Introduction
Morphological variations of articular facets of calcaneum may predispose people to joint instability, ligamentous laxity and development of arthritic changes in the subtalar joint. Knowledge of such variations is essential for treatment and diagnostic procedures in orthopaedic surgeries.
Aim
The aim of this study was to determine patterns of articular facets of calcanei and to establish its correlation with calcaneal spurs.
Materials and Methods
The study was conducted on 580 adult calcanei of Indian origin at Maulana Azad Medical College and pattern of articular facets were observed and classified according to five patterns described in literature. A digital vernier calliper was used to measure separation between anterior and middle facet. Degree of intersecting angle between anterior and medial facets was calculated using UTHSCSA Image Tool software. The calcaneal spurs were observed by visual inspection.
Results
Out of 580 calcanei, 66.55% had fused anterior and middle facets (Pattern I), 27.59% had all three facets separate (Pattern II), 5.52% had absence of anterior facet (Pattern III), 0.17% had all three facets fused (Pattern IV) and 0.17% had fused middle and posterior facets (Pattern V). A significant side variation was present in Pattern III with predominance on left side. Mean angle of intersection was 147.700 in Pattern I and 133.340 in Pattern II calcaneum. Calcaneal spurs were found in 61.38% out of which it was associated with Pattern I in 43.62%, Pattern II in 14.66% and Pattern III in 2.76%.
Conclusion
Individuals with Pattern I and III calcaneum were found to be at a greater risk of subtalar joint instability than individuals with Pattern II. Angle of intersection was obtuse in Pattern I which resulted in ligament laxity and unstable joint. Pattern I was more common in Indian population and this fact necessitates modifications of the western surgical techniques to suit the Indian scenario. An association between the presence of spur and facet configuration was found to be significant.
Introduction
Anterior and posterior articulations between the calcaneum and talus form a functional unit often termed the ‘subtalar joint’. There are three talar facets over the superior surface of calcaneum which contributes in the formation of this joint, namely anterior, middle and posterior facet. The anterior and middle facets lie on anterior one third of the calcaneum and articulate with the head of the talus while the posterior facet, which lies on the middle one third of calcaneum, articulates with the body of talus [1].
These facet configurations are probably genetically determined and are not developmental responses to walking habits, physique of a person, duration of weight bearing in post-natal life [2,3]. A comparison of the adult African, Indian and European calcaneal bones have revealed distinct racial difference in adult bones [2]. Racial and individual differences of articular facets of calcaneum have an important role on static and kinetic dynamics of the foot [2,4,5].
Morphological variations of talar articular facets may predispose people to joint instability, ligamentous laxity and development of arthritic changes in the subtalar joint [6,7]. Knowledge of the patterns is important during treatment of talocalcaneal arthritis and coalition, intraarticular fractures, congenital dysmorphology, club foot, severe pronation cases, subtalar instability and valgus deformities. Morphometric values of calcanei are of significance for the science of anatomy, orthopaedic surgery, kinesiology, physical treatment and rehabilitation sections [2,4,5]. Detailed anatomic information forms baseline for advanced treatment procedures such as subtalar implants and prosthesis for foot [5]. Chronic heel pain and instability of ankle can also be analyzed as these are associated with pre-existing anatomic variations.
Foot and ankle surgeons have observed subtalar instability as a major podiatric problem because it can lead to severe flatfoot with growing pain and quick fatigue while walking and running. It can lead to many orthopaedic problems affecting ankle, knee, hip joint and lower back and result in clinical presentations like anterior or posterior tibial tendonitis, plantar fasciitis and forefoot pain [8,9].
Calcaneal spurs are formed at the site of insertion of tendons and ligaments into bone. Spurs can be dorsal (posterior) or plantar (inferior) and tend to grow in the direction of the pull of tendons and ligaments [10]. Incidence of calcaneal spurs increase with age and is associated with configuration of articular facets, physical activity and concurrent orthopaedic diseases. Gerster et al., found that the incidence of calcaneal spur was maximum in patients of osteoarthritis (56%), followed by reiter’s syndrome (37.4%), ankylosing spondylitis (31.2%) and rheumatoid arthritis (24%) [11]. Menz et al., reported a positive correlation between calcaneal spur and osteoarthritis and found that individuals with plantar spurs were more likely to be obese [12]. Williams et al., found on plain X-ray that 39 out 52 painful heels (75%) showed plantar spurs, compared with 5 of 63 (7.9%) heels in age and sex matched controls. This suggests association of calcaneal spurs with heel pain [13].
Hence, the present study was carried out to know the variation in the patterns of the articular facets of calcanei and to evaluate its relationship with subtalar joint morphology and to establish the correlation of calcaneal spurs with specific facet patterns.
