Oral Submucous Fibrosis (OSMF) is a chronic disorder characterized by fibrosis of the lining mucosa of the upper digestive tract involving the oral cavity, oropharynx and frequently the upper third of the oesophagus. Except in early forms of the disease the clinical presentation is characteristic due to fibrosis of lamina propria and submucosa with an increasing loss of tissue mobility [1]. Worldwide estimates of OSMF shows confinement to Indians and South East Asians with overall prevalence rate in India to be about 0.2% to 5% and prevalence by gender varying from 0.2% to 5% in males and 1.2- 4.5% in females [2]. The various forms of tobacco which causes OSMF are Pan, Pan Masala, Gutkha, Pan Parag, Mawa [3]. Amongst the structures communicating with the oral cavity the eustachian tube (pharyngotympanic tube) connects the middle ear cavity with the nasopharynx [4]. Extension of fibrosis into nasopharynx involving the pharyngeal orifice of eustachian tube and in the muscles, affects the functions of eustachian tube [5]. Normal opening of eustachian tube equalizes atmospheric pressure in middle ear; closing of eustachian tube protects middle ear from unwanted pressure fluctuations and loud sounds. Abnormal or impaired eustachian tube functions (i.e., impaired opening or closing) may cause pathological changes in the middle ear [6]. This in turn can lead to hearing impairment which can be evaluated by audiometry and tympanometry [7,8]. Pure tone audiometry is an electronic device which produces pure tones. It is the most common technique used for hearing assessment. Tympanometry is based on the principle that a stiffer tympanic membrane would reflect more of sound energy then a compliant one.
To assess the hearing efficiency in patients suffering from OSMF and to assess the severity of involvement/fibrosis of the eustachian tube in stage III and stage IV OSMF patients.
Materials and Methods
A case control study was done in the Department of Oral Medicine & Radiology for a period of six months. Only the patient who had fibrosis of the buccal mucosa, labial mucosa and soft palate (stage III, stage IV OSMF), according to Khanna JN and Andrade NN, were enrolled for study based on clinical examination [9]. The sample size of 45 calculated based on previous studies was divided into three groups of 15 each. Group A consisted of 15 patients with stage III OSMF. Group B consisted of 15 patients with stage IV OSMF and Group C consisted of 15 controls who did not have OSMF. Both ears were examined in each group and therefore a total of 30 ears were examined in each group. OSMF patients in the age group between 15 years to 55 years were included for the study. Cases of initial stages of OSMF, previous ear surgery, patients with ear wax, hearing aid, middle ear infections, trauma to ear, nasopharyngeal mass, patient working in noisy area, cleft palate, cleft lip, auto sclerosis were excluded from the study. Informed consent from patients and Institutional ethical clearance was obtained.
Audiological assessment was done by using a clinical audiometer graphic audiometer classic I-S and eustachian tube function by impedence tympanogram maico MI 34 (tympanometric evalution). The audiometric and tympanometric assessment were done by an ENT surgeon and the output was obtained as a graph. Pure tone audiometry is an electronic device which produces pure tones. It is the most common technique used for hearing assessment. Pure tone is delivered to the ear through headphone for air conduction and by bone vibrator for bone conduction [Table/Fig-1]. Hearing level in decibels above the normal threshold is plotted. The frequency tested usually ranged from 250 to 800Hz [10]. Tympanometry is based on simple principle when a sound strikes tympanic membrane, some of the sound energy is absorbed while the rest is reflected. A stiffer tympanic membrane would reflect more of sound energy then a compliant one. By changing the pressure in a sealed external auditory canal and then measuring the reflected sound energy, it’s possible to find the compliance or stiffness of the tympano-ossicular system and thus find whether there is fibrosis of eustachian tube or not [6] [Table/Fig-2].

