Introduction
Porphyromonas gingivalis (P.gingivalis) is a notorious perio-pathogen with the ability to evade host defense mechanism and invade into the periodontal tissues. Many antimicrobial agents have been tested that curb its growth, although these agents tend to produce side effects such as antibiotic resistance and opportunistic infections. Therefore search for naturally occurring anti-microbials with lesser side effects is the need of the hour.
Aim
The aim of this study was to substantiate the antimicrobial activity of various essential oils; eucalyptus oil, chamomile oil, tea tree oil and turmeric oil against P. gingivalis.
Materials and Methods
Pure cultures of P. gingivalis were grown on selective blood agar. Antimicrobial efficacy of various concentrations of essential oils (0%, 25%, 50% and 100%) was assessed via disc diffusion test. Zone of inhibition were measured around disc after 48 hours in millimeters.
Results
Zones of inhibition were directly proportional to the concentration of essential oils tested. At 100% concentration all the tested oils possess antimicrobial activity against P.gingivalis with eucalyptus oil being most effective followed by tea tree oil, chamomile oil and turmeric oil.
Conclusion
All essential oils tested were effective against P.gingivalis. After testing for their clinical safety they could be developed into local agents to prevent and treat periodontitis.
Introduction
Periodontitis is an inflammatory disease of the oral cavity of the microbial origin. Host of bacteria have been identified to be associated with it and are termed as ‘periopathogens’ [1]. Of these, one periopathogen that has grabbed the fancy of researchers is Porphyromonas gingivalis. Frequently isolated from active periodontal lesions, it has been positively correlated with progression of periodontal disease [2]. Although a natural member of oral ecology and found in periodontally healthy individuals as well it is highly destructive and attain high numbers in periodontal lesion [3,4]. It has an arsenal of virulence factors which makes it an aggressive ‘pathobiont’ [5,6].
Over the years the basic treatment of periodontitis has remained constant which is the removal of plaque biofilm and calculus from supra and subgingival surfaces through scaling and root planning [7,8]. This treatment aims at removing whole of the biofilm rather than targeting specific periopathogens. However, it has been observed that all the patients might not respond to mechanical debridement only [9]. One of the reasons for this is that some periopathogens including P.gingivalis invade the gingival tissues and are thus spared from mechanical debridement [10]. These hidden pathogens then provide the source for recolonization of periodontal pocket and resurgence of disease. The adjuvant treatment of local drug delivery has been suggested for such tissue invading periopathogens [11].
In local drug delivery, antimicrobial agent is placed within the periodontal pocket in a carrier medium where it is released in to the local area over a period of time [12]. Many anti-microbial agents have been used for this purpose with rather enviable clinical results. Antimicrobial agents that have been used successfully for this purpose include chlorhexidine, tetracycline and metronidazole to name a few [13–15]. But there remains a roadblock in this success march with local delivery of antimicrobials. Previous decades have seen an indiscriminate use of commercial antimicrobials, leading to emergence of multi-drug resistance bacteria [16]. Due to these reasons, natural antimicrobial agents have grabbed attention of researchers. One such group of natural antimicrobial agent that has been used for centuries in naturopathy is the botanically derived essential oils.
Essential oils, also called aromatic plant essences are fragrant volatile substances biosynthesized by plants [17]. The earliest mention of essential oil used for therapeutic purposes is in Ebers papyrus, where more than 800 remedies and treatments have been listed [18]. Since then essential oils have been recognized for their anti-inflammatory, anti-microbial and anti-oxidant properties. The oxygenated terpenoids and some hydrocarbons found in essential oils account for most of their anti-microbial activity [19]. Research suggests that terpenoids diffuse within the cell membrane, irreversibly damaging it and causing bacterial cell death. Being lipophillic in nature, these terpenes causes expansion of membrane, increases its fluidity and inactivates the enzymes embedded within the membrane [20,21].
Although there is a revival of interest in essential oils and their anti microbial properties, the data regarding the efficacy of these oils against oral bacteria especially periopathogens is limited. Here in this study, we assessed the antimicrobial efficacy of above mentioned essential oils at varying concentrations against a major periopathogen P.gingivalis.