Materials and Methods
The observational study was conducted on 580 (280 right and 300 left) adult human calcanei of Indian origin, from August 2014 to December 2015 at Department of Anatomy, Maulana Azad Medical College, New Delhi, India. Calcaneum with obscuring pathologies such as cortical bone deterioration was excluded from the study. All the calcanei were numbered for identification. Pattern of articular facets on calcaneum were observed and classified according to five patterns described in the studies of Saadeh et al., and Gupta et al., [Table/Fig-1] [14,15]. In calcanei with pattern II, a digital vernier calliper (with a range of 0 to 150 mm and with the least count of 0.02) was used to measure separation between anterior and middle facet. Distance was measured between posterior most part of anterior facet and anterior most part of middle facet. Depending on the degree of separation between anterior and middle facets, pattern II was divided into three subtypes [Table/Fig-1].
Classification of calcaneal articular facets [14,15].
| Pattern | Feature | Subtype | Feature |
|---|
| I | Fused (continous) anterior & middle facetsSeparate posterior facet | IA | Constricted continous facet |
| IB | Non-constricted continous facet |
| II | Separate anterior & middle facetsSeparate posterior facet | IIA | Degree of separation between anterior & middle facet is < 2mm |
| IIB | Degree of separation is between 2-5 mm |
| IIC | Degree of separation is between > 5 mm |
| III | Absence of anterior facet (only middle facet present)Separate posterior facet |
| IV | Fused anterior, middle & posterior facets |
| V | Fused middle & posterior facets |
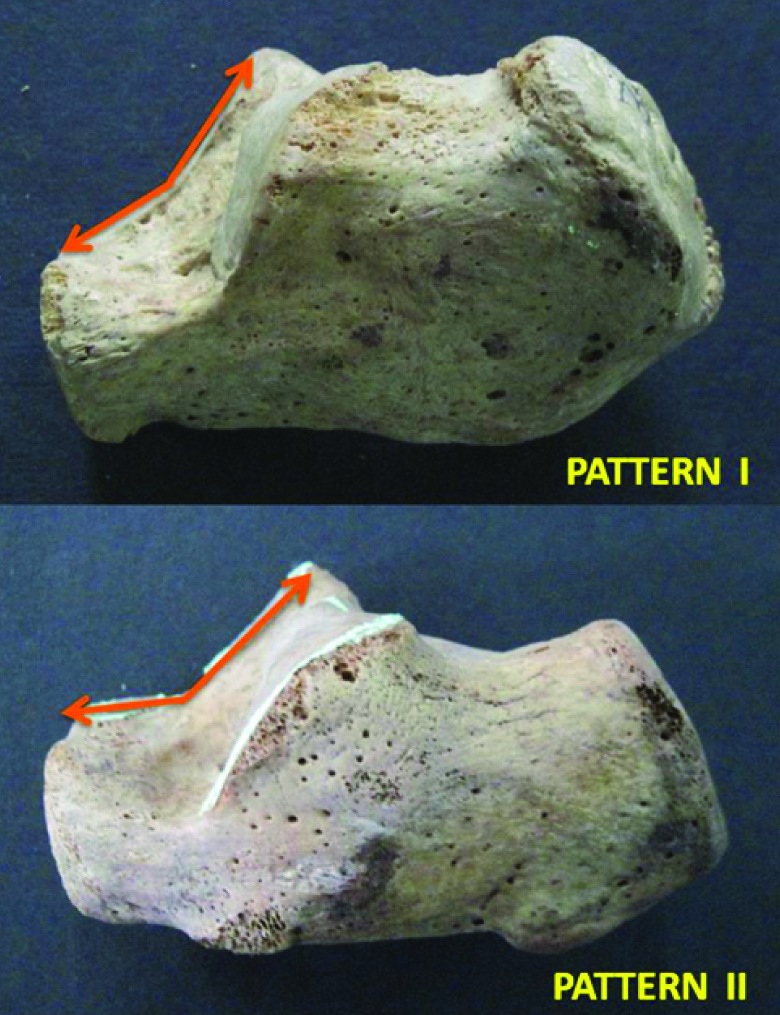
After classifying the patterns of calcanei, degree of intersecting angle was measured between anterior and middle facets. The calcaneum was placed on its medial side on a horizontal surface so that the plane of the facets was perpendicular to the horizontal surface. All the calcanei were photographed in this position and then the angle of intersection was measured with the help of UTHSCSA Image Tool software. After importing these photographs to the software Image Tool, a reference point was taken at the maximum point of concavity between anterior and medial facet and then a line was drawn parallel to the plane of anterior facet with Image Tool. Then from the same previous reference point, another line was drawn parallel to the plane of medial facet. The angle was measured twice for each calcaneum and the mean was recorded [Table/Fig-2].
Measurement of angle of intersection between anterior & middle facet.