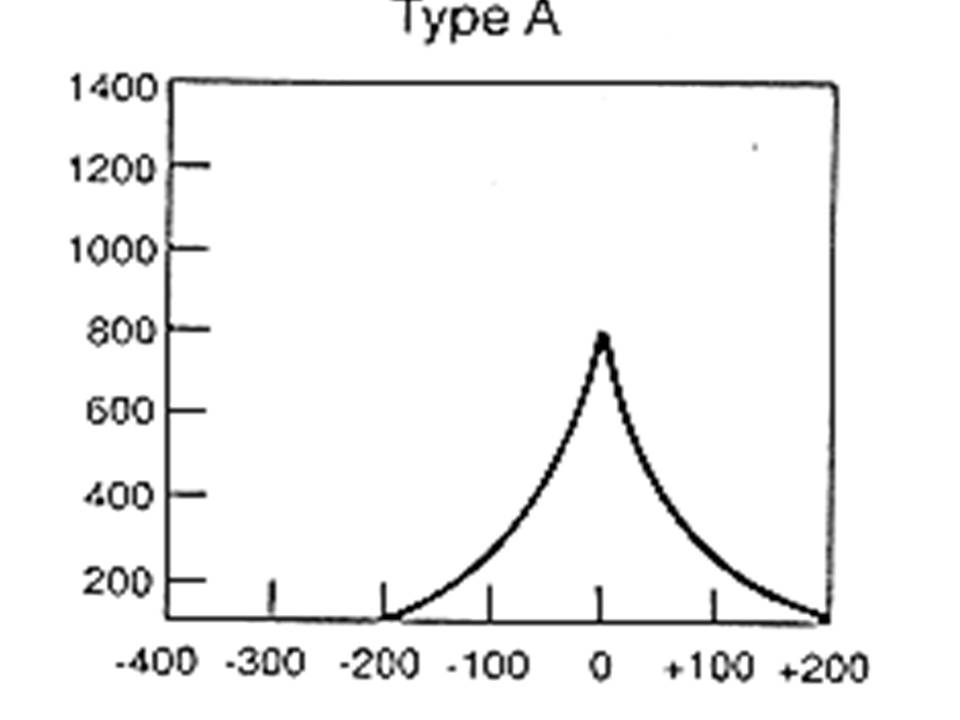
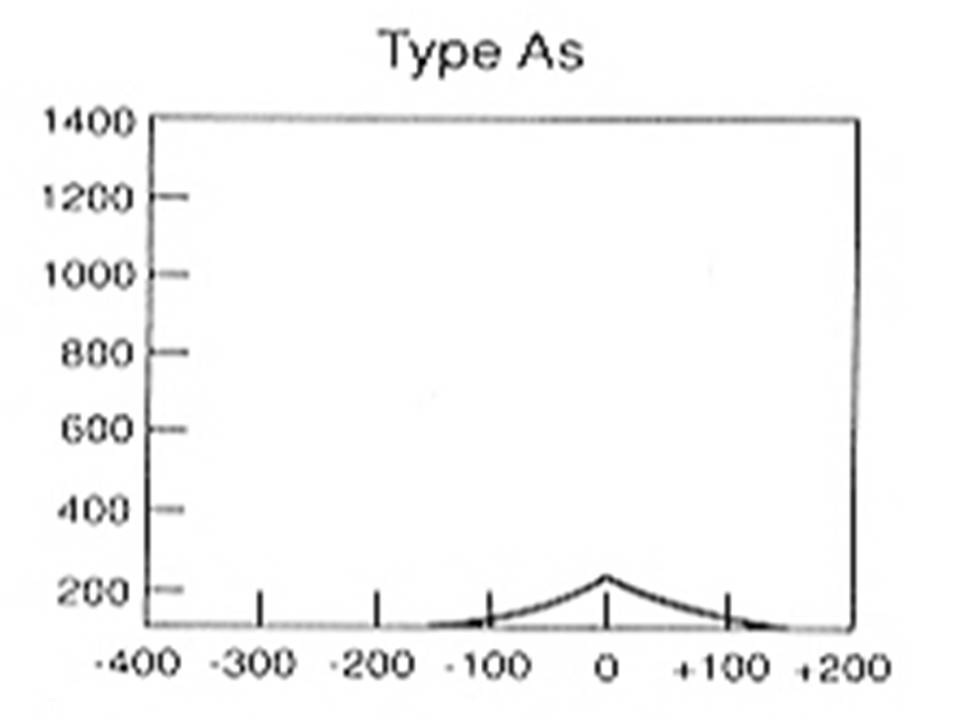
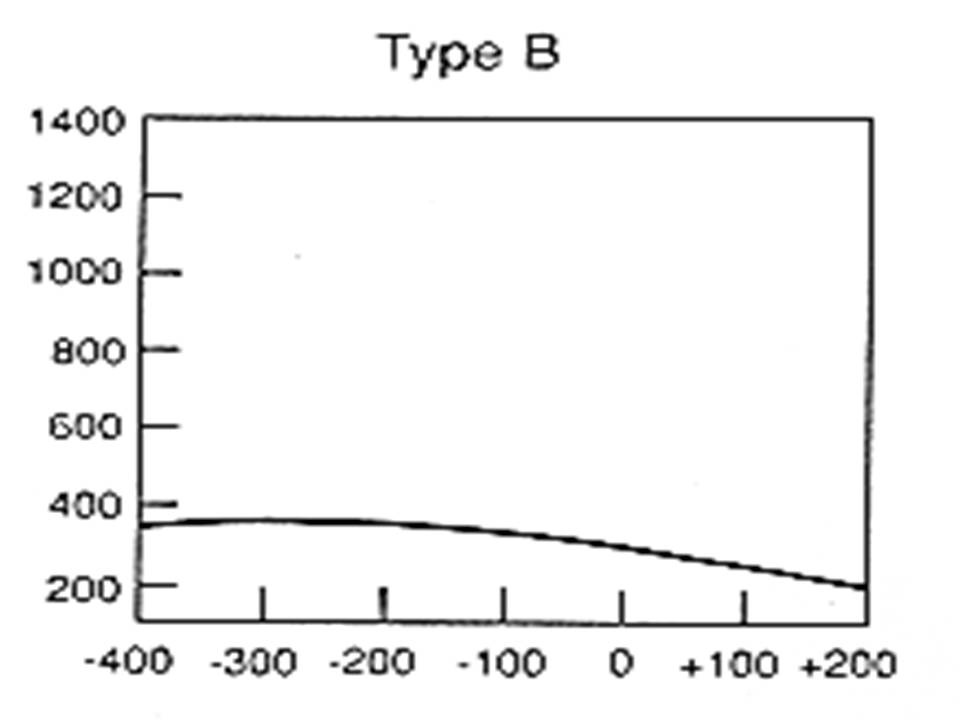
The patient’s ability to equalize the pressure difference between the surroundings and the middle ear is called the “tube function”. Tympanometry is performed in auto-tympo mode. The audiometer can automatically give a patient a constant over or under pressure of 200daPa in the auditory canal. A patient must swallow 8 to 10 times so that the over or under pressure that the tight tympanic membrane caused in the middle ear is equalized. The examiner records the compliance graph and if the Eustachian tube functions correctly, the middle ear will move in the opposite direction of the static pressure and thus, the shifted compliance peak shows that the function of eustachian tube are good. If there is no shifting of compliance peaks, then it means that it’s functioning poorly [8]. By charting the compliance of tympano auricular system against various pressure changes, different types of tympanogram (Assessment Curves-1,2,3) [11] [Table/Fig-3,4 and 5] were obtained.
Both the ears were examined for each case and control and were subjected to audiogram and tympanometric evaluation.
Results
Among stage IV cases, 86.7% were males and 13.3% were females. The average age of the patient in stage IV was about 40 years. Both ears were normal (or) either of it was affected. The results are shown in [Table/Fig-6,7].
