Exostosis Bursata – Multimodality Imaging Approach
Asik Ali Mohamed Ali1, Praveen Sharma2, Rujuta Rege3, CR Seena4, Saveetha Rajesh5
1 Assistant Professor, Department of Radiology and Imaging Sciences, Saveetha Medical College Hospital, Chennai, Tamil Nadu, India; Clinical Fellow, Cardiothroacic Imaging, Vancouver General Hospital, Vancouver, Canada.
2 Assistant Professor, Department of Radiology and Imaging Sciences, Saveetha Medical College Hospital, Chennai, Tamil Nadu, India.
3 Resident, Department of Radiology and Imaging Sciences, Saveetha Medical College Hospital, Chennai, Tamil Nadu, India.
4 Professor, Department of Radiology and Imaging Sciences, Saveetha Medical College Hospital, Chennai, Tamil Nadu, India.
5 Professor, Department of Radiology and Imaging Sciences, Saveetha Medical College Hospital, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Asik Ali Mohamed Ali, 16 New 33 Gandhi Road, Gill Nagar Extn., Choolaimedu, Chennai - 600094, Tamil Nadu, India.
E-mail: asik1144@gmail.com
Osteochondromas or exostosis are common benign bone tumours, commonly arising from the metaphyseal region of long bones (femur, humerus, tibia). Osteochondroma of the scapula are rare and cause mechanical irritation leading to bursal formation. We hereby report a case of 30-year-old man who presented with painful chest wall swelling and its multimodality approach to establish the diagnosis.
Bone tumour, Bursae, Osteochondroma
Case Report
A 30-year-old man presented with swelling on posterior right chest wall. Swelling was tender and progressively increased to present size in one year. There was no suspicious trauma, surgical or medical history. Physical examination demonstrated 20x10 cm soft, compressible swelling along the lateral border of the right scapula. There was no restriction in the range of motion of right shoulder. Haematological investigations were within normal limits. Computed Tomography (CT) and three dimensional volume rendered image demonstrated pedunculated bony outgrowth in the inferior and ventral aspect of the right scapula with fluid accumulation in the bursa, manifesting as 3x15 cm enlarging mass between the serratus anterior muscle and thoracic cage [Table/Fig-1,2,3 and 4]. Magnetic Resonance Imaging (MRI) showed bony outgrowth with cartilage cap of thickness 1.5 mm and bursal fluid accumulation with few haemorrhagic areas [Table/Fig-5,6 and 7]. Under ultrasound guidance, 100 ml of sero-sanguineous fluid was aspirated [Table/Fig-8]. Cytological evaluation of the aspirate showed red blood cells, macrophages and inflammatory cells, suggestive of inflammation. Preoperative diagnosis of osteochondroma with bursal fluid accumulation was made. The patient underwent surgical excision successfully and the diagnosis was confirmed by histopathology.
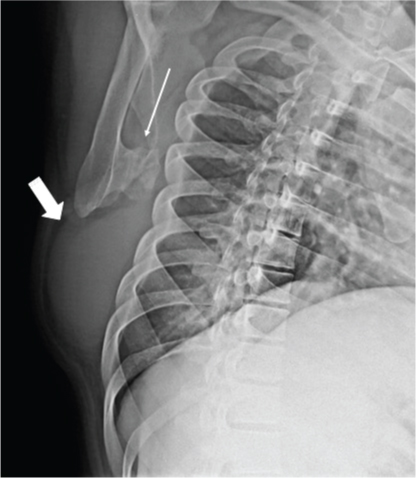
Oblique view of the scapula showing bony outgrowth (arrow) arising from the ventral and inferior aspect of the scapula facing towards the chest wall with bursa inferior to the scapula (bold arrow).
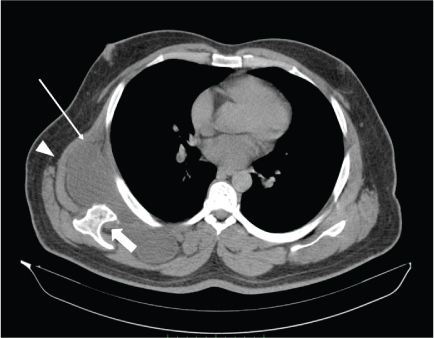
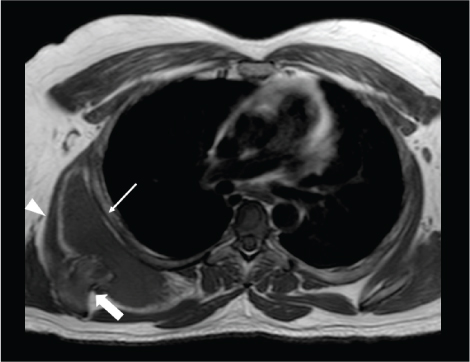
CT axial section of thorax shows Osteochondroma (bold arrow) causing bursal fluid accumulation (arrow) between the serratus anterior muscle (arrowhead) and chest wall.