Materials and Methods
This in-vitro microbiological study was carried out in Department of Periodontology, Faculty of Dental Sciences, SGT University in association with Department of Microbiology, Faculty of Medical and Health Sciences, SGT University, Gurgaon, Delhi-NCR. The P.gingivalis colonies used in this study were cultivated from the subgingival plaque samples obtained from the Chronic Periodontitis patients reporting to the OPD of the Department of Periodontology. The study commenced in September 2015 and was completed within two weeks of initiation.
Collection of subgingival plaque samples: Five patients with untreated generalized chronic periodontitis were selected for collection of subgingival plaque samples. The patients selected had at least four sites with probing pocket depth of 6 mm or more. To collect the subgingival samples, sterile paper points were used. The area was isolated using cotton rolls and any supragingival plaque and calculus hindering the insertion of paper point into the periodontal pockets was removed using sterile supragingival scalers. Sterile paper points were then inserted slowly with the help of a sterile dental tweezer into the pocket until tissue resistance. Paper point was left in place for around 60 seconds, carefully removed and immediately placed into a sterile container with anaerobic transport media and sent for microbiology department for culture.
P.gingivalis culture on selective media: The composition of selective media per 1000 ml was as follows: Columbia agar (42.5%), Agar (6.5g), 0.1% solution of Hemin (5.0ml), 1% solution of vitamin K1 (1.0 ml), Human blood (50ml), Colistinmethanesulfonate (15.37 mg), Bacitracin (10mg), Nalidixic acid (15 mg) and distilled water. Media was prepared and stored under strict anaerobic conditions to prevent oxidation. Subgingival samples obtained were directly inoculated onto selective media plates for P.gingivalis. The inoculated plates were then incubated anaerobically at 37oC for 48 hours. Colonies of P.gingivalis developed after 48hours which were round, opaque and convex with 1-2mm diameter. Since whole blood was used the black pigment did not appear at 48 hours since appearance of pigment is slow in non lysed blood.
Confirmation of P. gingivalis growth: Since a media selective for P.gingivalis was used, only few tests to confirm the presence of desired bacteria were done. The colonies were tested for their ability to fluoresce under ultraviolet light. The colonies were dispersed in 1.0 ml of 96% aqueous ethanol and the suspension was illuminated in a dark room with a 366nm ultra violet light. The colonies failed to produce a red fluorescence which was taken as positive for P.gingivalis growth. Further the colonies were tested for their ability to hydrolyse synthetic trypsin substrate N-Benzoyl-DL-Arginine-2-Naphthylamide (BANA). A sterile paper saturated with BANA was taken and colonies were placed over it for 30minutes. This strip was then placed over a filter paper saturated with fast blue BB salt (0.35% w/v in methoxyethanol). The colonies gave a positive reaction with appearance of orange red colour. Both of these test confirmed the colonies to be of P.gingivalis.
Preparation of various concentrations of essential oils: Four essential oils; Eucalyptus, Tea-tree, Chamomile and Tur meric oil were tested for their efficacy against P.gingivalis. All the essential oils were obtained from Farmaessentials®, Chandigarh, India. All were tested in four concentrations for their antibacterial activity: 0%, 25%, 50% and 100%. The essential oils were diluted in vegetable oil which in itself lacked antimicrobial activity. This was confirmed with the inclusion of 0% group in the study which contained only vegetable oil and no essential oil. Twenty five percent concentrations were prepared by adding 1.25 ml of essential oil in 5ml of vegetable oil. Likewise 50% concentration had 2.5 ml of essential oil in 5 ml of vegetable oil where as 100% concentration had only pure essential oil but no vegetable oil. The dilutions were prepared just before the paper disc diffusion test was initiated.
Paper disc diffusion test: Paper disc diffusion was carried out on selective blood agar plates. The P.gingivalis culture was aseptically spread on surface of agar plate. Sterilized small filter paper disc with 6 mm diameter were used for the study. The discs impregnated with essential oils were placed on the agar surface. Ten discs of each concentration of each essential oil were taken for the experiment. The agar plates were incubated at 37oC for 48 hours under strict anaerobic conditions. The antibiotic activity of various concentrations of essential oil was assessed by measuring the diameter of the growth inhibition zone in millimeters. All the data was collected and assessed with SPSS 19.0 software for statistical analysis. Both intra group and intergroup comparisons was carried out using student’s t-test.