Audiometric evaluation-Stage IV OSMF.
| Stage IV | Frequency(No. of Ears) | Percent |
|---|
| Negative | 07 | 23.3 |
| Positive | 23 | 76.7 |
| Total | 30 | 100 |
Tympanometric evaluation-Stage IV OSMF.
| Stage IV | Frequency(No. of Ears) | Percent % |
|---|
| A | 05 | 16.7 |
| As | 19 | 63.3 |
| B | 06 | 20.0 |
| Total | 30 | 100 |
Among stage III cases 73.3% are males and 26.7% females. Both ears were normal (or) either of it was affected. The results are shows in [Table/Fig-8,9]. Age and sex matched controls who did not have any hearing deficit were compared with Group A and Group B. Inter group comparisons were done between stage IV and stage III and controls and the results are shown in [Table/Fig-10,11,12 and 13]. The audiometric evaluation of stage IV OSMF cases [Table/Fig-6] showed 76% of cases positive for hearing impairment. Further study was done to evaluate the extent of fibrosis of eustachian tube in stage IV [Table/Fig-7] in which 63% of the cases showed as curve on the graph, which meant that there was impairment of hearing. The audiometric evaluation of stage III OSMF cases [Table/Fig-8] showed 43% were found to be positive for hearing impairment. The Tympanograph showed as curve in 47% of cases.