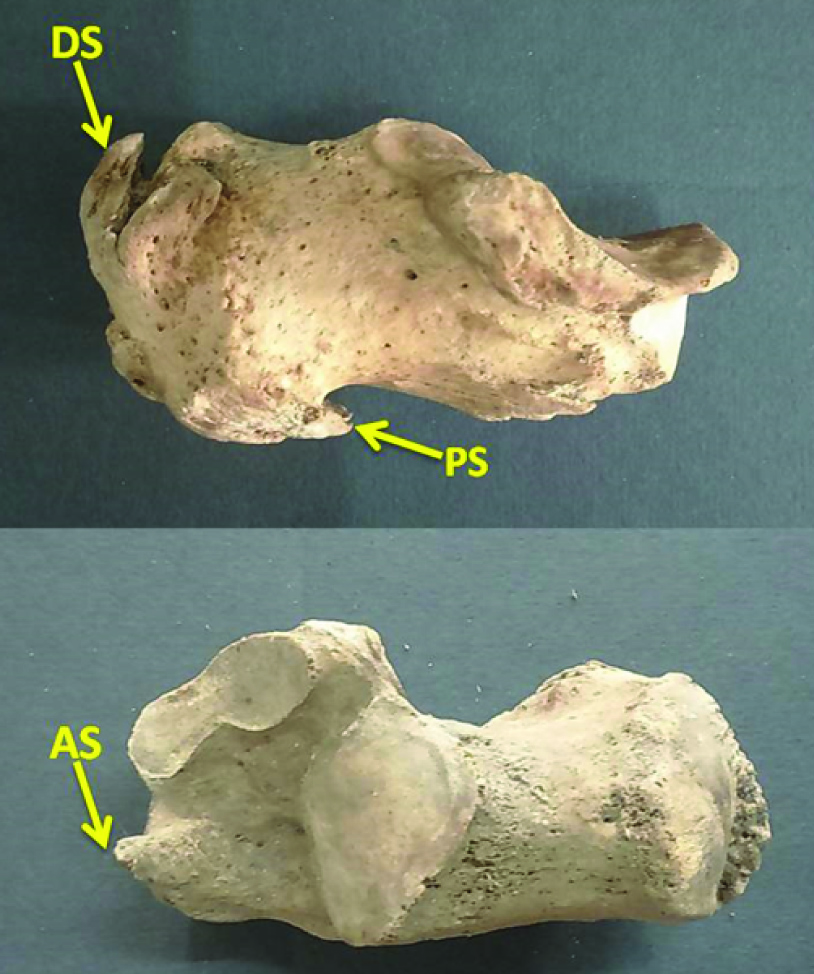
Presence of dorsal (posterior) and plantar (inferior) calcaneal spurs was noted by visual inspection [Table/Fig-3].
Calcaneum showing Dorsal (DS), Plantar (PS) and Anterior (AS) Spurs.
All observations and measurements were made by two different observers and in case of any discrepancy, either the observation was repeated or the mean was calculated for parameter. To avoid any observer bias, the second observer was kept oblivious of the observations obtained by the first observer.
Statistical Analysis
Incidence of various patterns of the articular facets of the calcaneum and their subtypes were calculated as percentage and compared with available literature. Incidence of plantar and dorsal spurs were also calculated and compared with previous data. Mean, range and standard deviation of the angle of intersection were calculated for pattern I and II.
Chi-Square test and Student’s t-test in Microsoft Excel 2007 was used for the statistical analysis. The relationship between the examined variables was assessed and a level of significance of p < 0.05 was used.
Results
Out of 580 calcanei (280 right and 300 left), pattern I with fused anterior and middle facets [Table/Fig-4] was predominant and was observed in 66.55% (191 right and 195 left calcanei) followed by pattern II with separate anterior, middle and posterior facets [Table/Fig-5] in 27.59% (65 right and 95 left calcanei). Pattern III with absence of anterior facet [Table/Fig-6] was found in 5.52% (17 right and 15 left calcanei). Pattern IV with all three facets fused and pattern V with fused middle and posterior facet [Table/Fig-6] were observed in one calcaneum each (0.17%) and in both cases, the calcaneum belonged to right side. The Chi Square result showed a significant statistical difference (p= 0.022) depicting significant side variation in the frequency of pattern III with predominance on left side. The Chi Square results for the rest of the patterns did not depict side variation.