Results
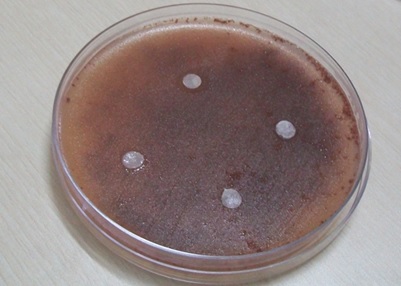
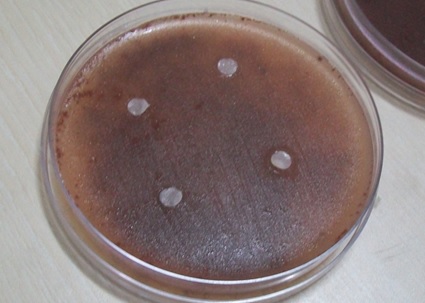
The zone of inhibition obtained for varying concentrations of four essential oils included in the study are compiled in [Table/Fig-1]. The zones of inhibition around paper discs infused with these essential oils are depicted in [Table/Fig-2,3,4 and 5]. Since ten discs were used for each concentration, the zones of inhibition were calculated as a mean of all ten values. The zone of inhibition was directly proportional to concentration of essential oil tested. No zone of inhibition was observed around zero percent disc confirming the carrier medium was inert with no antibacterial activity of its own. Turmeric oil had least activity against P.gingivalis, whereas eucalyptus oil had maximum. On intragroup comparison [Table/Fig-6] of varying concentration of essential oils, there was significant difference between 25% and 50% concentration of eucalyptus and chamomile essential oils (p<0.001). While comparing the difference in antibacterial activity of 50% and 100% concentrations, all the oils tested had highly significant results (p<0.001). On intergroup comparison [Table/Fig-7], there was highly significant difference in antibacterial activity of 100% concentration of all essential oils tested against P.gingivalis. The antibacterial activity of these oils was in following order: eucalyptus oil, chamomile oil, tea tree oil followed by turmeric oil.
Zone of inhibition of various concentrations of essential oils.
| Essential oil | Concentration (%) | Zone of inhibition (mm) ± S.D |
|---|
| Eucalyptus Oil | 0 | 0 |
| 25 | 1.70 ± 0.258 |
| 50 | 2.51 ± 0.213 |
| 100 | 4.5 ± 0.183 |
| Chamomile Oil | 0 | 0 |
| 25 | 0.52 ± 0.199 |
| 50 | 1 ± 0.2 |
| 100 | 1.7 ± 0.183 |
| Turmeric Oil | 0 | 0 |
| 25 | 0 |
| 50 | 0.5 ± 0.082 |
| 100 | 1.12 ± 0.079 |
| Tea tree Oil | 0 | 0 |
| 25 | 0 |
| 50 | 0.98 ± 0.092 |
| 100 | 2.9 ± 0.356 |
Zone of inhibition around eucalyptus essential oils discs against P.gingivalis.

Zone of inhibition around chamomile essential oils discs against P.gingivalis.
Zone of inhibition around tea tree essential oils discs against P.gingivalis.

Zone of inhibition around turmeric essential oils discs against P.gingivalis.
Intragroup comparison of various concentrations of essential oils.
| Essential oil | 25% v/s 50% | 50% v/s 100% |
|---|
| 95% CI | p- value | 95% CI | p-value |
|---|
| Eucalyptus Oil | 1.032-0.588 | <0.001 | 2.176-1.804 | <0.001 |
| Chamomile Oil | 0.667-0.293 | <0.001 | 0.880-0.520 | <0.001 |
| Turmeric Oil | - | - | 0.695-0.545 | <0.001 |
| Tea tree Oil | - | - | 2.164-1.676 | <0.001 |
p<0.001 is highly significant [data was analysed using t-test]
Intergroup comparison of 100% concentration of essential oil.
| Essential oil | Chamomile Oil | Turmeric Oil | Tea tree Oil |
|---|
| 95% CI | p- value | 95% CI | p-value | 95% CI | p-value |
|---|
| Eucalyptus Oil | 2.628-2.972 | <0.001 | 1.334-1.866 | <0.001 | 1.334-1.866 | <0.001 |
| Chamomile Oil | - | - | 0.448-0.712 | <0.001 | 1.466-0.934 | <0.001 |
| Turmeric Oil | - | - | - | - | 1.538-2.022 | <0.001 |
p<0.001 is highly significant (data was analysed using t-test)
Discussion
Several naturally and synthetically derived agents are being used in dentistry to inhibit the disease causing plaque biofilm these agents include cetylpyridinium chloride and other antimicrobials such as doxycycline, minocycline and metronidazole. These have been used successfully as a mouthwash, topically applied gels or intrapocket local drug delivery agents. These modalities have shown promising results as an adjunct to standard therapy of scaling and root planing [22–24]. The dental community is in search of newer therapeutic agents that apart from having a positive impact on periodontal health will lack the usual side effects of in use antimicrobials. Phytochemicals such as essential oils provide such an alternative.
