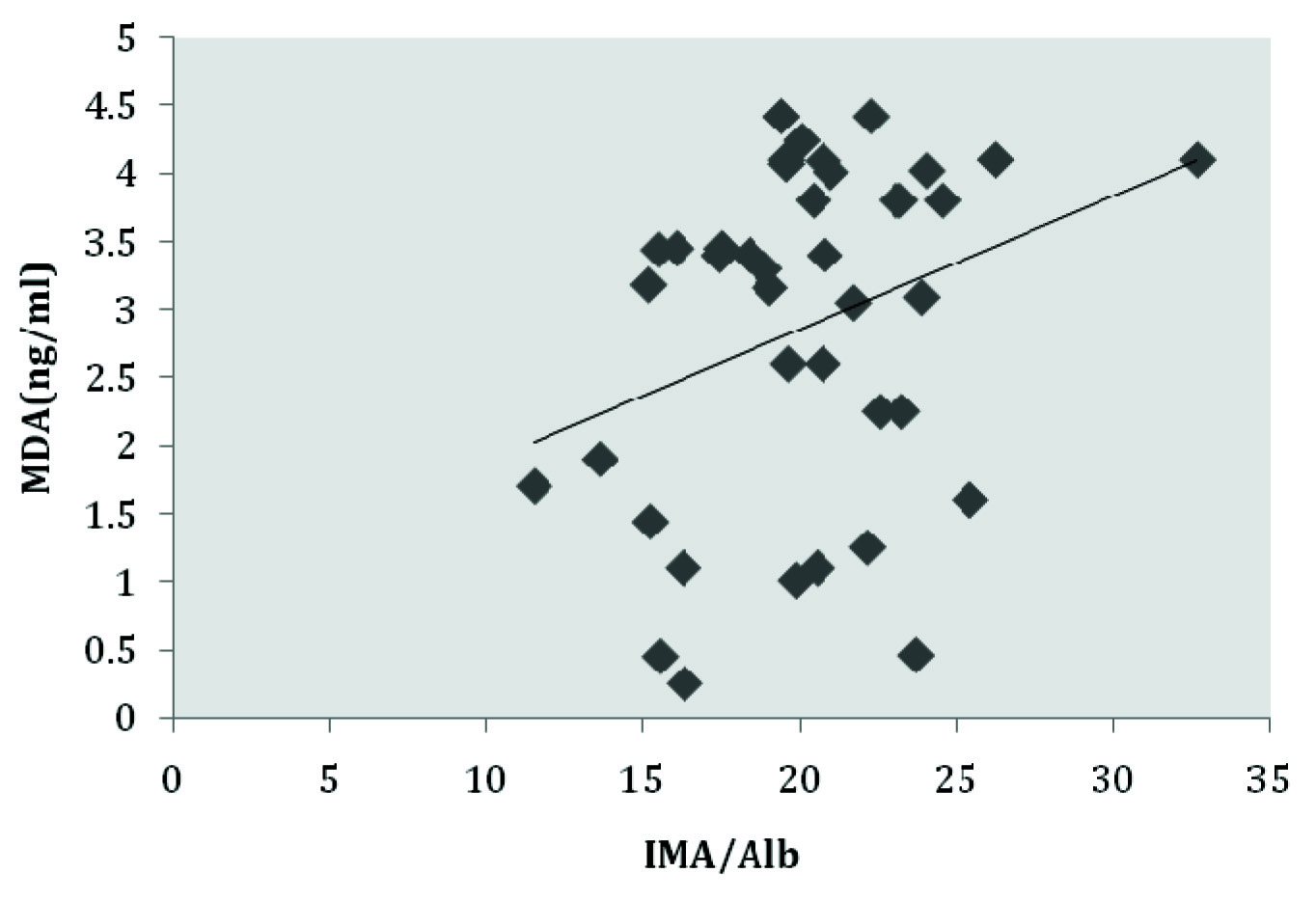
[Table/Fig-2,3] shows maternal serum IMA and IMA/Albumin is positively correlated with serum MDA in normal pregnant women.
Correlation between serum IMA and MDA in normal pregnant women.