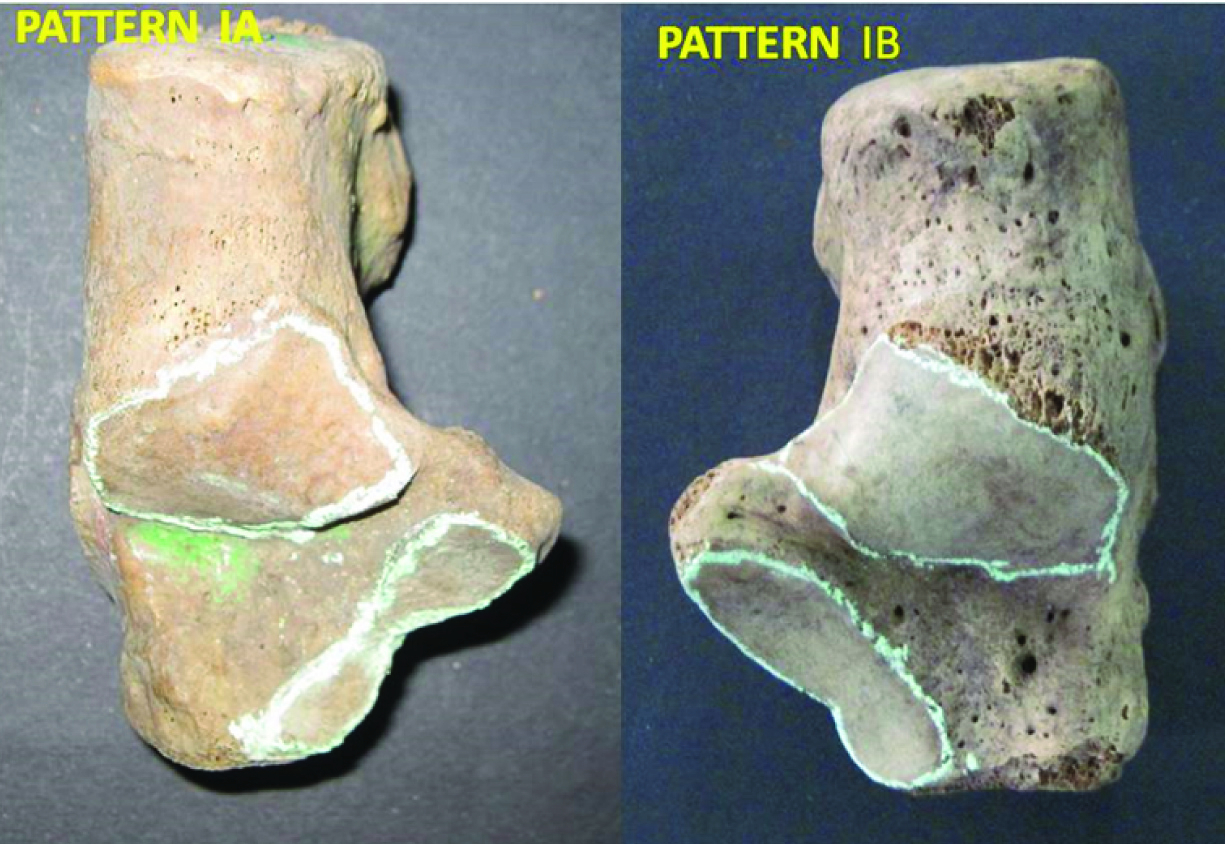
Calcaneum showing Pattern I (fused middle and anterior facets) having Subtype A (constricted facet) and Subtype B (non-constricted facet).
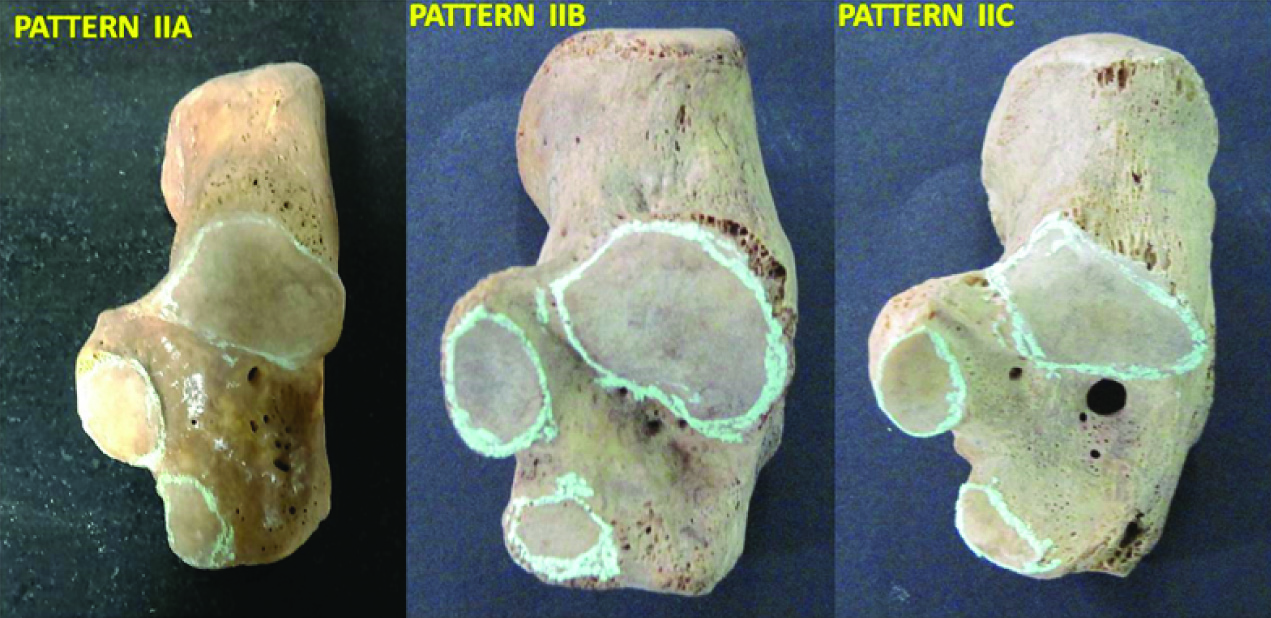
Calcaneum showing Pattern II (separate middle and anterior facets) having Subtype IIA (<2mm), Subtype IIB (2-5mm) and Subtype IIC (>5mm).