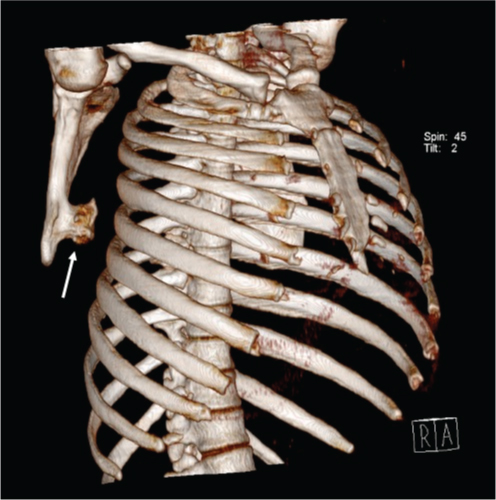
CT three dimensional volume rendered image showing bony lesion (obliquely rotated) arising from the ventral aspect of the right scapula (arrow).
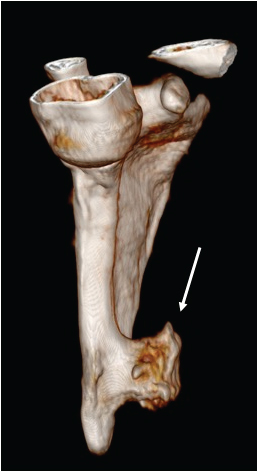
CT three dimensional volume rendered image of right scapula (cropped) showing bony lesion arising from the ventral aspect of the right scapula (arrow).
T1 weighted image shows bony outgrowth from the ventral surface of the scapula (bold arrow) hypointense collection between the serratus anterior muscle (arrowhead) and chest wall (arrow) with few hyperintensities within.
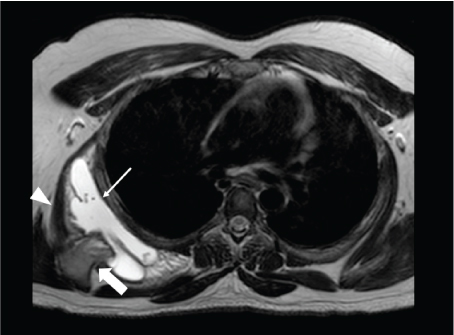
T2 weighted image shows bony outgrowth from the ventral surface of the scapula (bold arrow) with hyperintense collection between the serratus anterior muscle (arrowhead) and chest wall (arrow) with few hypointensities within. Cartilage cap measures 2.2 mm.
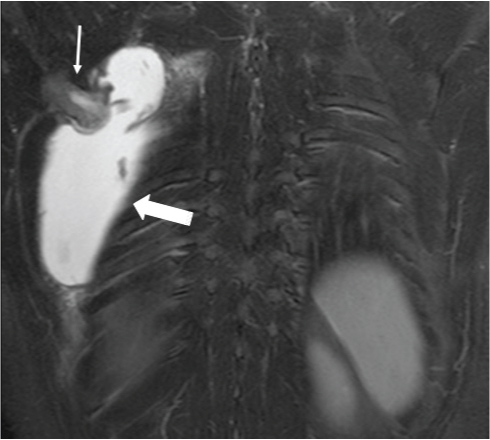
STIR (short tau inversion recovery) coronal images shows Osteochondroma (arrow) with cartilage cap and bursal fluid collection (bold arrow).
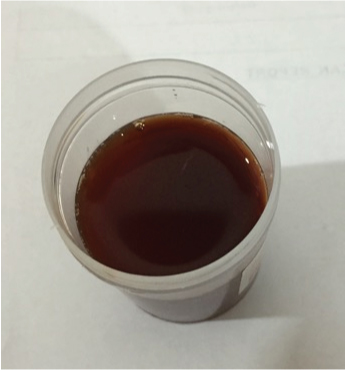
Ultrasound guided aspiration of the bursa revealed serosangenious fluid.