We tested four essential oils in varying concentrations against the notorious periopathogen P.gingivalis. Our data revealed that all four essential oils tested, that is eucalyptus oil, chamomile oil, turmeric oil and tea tree oil had antimicrobial activity against P.gingivalis where eucalyptus oil had maximum efficacy and turmeric oil the least. Also, tea tree oil and turmeric oil lacked any antibacterial activity against P.gingivalis at 25% concentration. As the concentration of each oil increased, the antibacterial efficacy improved. An interesting observation though is higher antibacterial effect of tea tree oil than chamomile oil at 50% and 100% concentration whereas at 25% concentration chamomile oil was more efficacious. This indicates that certain essential oils such as tea tree oil work better at higher concentrations.
Eucalyptus, genus of family Myrtaceae has been used to control infectious diseases since the time of ancient Egyptians [25]. Antimicrobial, anti-inflammatory as well as analgesic properties of eucalyptus essential oil have been reported [26,27]. Its predominant component is Citronellal (57%) followed by citronellol (16%) and citronellyl acetate (15%) [28]. However, the antimicrobial bioactivity can be attributed to α- terpineol which showed eight fold higher activity than citronellol against Staphyllococcu saureus [29]. Eucalyptus oil inhibited the growth of periodontopathogens including P.gingivalis and the minimum inhibitory concentration ranged from 0.25% to 0.5% for various strains [30].
Matricariarecutita, commonly called chamomile belongs to the family Asteraceae. As believed by Anglo-saxons, chamomile is one of the nine sacred herbs given by Lord to humans [31]. Chamomile flowers contain a blue colour volatile oil, of which around 120 constituents have been identified [32]. Major constituent is a terpenoid, α-bisabolol and its oxides which form around 78% of composition. Other constituents which form around 1-15% of composition are azulenes which include chamazulene [33]. The antimicrobial activity of chamomile oil has been confirmed against S. aureus and Candida strains [34]. There is limited research on the antibacterial effect of chamomile essential oil against common oral pathogens. During the search of literature on chamomile oil we could not find much data on its antimicrobial or antibacterial activity. It is therefore to our knowledge first data on antibacterial effect of chamomile oil against any periopathogen.
Tea tree oil is extracted via steam distillation of leaves and twigs of tree Melaleucaalternifolia. It has been used widely for the treatment of cold, cough, sore throats and skin diseases [35]. The anti-microbial activity of this essential oil could be attributed to terpinen-4-ol [36]. Research has demonstrated its ability to inhibit cellular respiration in Eschercia coli by disrupting the permeability barrier of bacterial cell membrane [37]. Similar to our study, it has been found to have significant antibacterial activity against four common intra canal oral pathogens [38]. Tea tree oil also shows significant adhesion-inhibiting activity against P. gingivalis [30].
Curcuma longa, commonly termed turmeric is a botanical relative of family Zingiberaceae [39]. It’s a commonly used spice along with vast history of use as a therapeutic agent. The extract of turmeric is an oleoresin which has two fractions: a yellow brown heavy fraction and a light volatile oil fraction. The extract as a whole consists of many curcuminoids, monoterpenoids and sesquiterpenoids [40]. Curcumin is the principle curcuminoid responsible for antioxidant, anti-inflammatory and antimicrobial activity of turmeric [41]. The major component of turmeric essential oil is aromatic tumerone (20-30%) [42]. Although used as a mosquito repellent and in treatment of respiratory diseases, its antibacterial and antifungal activity has also been identified [43–46]. Research on its effect against periopathogens is lacking but still it has been used clinically as a mouthwash, local drug delivery agent as well as subgingival irrigant [47–49].