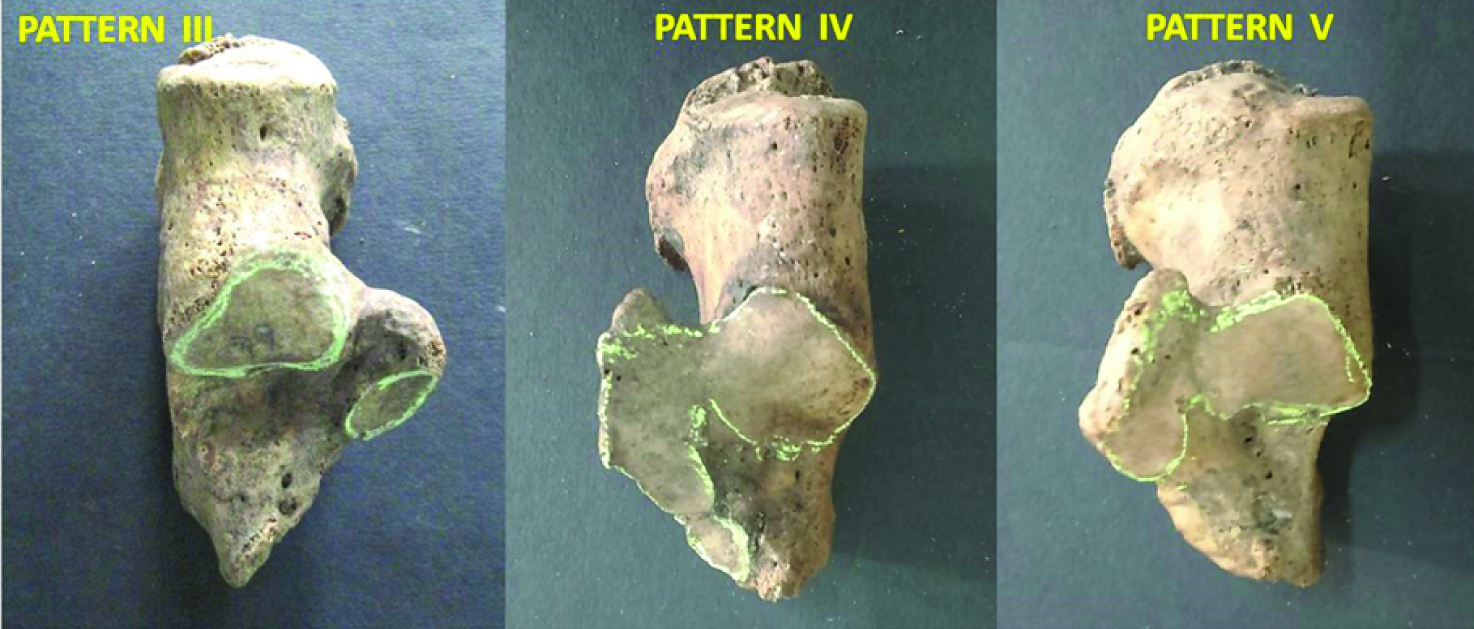
Calcaneum showing Pattern III (absence of anterior facet), Pattern IV (fused anterior, middle and posterior facets) and Pattern V (fused middle & posterior facets).
In pattern I, calcanei with constricted continuous facet was found in 185 bones (31.90%) and with non-constricted continuous facet was found in 201 bones (34.66%). In pattern II, subtype A with anterior and middle facet separation of less than 2 mm was seen in 38 bones(6.55%), subtype B with anterior and middle facet separation of 2-5mm was seen in 96 bones(16.55%) and subtype C with separation more than 5 mm was observed in 26 bones (4.48%).
Mean angle of intersection was 147.700 in Pattern I and 133.340 in Pattern II calcaneum. The angle was found statistically equal on right and left side [Table/Fig-7].
Angle of Intersection in the present study.
| Mean of Angle of Intersection (°) | Standard Deviation | p-value |
|---|
| Pattern I | Right | 148.02 | 6.39 | 0.164 |
| Left | 147.39 | 6.22 |
| Pattern II | Right | 133.49 | 6.63 | 0.40 |
| Left | 133.24 | 6.19 |
Calcaneal spurs were found in 356 calcanei (61.38%) out of which only dorsal spurs were found in 156 calcanei (26.90%), only plantar spurs in 80 calcanei (13.79%) and both dorsal and plantar spurs in 119 calcanei (20.52%). In one calcaneum (0.17%), anterior spur was observed [Table/Fig-6]. Calcaneal spurs were present in 43.62% of calcanei with long continuous facet, in 14.66% of calcanei with two separate facets on sustentaculum tali, in 2.76% of calcanei with medial facet only, in 0.17% of calcaneum with all facets fused and in 0.17% of calcanei with fused middle and posterior facets. A Chi-Square test for an association between the presence of spur and facet configuration was found to be significant (p =0.033).
Discussion
Pattern I calcaneum was found to be the commonest in the present study which is in accordance with other Indian studies [15–18] as well as in Egyptian[14], Turkish [19] and Spanish [20] studies. In contrast to this, Pattern II was predominant in Europeans [2] and Belgians [21]. American population [7,22] also showed predominance of Pattern I [Table/Fig-8] [2,7,14–22].
