Fistular Opening below the Intertragric Notch: A Rare Variant of Pre-Auricular Sinus
Rakhi Kumari1, Rajiv Kumar Jain2, Priyanko Chakraborty3, Sidharth Pradhan4, Purnima Joshi5
1 Junior Resident, Department of ENT, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
2 Professor and Head, Department of ENT, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
3 Resident, Department of ENT, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
4 Resident, Department of ENT, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
5 Resident, Department of ENT, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rakhi Kumari, Junior Resident, Department of ENT, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005, Uttar Pradesh, India.
E-mail: dr.rakhi.kumari@gmail.com
Preauricular sinus, Intertragic notch, postauricular sinus
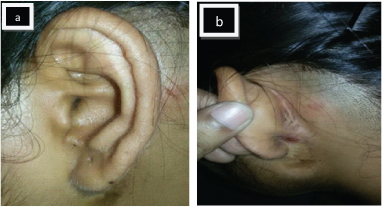
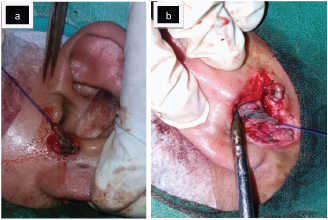
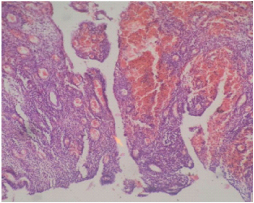
A 22-year-old female presented in the Department of Otorhinolaryngology, Institute of Medical Sciences, BHU, Varanasi with complaints of recurrent painful swelling, itching and discharge from left postauricular area for ten years, for which she was operated five year back and the swelling was excised. But her symptoms persisted after surgery. She had history of incision and drainage twice in the left ear after that. On careful examination a sinus opening was found just below the intertragic notch since birth. Scar mark of previous incision and scarring present in postauricular area [Table/Fig-1a,b]. During the surgery, local anaesthesia was given around sinus opening located below intertragic notch and in retroauricular area. Methylene blue dye was injected in the sinus tract. An elliptical incision was made around sinus tract and in retroauricular area and the sinus tract was dissected from surrounding structure under visual guidance. On tracing the sinus tract, the sinus tract was seen to be passing through the conchal cartilage [Table/Fig-2a,b]. Hence, a piece of conchal cartilage was excised along with the tract and the sample was sent for histopathological examination. The sinus tract was not related to parotid tissue and facial nerve. Histopathology confirmed that the excised tissue was a sinus tract lined with squamous epithelium [Table/Fig-3]. The patient was followed up for six months and no any further complains were reported.
Clinical photograph of patient showing: a) fistula opening just below intertragic notch; b) Post auricular scarring.
Intraoperative photograph of patient showing the excised tract along with the opening just below intertragic notch.
Histopathological picture showing sinus tract lined by inflammatory granulation tissue.
Discussion
The development of pinna begins during the fourth week of gestation and adult configuration is achieved at approximately five months. Developmental process of pinna is independent of development in middle and inner ear. Pinna develops from six mesenchymal proliferations, known as the hillocks of His; three from the first branchial arch and three from the second branchial arch [1]. Defective fusion of the hillocks of His during development of pinna leads to formation of preauricular sinus [2]. Preauricular sinus is an occasional finding found during examination of ear as a small pit close to the anterior margin of the ascending portion of the helix or in front of tragus [3].
Choi et al., divided the sinuses into two type depending up on the relation of the sinus opening with extended tragal line -a perpendicular line passing posterior to the tragus and ascending limb of the helix. Sinus was classified as preauricular or postauricular depending upon location of sinus opening in front of or behind the extended tragal line [4].
In preauricular sinus the most common site of fistula opening is anterior to ascending crux of helix or just in front of tragus with sinus tract lies anterior to ascending crux of helix and in majority of cases attached to its perichondrium. In postauricular sinus, the most common site of fistula opening is at the root of helix with the sinus tract directed towards the posterior or postero-inferior portion of the pinna. Sinus tract of postauricular sinus passes through auricular cartilage.