There are increasing numbers of research paper on the antimicrobial efficacy of various essential oils for their prospective use as surface disinfectants, food preservatives and alternative medicinal therapy. However articles on their antibacterial efficacy against oral pathogens especially periopathogens are limited. Takarada et al., assessed the antimicrobial effect of essential oils on cariogenic and periodontopathic bacteria including P.gingivalis [30]. They found that periodontopathic bacteria were killed completely by exposure for 30 seconds to 0.2% manuka oil, tea tree oil and eucalyptus oil. Tea tree and manuka oil showed significant adhesion inhibiting activity against P.gingivalis [27]. These results are in accordance with our study. Among all the oils tested, manuka and tea tree oil had particular strong antibacterial activity against periodontopathic bacteria. In our study, we found eucylyptus oil to be more effective than tea tree oil against P.gingivalis.
Since periodontitis is highly prevalent disease, undesirable effects of several antimicroial agents presently being used in treatment of oral disease and augmented resistance of oral bacteria to antibiotics are a cause of concern. Alternate products that are safe but equally effective are required for the treatment as well as the prevention of disease. Essential oils such as those tested in this study could provide a good alternative to usual commercial antibiotics.
Limitation
There are certain limitations of the study that we carried out. First, only one periopathogen P.gingivalis was tested for antibacterial efficacy of these essential oils. The reason is fastidious growth condition required for growth of these anaerobic periopathogens. Another drawback is that minimum inhibitory concentrations of these essential oils were not determined. The results of our study indicate their potential use in oral cavity especially intrapocket placement which is the ecological niche of P.gingivalis. Our follow- up research will be on their safety and cell toxicity at various concentrations. Establishing the safety of these oils intraorally will pave the path for their full scale use as a local drug delivery agent for the treatment of periodontitis.
Conclusion
To conclude both eucalyptus and tea tree oil possess a significant antibacterial activity against P.gingivalis followed by chamomile and turmeric oil. Also as the concentration of essential oils increases so does the antibacterial efficacy.
p<0.001 is highly significant [data was analysed using t-test]
p<0.001 is highly significant (data was analysed using t-test)
[1]. Flemmig TF, PeriodontitisAnn Periodontol 1999 4:32-37. [Google Scholar]
[2]. Pihlstrom BL, Periodontal risk assessment, diagnosis and treatment planningPeriodontol 2000 2001 25:37-58. [Google Scholar]
[3]. Hajishengallis G, Porphyromonas gingivalis-host interactions: open war or intelligent guerilla tactics?Microbes Infect 2009 11:637-45. [Google Scholar]
[4]. Slots J, Update on Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis in human periodontal diseaseJ Int Acad Periodontol 1999 1:121-26. [Google Scholar]
[5]. O-Brien-Simpson NM, Veith PD, Dashper SG, Reynolds EC, Porphyromonas gingivalis gingipains: the molecular teeth of a microbial vampireCurr Protein Pept Sci 2003 4:409-26. [Google Scholar]
[6]. Bostanci N, Belibasakis GN, Porphyromonas gingivalis: an invasive and evasive opportunistic oral pathogenFEMS Microbiol Lett 2012 333:1-9. [Google Scholar]
[7]. Smiley CJ, Tracy SL, Abt E, Michalowicz BS, John MT, Gunsolley J, Systematic review and meta-analysis on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjunctsJ Am Dent Assoc 2015 146:508-24. [Google Scholar]
[8]. Drisko CL, Periodontal debridement: still the treatment of choiceJ Evid Based Dent Pract 2014 14(Suppl):33-41. [Google Scholar]
[9]. Haffajee AD, Dibart S, Kent RL Jr, Socransky SS, Factors associated with different responses to periodontal therapyJ Clin Periodontol 1995 22:628-36. [Google Scholar]