Comparison of incidence of patterns of calcaneal articular facets with previous data (n=total number of calcanei studied).
| Sl. No. | Author | Year | Population | n | Type I(%) | Type II(%) | Type III(%) | Type IV(%) | Type V(%) |
|---|
| 1 | Burning & Barnett [2] | 1965 | European | 194 | 33 | 67 | -- | 00 | -- |
| 2 | Gupta SC et al., [15] | 1977 | Indian | 401 | 67 | 26 | 5 | 2 | -- |
| 3 | Camposs & Pellicio [20] | 1989 | Spanish | 176 | 53.41 | 39.77 | 6.82 | 00 | -- |
| 4 | Verhagen FD [7] | 1993 | American | 191 | 54.45 | 26.7 | 18.85 | -- | -- |
| 5 | Saadeh FA et al., [14] | 2000 | Egyptian | 300 | 63 | 30.3 | 4.7 | 02 | -- |
| 6 | Barbaix E et al., [21] | 2000 | Belgian | 134 | 25 | 64 | 11 | 00 | -- |
| 7 | Regab A et al., [22] | 2003 | American | -- | 46 | 25 | 12 | 0.2 | -- |
| 8 | Uygur M et al., [19] | 2009 | Turkish | 221 | 58.37 | 34.39 | 4.98 | 2.2 | -- |
| 9 | Muthukumaravel N et al., [16] | 2011 | S Indian | 237 | 65.82 | 33.33 | -- | 0.42 | 0.42 |
| 10 | Garg R et al., [17] | 2012 | Indian | 310 | 72.26 | 24.52 | 1.3 | 1.6 | 0.32 |
| 11 | Nemade KS et al., [18] | 2013 | Indian | 220 | 65.45 | 25.45 | 9.09 | -- | -- |
| 12 | Present study | 2016 | Indian | 580 | 66.55 | 27.59 | 5.52 | 0.17 | 0.17 |
These findings establish the racial and individual difference in the patterns of the articular facets of calcaneum, for which no functional explanation can readily be offered.
In the present study, in pattern II, subtype B (2-5mm) was the commonest one (16.55%). This finding coincided with the finding of Muthukumaravel N et al., and Camposs and Pellicio, [16,20], while in studies by Saadeh FA et al., Gupta SC et al., Garg R et al., and Uygur M et al., subtype C (>5mm) was common [Table/Fig-9] [14–17,19,20]. Thus, racial difference as well as difference with in the Indian population was observed.
Comparison of incidence of subtypes of pattern II with previous data (n=total number of calcanei studied).
| Sl. No. | Study | Year | Population | n | Subtype A<2mm | Subtype B 2-5mm | Subtype C >5mm |
|---|
| 1. | Gupta SC et al., [15] | 1977 | Indian | 401 | 9% | 4% | 13% |
| 2. | Camposs & Pellicio [20] | 1989 | Spanish | 176 | 2.84% | 21.02% | 15.91% |
| 3. | Saadeh FA et al., [14] | 2000 | Egyptian | 300 | -- | 6.7% | 23.7% |
| 4. | Uygur M et al., [19] | 2009 | Turkish | 221 | 4.08% | 13.12% | 17.19% |
| 5. | Muthukumaravel N et al., [16] | 2011 | South Indian | 237 | -- | 27% | 6.32% |
| 6 | Garg R et al., [17] | 2013 | Indian (Rajasthan) | 310 | 4.8% | 7.7% | 8.1% |
| 7. | Present Study | 2016 | Indian | 580 | 6.55% | 16.55% | 4.48% |
Pattern IV which has been scarcely reported in the previous studies, was observed in the present study is 0.17%. The unique finding of the present study was the presence of pattern V in 0.17% which has been very rarely reported in the literature. Pattern V calcaneum (fused middle and posterior facets) found in the present study had absence of the anterior facet in contrast to Muthukumaravel N et al., and Garg R et al., who reported pattern V calcaneum with a distinct anterior facet [16,17].
Bruckner stated that sustenteculum tali facet variations are clinically important because they influence subtalar joint stability [6]. The subtalar joint formed by calcanei which had the pattern II facet configuration were comparatively more stable and had lower frequency of arthritic changes. The 2-facet configuration is typically associated with a higher angled subtalar joint axis and a sharper intersecting angle [7]. These two facets along with the posterior facet provide an ‘osseous tripod’ for the talus to sit on and to prevent excess motion of the talar head. Thus, the subtalar joint is less likely to suffer trauma, accidents or other biomechanical stress and the incidence of osteoarthritis is less [6,7].
Pattern I configuration can cause laxity of the spring ligament and other supporting muscles due to the continuous and excessive pressure which is exerted by the talar head due to its increased mobility and uneven weight distribution. This is due to the presence of fused anterior and middle facet which is continuous, flat and smooth, thus giving fewer impediments to the medial rotation of the talar head. Eventually, the subtalar joint formed by calcanei with pattern I facet configuration are relatively unstable and more prone to osteoarthritis [7].