Correlation between serum IMA/Alb and MDA in normal pregnant women.
Discussion
Increase in demand of blood supply and vascular transformation in pregnancy leading to hypoxic ischemic reperfusion injury results in generation of Readive Oxygen Species (ROS) and oxidative stress [11,12]. Oxidative stress is a state of imbalance between generation of ROS and level of antioxidant defense system. Though many antioxidant defense mechanisms come to action but pregnancy is a physiological condition where there is high chance of imbalance between pro-oxidant and antioxidants.
In the present study there was increase in IMA in normal pregnant women (72.54± 9.89IU/L) compared to non-pregnant healthy controls (48.47±8.30U/L,10.51±1.76). IMA was normalized to albumin to minimize the effect of decrease in serum albumin seen during pregnancy as done by Van Rijn et al., Our study is in accordance to the study done by Guven et al., Rossi a et al., and Van Rijn et al., who observed maternal serum IMA levels in normal pregnant women were significantly increased (p< 0.05) suggesting increase oxidative stress in normal pregnancy [13–15]. Rossi et al., found that IMA concentration increased with increase in gestational weeks. Though IMA has a short half-life it is continually produced during ischemic event, hence irrespective of gestational weeks it remains high throughout the pregnancy [14]. This finding supports the hypothesis that normal trophoblastic development is associated with hypoxic intrauterine environment, with increase in substrate need and change in metabolism in the fetoplacental unit [16]. Oxidative stress that develops from post-ischemic reperfusion has an important role in normal pregnancy development. Poor trophoblastic invasion and spiral artery vasoreactivity results in more ischemic environment, the exaggeration of which can result in complications related to pregnancy manifested in its later half. Rossi et al., even found out that first trimester IMA levels are well above the cut-off value used for diagnosis of cardiac ischemia [14]. ROS, produced during ischemia generates highly reactive hydroxyl free radicals causing site specific modification of N-terminus of albumin resulting in loss of binding capacity of the albumin to transition metals resulting in the formation of IMA [17].
MDA was found to significantly increase in our cases compared to the controls, which is in accordance to the study done by Saikumar P et al., Ghate J et al., and Patil et al., who found that even in uncomplicated pregnancy there is increased oxidative stress and lipid peroxidation as shown by the increased serum MDA levels as gestation advances [11,12,18]. Lipid peroxidation occurs with the interaction of ROS with lipids. During pregnancy human placenta produces lipid peroxides that are secreted to maternal side leading to increase in lipid peroxide products in maternal circulation [19]. Malondialdehyde (MDA) is one of the final products of PUFA peroxidation and well correlated with lipid peroxidation [20]. A statistically significant correlation was found out between maternal serum MDA with IMA and IMA/Alb, suggesting serum IMA increases with increase in oxidative stress. These findings suggest that IMA can also be considered as an effective marker of oxidative stress.
Various protective mechanisms develop against free radical generation and damage during pregnancy but degree of oxidative stress depends upon balance between the defense mechanisms and free radical producing mechanisms.
Limitation
The study was performed in a limited study group, IMA at different trimester of pregnancy was also not compared. Similarly IMA in normal pregnancy was also not compared with complicated pregnancies.
Conclusion
Serum ischemia modified albumin a marker of cardiac ischemia is also increased in normal pregnancy. So continuous monitoring of serum IMA can give us an idea regarding progress of pregnancy. Any deviation or increase can suggest complications in pregnancy. This can help us to intervene earlier in complications and prevent the mortality and morbidity related to it. IMA being positively correlated with MDA can also be considered as the marker of oxidative stress. Consideration should be done while selecting IMA as marker of cardiac ischemia in normal pregnant women.
Considerably more work will need to be done to know the cut-off value of serum IMA at different trimesters of pregnancy so that it can be used to know the vulnerable period for fetal health and gestational process. Correlation of fetal blood oxidation status to that with placenta and with systemic circulation of pregnant mother should also be done. Future works should be emphasized, where pregnancy should be followed with its outcome for better establishment of IMA as a marker of oxidative stress in pregnancy.
*p-value <0.001.