[10]. Amano A, Disruption of epithelial barrier and impairment of cellular function by Porphyromonas gingivalisFront Biosci 2007 12:3965-74. [Google Scholar]
[11]. Page RC, The microbiological case for adjunctive therapy for periodontitisJ Int Acad Periodontol 2004 6(Suppl):143-49. [Google Scholar]
[12]. Etienne D, Locally delivered antimicrobials for the treatment of chronic periodontitisOral Dis 2003 9(Suppl):45-50. [Google Scholar]
[13]. Medaiah S, Srinivas M, Melath A, Girish S, Polepalle T, Dasari AB, Chlorhexidine chip in the treatment of chronic periodontitis - a clinical studyJ Clin Diagn Res 2014 8:22-25. [Google Scholar]
[14]. Aimetti M, Romano F, Torta I, Cirillo D, Caposio P, Romagnoli R, Debridement and local application of tetracycline-loaded fibres in the management of persistent periodontitis: results after 12 monthsJ Clin Periodontol 2004 31:166-72. [Google Scholar]
[15]. Paul TP, Emmatty R, Pulikkottil JJ, Rahman AA, Kumar SA, George N, Comparative evaluation of sustained release collagen device containing 5% metronidazole (metrogene) along with and without scaling and root planing at regular intervals with treatment of chronic periodontitis: a case control studyJ Int Oral Health 2015 7:18-22. [Google Scholar]
[16]. Pogue JM, Kaye KS, Cohen DA, Marchaim D, Appropriate antimicrobial therapy in the era of multidrug-resistant human pathogensClin Microbiol Infect 2015 21:302-12. [Google Scholar]
[17]. Bassolé IH, Juliani HR, Essential oils in combination and their antimicrobial propertiesMolecules 2012 17:3989-4006. [Google Scholar]
[18]. Vigan M, Essential oils: renewal of interest and toxicityEur J Dermatol 2010 20:685-92. [Google Scholar]
[19]. Bhatti HN, Khan SS, Khan A, Rani M, Ahmad VU, Choudhary MI, Biotransformation of monoterpenoids and their antimicrobial activitiesPhytomedicine 2014 21:1597-626. [Google Scholar]
[20]. Andrews RE, Parks LW, Spence KD, Some effects of douglas fir terpenes on certain microorganismsAppl Environ Microbiol 1980 40:301-14. [Google Scholar]
[21]. Sikkema J, de Bont JA, Poolman B, Mechanisms of membrane toxicity of hydrocarbonsMicrobiol Rev 1995 59:201-22. [Google Scholar]
[22]. Elias-Boneta AR, Toro MJ, Noboa J, Romeu FL, Mateo LR, Ahmed R, Efficacy of CPC and essential oils mouthwashes compared to a negative control mouthwash in controlling established dental plaque and gingivitis: A 6-week, randomized clinical trialAm J Dent 2015 28:21A-6A. [Google Scholar]
[23]. Bergamaschi CC, Santamaria MP, Berto LA, Cogo-Müller K, Motta RH, Salum EA, Full mouth periodontal debridement with or without adjunctive metronidazole gel in smoking patients with chronic periodontitis: A pilot studyJ Periodontal Res 2016 51:50-59. [Google Scholar]
[24]. Matesanz-Pérez P, García-Gargallo M, Figuero E, Bascones-Martínez A, Sanz M, Herrera D, A systematic review on the effects of local antimicrobials as adjuncts to subgingival debridement, compared with subgingival debridement alone, in the treatment of chronic periodontitisJ Clin Periodontol 2013 40:227-41. [Google Scholar]
[25]. Luqman S, Dwivedi GR, Darokar MP, Kalra A, Khanuja SPS, Antimicrobial activity of Eucalyptus citriodora essential oilInternational Journal of Essential Oil Therapeutics 2008 2:69-75. [Google Scholar]
[26]. Cimanga K, Kambu K, Tona L, Apers S, De Bruyne T, Hermans N, Correlation between chemical composition and antibacterial activity of essential oils of some aromatic medicinal plants growing in the Democratic Republic of CongoJ Ethnopharmacol 2002 79:213-20. [Google Scholar]
[27]. Silva J, Abebe W, Sousa SM, Duarte VG, Machado MI, Matos FJ, Analgesic and anti-inflammatory effects of essential oils of EucalyptusJ Ethnopharmacol 2003 89:277-83. [Google Scholar]
[28]. Tian Y, Liu X, Zhou Y, Guo Z, Extraction and determination of volatile constituents in leaves of Eucalyptus citriodoraChinese J Chromatography 2005 23:651-54. [Google Scholar]