In Pattern III calcanei, the arthritic changes and intersecting angle is midway between Pattern I and II. Here, sustentaculum tali with only a medial facet provide inadequate talar head support which allows excessive anterior and inferior rotation of talus. This results in valgus position of calcaneum and downward tilt of talar head [23]. Hence, the increased pressure on the anterior subtalar joint capsule causes ligamentous laxity [24]. CT scans show that flat foot is associated with Pattern III [25].
The deformities in pes planus are corrected by procedure “Lengthening-distraction wedge calcaneal osteotomy and interposition bone graft” during which the identification of the interval between the anterior and middle facet is important for the exact placement of the retractor by the orthopaedic surgeons [26]. Since the line of osteotomy usually passes through the interval between anterior and middle facets, this technique is suitable for the Europeans with prominent pattern II calcanei. Pattern I calcanei is commonly seen in Indians, the anterior and middle facets are fused and the subtalar joint must be violated to perform this operation. This fact necessitates modification of the western surgical technique to suit the Indian scenario [16].
In the ‘triple arthrodesis’ procedure to correct the deformities of flatfoot, the articular facet configurations of the calcaneum should be clearly kept in mind in order to safely denude the surfaces of the subtalar joints of all the articular cartilages [26]. Treatment of complete foot deformity requires osteotomy, anatomic reduction and relaxation of soft tissue, for which anatomical knowledge of the foot is essential [17].
The incidence of calcaneal spurs was high (61.38%) in the present study which is in accordance with Australian (55.1%) [12] and South Indian (56%) studies [27]. Riepert et al., reported relatively low incidence of spurs (15.70%) in European population [28]. The incidence of only dorsal spur was highest (26.90%) in the current study and this finding coincides with Kullar JS et al., (15.5%) [29] [Table/Fig-10]. Anterior spur (0.17%) observed in the present study has not been reported earlier.
Comparison of incidence and type of calcaneal spurs with previous data. (n=total number of calcanei studied).
| Sl. No. | Study | Year | Population | n | Plantar Spurs(%) | Dorsal Spurs(%) | Both Spurs(%) | Total Spurs(%) |
|---|
| 1. | Riepert et al., [28] | 1995 | European | -- | 11.2 | 9.3 | -- | 15.70 |
| 2. | Menz et al., [12] | 2008 | Australian | 216 | 55 | 48 | -- | 55.1 |
| 3. | Perumal and Anand [27] | 2013 | Indian(Tamilnadu) | 218 | -- | -- | -- | 56 |
| 4. | Kullar JS et al., [29] | 2014 | Indian (Punjab) | 200 | 6.5 | 15.5 | 4.5 | 26.5 |
| 5. | Present study | 2016 | Indian | 580 | 13.79 | 26.90 | 20.52 | 61.38 |
In the current study, Pattern I calcanei has been found to be most frequently associated with spurs (43.62%) which is in accordance to Kullar JS et al., [29]. He found absence of spurs in pattern III in Indian study but it was observed in 2.76% of calcanei in our study.
Limitation
The sex, age and occupation of each individual from whom the calcaneum was obtained was not known. Therefore, the study could not provide a relationship between gender and configuration of the articular facets. Also, association of the frequency of the calcaneal spurs with increasing age and varied physical activity could not be established.
Conclusion
The articular facets on calcanei show racial and individual differences. Pattern I is more common in Indian population as compared to Europeans who have pattern II and thus modifications of the western surgical techniques are needed to suit the Indian scenario. Individuals who display Pattern I and III calcaneum are found to be at a greater risk of subtalar joint instability than individuals with Pattern II. Angle of intersection is obtuse in Pattern I which puts more strain on the talar head during heel strike resulting in ligament laxity and unstable joint. The present study population may be at a greater risk of developing subtalar arthritis due to the dominance of Pattern I calcanei. An association between the presence of spur and facet configuration was found to be significant. The Pattern V observed in the present study is a unique finding and has been scarcely reported in the previous studies.