In the present case, a sinus opening was present just below the intertragic notch. On tracing the sinus tract, the sinus tract was seen to be passing through the conchal cartilage. So, we procceded by giving an elliptical incision around the sinus tract and in retroauricular area. The sinus tract was dissected from surrounding structure and it was confirmed by histopathological findings also.
Work classified first brachial cleft anomaly in two type: type I and type II [5]. Sinus tract of type I first brachial cleft anomaly ends in bony meatus without any external opening and closely related to inferior division of facial nerve and parotid tissue [6]. External opening formed only after sinus tract becomes infected, whereas sinus opening of type II first brachial cleft anomaly generally located in upper part of neck with sinus tract closely related to parotid tissue and facial nerve [7]. In the present case sinus opening was present since birth and sinus tract was not related to parotid tissue and facial nerve. So we suggest it was not a variant of brachial cleft anomaly. Sinogram may be ordered to find out length, branching and depth of sinus tract but the actual differentiation from branchial arch anomalies lies in the knowledge of the regional embryology and peroperative findings [8].
Preauricular sinus generally remains asymptomatic and was found during examination of ear as an incidental finding. When it remains asymptomatic it does not require any treatment. Symptoms appear when it gets infected. Infection of preauricular sinus leads to recurrent discharge, pain, itching, swelling around pinna and abscess formation. The most common pathogens causing infection of preauricular sinuses are Staphylococcal species followed by Proteus,Streptococcus and Peptococcus species [9]. Once infected, excision of sinus tract becomes necessary. Sinus opening away from post auricular swelling in post auricular sinus is frequently misdiagnosed. In postauricular sinus, the sinus opening is located in the center of the crus of helix, or its surrounding; and the sinus tract passes through the cartilage. Therefore, the portion of auricle cartilage needs to be removed; along with the sinus tract and removal via anterior-posterior approach of the auricle is necessary to completely remove the postauricular sinus [10]. In case of periauricular swelling and discharge careful search of sinus opening in and around auricle is necessary to avoid misdiagnosis of these rare findings. The significance of our case was the rare location of fistula opening just below the intertragic notch on the earlobe.
[1]. Sadler TW, Langman’s Medical Embryology 1990 6th ednBaltimoreWilliams & Wilkins:334-35. [Google Scholar]
[2]. Chowdary VS, Chandra NS, Madesh RK, Preauricular sinus: A novel approachKavuturu Indian J Otolaryngol Head Neck Surg 2013 65(3):234-36. [Google Scholar]
[3]. Chami RG, Apesos J, Treatment of asymptomatic preauricular sinuses: challenging conventional wisdomAnn Plast Surg 1989 23:406-11. [Google Scholar]
[4]. Choi SJ, Choung YH, Park K, Bae J, Park HY, The variant type of preauricular sinus: postauricular sinusLaryngoscope 2007 117:1798-802. [Google Scholar]
[5]. Coppens F, Peene P, Lemahieu SF, Diagnosis and differential diagnosis of branchial cleft cysts by CT scanJournal Belge de Radiologie 1990 73(3):189-96. [Google Scholar]
[6]. Work WP, Newer concepts of first branchial cleft defectsLaryngoscope 1972 82(9):1581-93. [Google Scholar]
[7]. Prasad SC, Azeez A, Thada ND, Rao P, Bacciu A, Prasad KC, Branchial anomalies: diagnosis and managementHindawi Publishing Corporation International Journal of OtolaryngologyVolume 2014http://dx.doi.org/10.1155/2014/237015 [Google Scholar]
[8]. Dutta M, Ghatak S, Sarkar R, Of peri-auricular pits and sinuses: understanding the masqueradersEinstein 2014 12(1):132-33. [Google Scholar]
[9]. Scheinfeld NS, Silverberg NB, Weinberg JM, Nozad V, Preauricular sinus: a review of its clinical presentation, treatment, and associationsPediatr Dermatol 2004 21:191-96. [Google Scholar]
[10]. Kim HJ, Lee JH, Cho HS, Moon IS, A case of bilateral postauricular sinusesKorean J Audiol 2012 16:99-101. [Google Scholar]