Audiometric evaluation in Stage III OSMF.
| Stage III | Frequency(No. of Ears) | Percent |
|---|
| Negative | 16 | 56.7 |
| Positive | 14 | 43.3 |
| Total | 30 | 100 |
Tympanometric evaluation in Stage III OSMF.
| Stage III | Frequency(No. of Ears) | Percent % |
|---|
| A | 12 | 40.0 |
| As | 14 | 46.7 |
| B | 04 | 13.3 |
| Total | 30 | 100 |
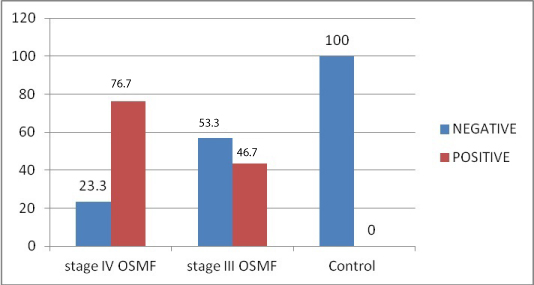
Inter group comparison of audiogram.
| Negative | % | Positive | % |
|---|
| Stage IV | 7 | 23.3 | 23 | 76.7 |
| Stage III | 16 | 53.3 | 14 | 46.7 |
| Control | 15 | 100 | | |
Inter group comparison of audiogram.
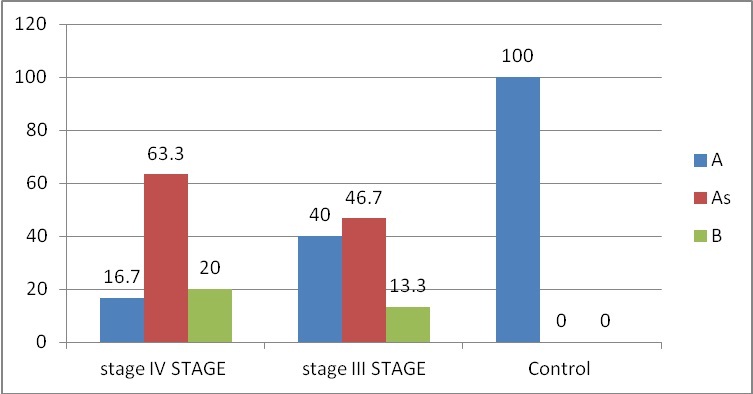
Inter group comparison of tympanogram.
| A | PER% | As | PER% | B | PER% |
|---|
| STAGE IV | 5 | 16.7 | 19 | 63.3 | 6 | 20 |
| STAGE III | 12 | 40 | 14 | 46.7 | 4 | 13.3 |
| CONTROL | 15 | 100 | | | | |
Inter group comparison of tympanogram.
Discussion
This study shows a positive clinical correlation between hearing loss and the disease progression [Table/Fig-14]. Sclerosis of tympanic membrane leads to reduction in hearing efficiency. In our study, it was evident that functions of the eustachian tube were affected as fibrosis of the oral mucosa progressed. Sclerosis of the tympanic membrane progressed as disease advanced. Palatal and paratubal muscles (levator veli palatini, tensor veli palatine, tensor tympani and salphingopharyngeous), which regulate the patency and function of pharyngeal orifice, may get affected, resulting in impairment of function and patency of eustachian tube. This leads to pain in the ear along with mild to moderate conductive loss of hearing [12].
Correlation of audiogram positive cases with tympanometry.
| AUDIOMETRY (POSITIVE) | TYMPANOMETRY (As) |
|---|
| STAGE IV | 76% | 63% |
| STAGE III | 43% | 47% |
In a study done by Shah M et al., tympanometric examination revealed, out of 54 ears normal tympanogram type –A curve in 42 (77.8%) ears [7]. Abnormal tympanogram type–B curve in none & type-C in 12 (22.2%) ears. Out of 54 ears, ETFT revealed no shift in compliance peaks in 15 (27.8%) ears with -200daPa pressure changes after swallowing.
In a study done by Gupta SC et al., tympanometric examination revealed, out of 106 ears, normal tympanogram type –A curve in 80 (75.5%) ears [8], abnormal tympanogram type–B curve in 17 (16.0%) & type–C in 9 (8.5%) of ears. Out of 106 ears, ETFT revealed no shift in compliance peaks in 24 (22.7%) ears with 200daPa pressure changes after swallowing.
In a study done by Sana Noor et al., eustachian tube function test revealed a statistically significant difference in eustachian tube function in OSMF patients and controls [13]. Further, they concluded that there was a significant increase in severity of dysfunction with increase in severity of disease.
Limitation
Hearing efficiency reduces as age advances. Therefore it might be a compounding factor too. The study could be done on a larger sample and it can also be done as pre and post treatment evaluation.
Conclusion
We would suggest that all patient’s with fibrosis of the oral mucosa be subjected for Audiological assessment and impedence tympanogram. Further, as the test is non-invasive, painless and less time consuming, it can be effectively used for educating the patient, which may be helpful in assessing the morbidity and in identifying the overall prognosis to find more appropriate therapeutic interventions.