[1]. Williams PL, Gray H, Bannister LH, Gray’s Anatomy. In Skeletal system 1995 38th edNew York, LondonChurchill Livingstone:715Soames, RW Edn [Google Scholar]
[2]. Bunning PSC, Barnett CH, A comparison of adult and foetal talocalcaneal articulationsJournal of Anatomy 1965 99(1):71-76. [Google Scholar]
[3]. Rehman FU, Study of human fetal calcaneal articular facetsInternational Journal of Developmental Research 2014 4(7):1362-65. [Google Scholar]
[4]. Ananthakrisnan D, Ching R, Tencer A, Hansen ST, Sangeorzan BJ, Subluxation of the talocalcaneal joint in adults who have symptomatic flatfootJ Bone Joint Surg 1999 81(8):1147-54. [Google Scholar]
[5]. Dogan A, Albayrak M, Akman YE, Zorer G, The results of calcaneal lengthening osteotomy for the treatment of flexible pes planovalgus and evaluation of alignment of the footActa Orthop Traumatol Turc 2006 40:356-66. [Google Scholar]
[6]. Bruckner J, Variations in the human subtalar jointJournal of Orthopaedic and Sports Physical Therapy 1987 8:489-94. [Google Scholar]
[7]. Verhagen FD, Arthritis of the subtalar joint associated with sustentaculum tali facet configurationJournal of Anatomy 1993 183:631-34. [Google Scholar]
[8]. Weil L, Emphasizing careful assessment of the etiology and underlying contributing factor to subtalar joint instabilityPodiatry today 2007 20:5 [Google Scholar]
[9]. John E, Sprains- residual instability of subtalar, Lisfranc joint and turf toeClin. Sports Medicine 2004 23:97-121. [Google Scholar]
[10]. Rogers J, Shepstone L, Dieppe P, Bone formers: Osteophyte and enthesophyte formation are positively associatedAnn Rheum Dis 1997 56:85-90. [Google Scholar]
[11]. Gerster JC, Vischer TL, Bennani A, Fallet GH, The painful heel. Comparative study in rheumatoid arthritis, ankylosing spondylitis, Reiter’s syndrome, and generalized osteoarthrosisAnn Rheum Dis 1977 36:343-48. [Google Scholar]
[12]. Menz HB, Zammit GV, Landorf KB, Munteanu SE, Plantar calcaneal spurs in older people: Longitudinal traction or vertical compression?J Foot Ankle Res 2008 1:7 [Google Scholar]
[13]. Williams PL, Smibert JG, Cox R, Mitchell R, Klenerman L, Imaging study of the painful heel syndromeFoot Ankle 1987 7:345-49. [Google Scholar]
[14]. Saadeh FA, Fuad AH, Mahmoud SMI, Marwan EE, Patterns of the talar articular facets of Egyptian calcaneiJournal of Anatomical Society of India 2000 49(1):6-8. [Google Scholar]
[15]. Gupta SC, Gupta CD, Arora AK, Patterns of talar articular facets in Indian calcaneiJournal of Anatomy 1977 124(3):651-55. [Google Scholar]
[16]. Muthukumaravel N, Ravichandran D, Melani RS, Human calcaneal facets for the talus: patterns and clinical implicationsJournal of Clinical and Diagnostic Research 2011 5(4):791-94. [Google Scholar]
[17]. Garg R, Dagal N, Kumar S, Shekhawat S, Study of patterns of talar articular facets of human calcanei and their clinical implications in population of RajasthanIndian Journal of Basic & Applied Medical Research 2013 7(2):643-50. [Google Scholar]
[18]. Nemade KS, Meshram MM, Kasote AP, Kamdi NY, Arthritis of the subtalar joint associated with sustentaculum tali facet configurationInt J Anat Res 2014 2(4):684-88. [Google Scholar]
[19]. Uygur M, Atamaz F, Celik S, Pinar Y, The types of talar articular facets and morphometric measurements of the calcaneus bone on Turkish raceArch orthop trauma surg 2009 129:909-14. [Google Scholar]
[20]. Campos FF, Pellico LG, Talar articular facets (Facies articulares talares) in human calcaneiActa Anat 1989 134:124-27. [Google Scholar]
[21]. Barbarix E, Roy PV, Clarys JP, Variations of anatomical elements contributing to subtalar joint stability: intrinsic risk factors for post-traumatic lateral instability of the ankleErgonomics 2000 43(10):1718-25. [Google Scholar]
[22]. Ragab A, Stewart SL, Cooperman DR, Implications of subtalar joint anatomic variation in calcaneal lengthening osteotomyJ Paediatr Orthop 2003 23:79-83. [Google Scholar]
[23]. Norkin CC, Joint Structure and Function 1983 PhiladelphiaF. A. Davis [Google Scholar]
[24]. Rose GK, Pes planus. In Disorders of the Foot and Ankle: Medical and Surgical Management. E. H. Wickland Jr 1991 PhiladelphiaW. B. Saunders:892-919. [Google Scholar]
[25]. Smith RW, Computerized sectional imaging: computed tomography and magnetic resonance imaging of the foot and ankleIn Disorders of the Foot and Ankle: Medical and Surgical Management E. H. Wickland Jr 1991 PhiladelphiaW. B. Saunders:155-205. [Google Scholar]
[26]. Greer Richardson E. Pes Planus. In: S Terry Canale, editor. Campbell’s Operative Orthopaedics. 9th ed. St. Louis: Mosby – Year Book, Inc., 1998; pp. 1720-1725 [Google Scholar]
[27]. Perumal A, Anand A, Morphometric study of spur formation in dry adult human calcaneaeInt J Curr Res Rev 2013 5:92-96. [Google Scholar]
[28]. Riepert T, Drechsler T, Urban R, Schild H, Mattern R, The incidence, age dependence and sex distribution of the calcaneal spur. An analysis of its x-ray morphology in 1027 patients of the central European populationRofo 1995 162:502-05. [Google Scholar]
[29]. Kullar JS, Randhawa GK, Kullar KK, A study of calcaneal enthesophytes (spurs) in Indian populationInt J App Basic Med Res 2014 4:S13-16. [Google Scholar]