[29]. Inouye S, Takizawa T, Yamaguchi H, Antibacterial activity of essential oils and their major constituents against respiratory tract pathogens by gaseous contactJ Antimicrob Chemother 2001 47:565-73. [Google Scholar]
[30]. Takarada K, Kimizuka R, Takahashi N, Honma K, Okuda K, Kato T, A comparison of the antibacterial efficacies of essential oils against oral pathogensOral MicrobiolImmunol 2004 19:61-64. [Google Scholar]
[31]. Singh O, Khanam Z, Misra N, Srivastava MK, Chamomile (Matricariachamomilla L.): an overviewPharmacogn Rev 2011 5:82-95. [Google Scholar]
[32]. Pino JA, Bayat F, Marbot R, Aguero J, Essential oil of chamomile. Chamomillarecutita (L.) Rausch from IranJournal of Essential Oil Research 2002 14:407-08. [Google Scholar]
[33]. Matos FJA, Machado MIL, Alencar JW, Craveiro AA, Constituents of Brazilian chamomile oilJournal of Essential Oil Research 1993 5:337-39. [Google Scholar]
[34]. Nogueira JC, DinizMde F, Lima EO, In vitro antimicrobial activity of plants in Acute Otitis ExternaBraz J Otorhinolaryngol 2008 74:118-24. [Google Scholar]
[35]. Carson CF, Hammer KA, Riley TV, Melaleucaalternifolia (Tea Tree) oil: a review of antimicrobial and other medicinal propertiesClin Microbiol Rev 2006 19:50-62. [Google Scholar]
[36]. Carson CF, Riley TV, Antimicrobial activity of the major components of the essential oil of MelaleucaalternifoliaJ Appl Bacteriol 1995 78:264-69. [Google Scholar]
[37]. Cox SD, Gustafson JE, Mann CM, Markham JL, Liew YC, Hartland RP, Tea tree oil causes K+ leakage and inhibits respiration in Escherichia coliLett Appl Microbiol 1998 26:355-58. [Google Scholar]
[38]. Thosar N, Basak S, Bahadure RN, Rajurkar M, Antimicrobial efficacy of five essential oils against oral pathogens: An in vitro studyEur J Dent 2013 7(Suppl 1):S71-S77. [Google Scholar]
[39]. Chattopadhyay I, Biswas K, Bandyopadhyay U, Banerje RK, Turmeric and curcumin: Biological actions and medicinal applicationsCurrent science 2004 87:44-53. [Google Scholar]
[40]. Gul P, Bakht J, Antimicrobial activity of turmeric extract and its potential use in food industryJ Food Sci Technol 2015 52:2272-79. [Google Scholar]
[41]. Menon VP, Sudheer AR, Antioxidant and anti-inflammatory properties of curcuminAdv Exp Med Biol 2007 595:105-25. [Google Scholar]
[42]. Govindarajan VS, Turmeric-chemistry, technology, and qualityCrit Rev Food Sci Nutr 1980 12:199-301. [Google Scholar]
[43]. Tawatsin A, Wratten SD, Scott RR, Thavara U, Techadamrongsin Y, Repellency of volatile oils from plants against three mosquito vectorsJ Vector Ecol 2001 26:76-82. [Google Scholar]
[44]. Li C, Li L, Luo J, Huang N, Effect of turmeric volatile oil on the respiratory tractZhongguo Zhong Yao Za Zhi 1998 23:624-25. [Google Scholar]
[45]. Negi PS, Jayaprakasha GK, Jagan Mohan Rao L, Sakariah KK, Antibacterial activity of turmeric oil: a byproduct from curcumin manufactureJ Agric Food Chem 1999 47:4297-300. [Google Scholar]
[46]. Jayaprakasha GK, Negi PS, Anandharamakrishnan C, Sakariah KK, Chemical composition of turmeric oil—a byproduct from turmeric oleoresin industry and its inhibitory activity against different fungiZ Naturforsch C 2001 56:40-44. [Google Scholar]
[47]. Waghmare PF, Chaudhari AU, Karhadkar VM, Jamkhande AS, Comparative evaluation of turmeric and chlorhexidine gluconate mouthwash in prevention of plaque formation and gingivitis: a clinical and microbiological studyJ Contemp Dent Pract 2011 12:221-24. [Google Scholar]
[48]. Behal R, Mali AM, Gilda SS, Paradkar AR, Evaluation of local drug-delivery system containing 2% whole turmeric gel used as an adjunct to scaling and root planing in chronic periodontitis: A clinical and microbiological studyJ Indian Soc Periodontol 2011 15:35-38. [Google Scholar]
[49]. Nagpal M, Sood S, Role of curcumin in systemic and oral health: An overviewJ Nat Sci Biol Med 2013 4:3-7. [Google Scholar]