Discussion
Osteochondroma is the most common benign tumour of bone, which are developmental lesions rather than true neoplasm and are called osteocartilaginous exostosis or exostosis [1]. Pathologically, they develop due to detachment of a fragment of epiphyseal growth plate cartilage, which eventually herniates through the periosteal bone surrounding the growth plate. Repeated growth of this fragment and its ensuing enchondral ossification results in sub-periosteal osseous outgrowth with a cartilage cap that projects from the bone surface [2]. True osteochondroma exhibit direct continuity with the underlying cortex and medulla. The commonest site are long bones of the extremity with unusual locations being small bones of hands and feet (10%), scapula (4%), pelvis (5%) and spine (2%) [3]. Osteochondroma of scapula, arising from the ventral surface, causes mechanical irritation on the chest wall, leading to formation of bursa. These bursa are lined by synovium and may become inflamed, infected or haemorrhagic. Clinically, bursa formation manifest as an enlarging mass causing restricted motion and winging of scapula. The term exostosis bursata was given originally in 1891 by Orlow, who described it as a bursal formation between osteochondroma and surrounding soft tissue [4]. Four bursae were seen in association with the chest wall and scapula [5]. In the superficial layers, between the inferior angle of scapula and latissimus dorsi and between superomedial aspect of scapula and trapezius muscle. In the deeper layers, between serratus anterior and subscapularis and between the serratus anterior and thoracic cage. This patient had bursal formation between serratus anterior and thoracic cage as evident in CT and MRI [Table/Fig-2]. This is better appreciated in trans-scapular view rather than frontal chest radiograph [Table/Fig-1]. Further imaging with ultrasound, aided in assessing the nature of bursal fluid and aspiration for cytological examination. Cortical and medullary continuity between osteochondroma and the parent bone is better visualized in CT. The three dimensional volume rendered CT allows optimal depiction of cortical and marrow continuity of the lesion and parent bone in osteochondroma [6] especially in areas of complex anatomy, such as ventral surface of the scapula [Table/Fig-3,4]. MRI gives an incomparable insight in visualizing the effect of the lesion on the surrounding structures and also in assessing the hyaline cartilage cap. MR sequences such as gradient recalled echo, T1, T2 weighted characterizes the nature of the content. The low signal intensity on T1-weighted images and very high signal intensity on T2-weighted MR images [Table/Fig-4,5] in scattered areas of cartilaginous cap, represents high water content [7–9]. These characteristics in MRI help in accurate measurement of cartilage cap thickness and more than 2 cm is considered as malignant transformation [10].
Conclusion
We recommend the multimodality approach, special views and post processing techniques for characterization and diagnosis of osteochondroma of scapula, which further contributes to treatment selection as well as roadmap for surgery.
[1]. Kwon OS, Kelly JI, Delayed presentation of osteochondroma on the ventral surface of the scapulaInternational Journal of Shoulder Surgery 2012 6(2):61 [Google Scholar]
[2]. Milgram JW, The origins of osteochondromas and enchondromas: a histopathologic studyClin Orthop 1983 174:264-84. [Google Scholar]
[3]. Vaishya R, Dhakal S, Vaish A, A solitary osteochondroma of the scapulaBMJ Case Reports 2014 2014:bcr2013202273 [Google Scholar]
[4]. Orlow LW, Die exostosis bursata und ihreentstehungDtsch Z Chir 1891 31:293-308. [Google Scholar]
[5]. Williams GR, Shakil M, Klimkiewicz J, Jannotti JP, Anatomy of the scapulothoracic articulationClin Orth 1999 359:237-46. [Google Scholar]
[6]. Kobayashi H, Kotoura Y, Hosono M, 3D- spiral CT of multiple exostosesComput Med Imaging Graph 1995 19:419-22. [Google Scholar]
[7]. Lee JK, Yao L, Wirth CR, MR imaging of solitary osteochondromas: report of eight casesAJR Am J Roentgenol 1987 149:557-60. [Google Scholar]
[8]. Aoki J, Sone S, Fujioka F, MR of enchondroma and chondrosarcoma rings and arcs of Gd-DTPA enhancementJ Comput Assist Tomogr 1991 15:1011-16. [Google Scholar]
[9]. De Beuckeleer LH, De Schepper AM, Ramon F, Magnetic resonance imaging of cartilaginous tu- mors: is it useful or necessary?Skeletal Radiol 1996 25:137-41. [Google Scholar]
[10]. Bernard SA, Murphey MD, Flemming DJ, Kransdorf MJ, Improved differentiation of benign osteochondromas from secondary chondrosarcomas with standardized measurement of cartilage cap at CT and mr imagingRadiographics 2010 255(3):857-63. [Google Scholar]