Liver possesses dual blood supply; it receives blood from both the hepatic artery and the portal vein. Variations of the hepatic artery and its branches are exceedingly common. Variations in the origin and number of the hepatic arteries may be facilitated by defining the terms commonly used in describing such variations. These terms are “aberrant”, “accessory”, and “replacing”. A typical “normal” right hepatic artery (RHA) arises from the proper hepatic artery and supplies the right lobe of liver [1].
An aberrant RHA is one that arises from some other source than the proper hepatic artery. If an aberrant artery supplies the right lobe of the liver, the right lobe also receives supply from the proper hepatic artery of normal origin it is known as an aberrant accessory RHA. If an aberrant RHA constitutes the sole blood supply to the right lobe of the liver it is known as an aberrant replacing right hepatic artery, since it replaces the normal RHA [2].
RHA is known for its surgical and radiological importance. A thorough knowledge of the RHA anatomy is mandatory while performing hepatic surgery and hepatic arteriography. Because of anatomic variations in the RHA, surgical injuries in the liver can occur inadvertently by even the most experienced surgeon [2].
Hepatic arterial perfusion scintigraphy, Transhepatic Arterial Chemoembolization (TACE) and Hepatic Arterial Infusion (HAI) chemotherapy are the newer therapeutic techniques used in the treatment of primary and metastatic hepatic tumors that derive most of its blood supply from the hepatic artery [3]. These procedures need expert knowledge on the origin, course and variations of the RHA. So, the present study was aimed to find out the frequency of variations in the origin and course of the RHA.
Materials and Methods
The study was conducted in 60 embalmed adult cadavers of the age group between 50-80 years, allotted for dissection to the first year MBBS students during the year 2012-2015 at Mahatma Gandhi Medical College and Research Institute, Puducherry, India. Abdomen was opened by a linear midline incision extending from the xiphoid process to the pubic symphysis. Anterior layer of peritoneum was removed from the lesser omentum close to the lesser curvature of the stomach. Coeliac trunk arising as a ventral branch from the abdominal aorta was traced. Origin of the common hepatic artery from the coeliac trunk, aorta and superior mesenteric artery (SAM) was traced. The common hepatic artery and its branch gastroduodenal artery were identified. Proper hepatic artery in the hepatoduodenal ligament was traced and the relation of the common hepatic artery and the proper hepatic artery were noted. Origin of the RHA was traced and the presence of aberrant right hepatic arteries: (i) Replaced; (ii) Accessory, were noted. To identify the presence of aberrant right hepatic arteries, abdominal aorta was exposed from the level of origin of the coeliac trunk to the level of origin of the inferior mesenteric artery. Presence of an accessory or replaced right hepatic artery arising from the superior mesenteric artery, RHA and inferior mesenteric artery were noted. The course of normal and aberrant RHA from its origin to entrance into the right lobe of the liver was traced and structures related to it were noted. Aberrant right hepatic arteries were painted and photographed for documentation.
Statistical Analysis
We used simple proportion (frequency analysis) with the help of Open Epi Version 3.0 software.
Results
The RHA originating from the main trunk of the proper hepatic artery was found in 52 specimens (86.6%). Presence of aberrant RHA was found in 8 specimens (13.3%). Among the 8 specimens of aberrant RHA: (a) Replaced RHA arising from SMA was found in 5 specimens (8.3%); (b) Accessory RHA arising from SMA was observed in 3 specimens (5%) [Table/Fig-1,2 and 3].
Variation of RHA in 60 cadavers.
| Variation of RHA | No. of variations | Frequency (%) | 95% Confidence Interval |
|---|
| Aberrant RHA | 8 | 13.3 | 5.9 to 24.6 |
| Replaced RHA | 5 | 8.3 | 2.8 to 18.4 |
| Accessory RHA | 3 | 5 | 1.0 to 13.9 |
N= 60
Replaced RHA arising from superior mesenteric artery.
ReRHA-replaced right hepatic artery, SMA-superior mesenteric artery, CT-coeliac trunk, LHA-left hepatic artery, LGA-left gastric artery, SA-splenic artery, GDA-gastroduodenal artery, RGA-right gastric artery, CyA-cystic artery.

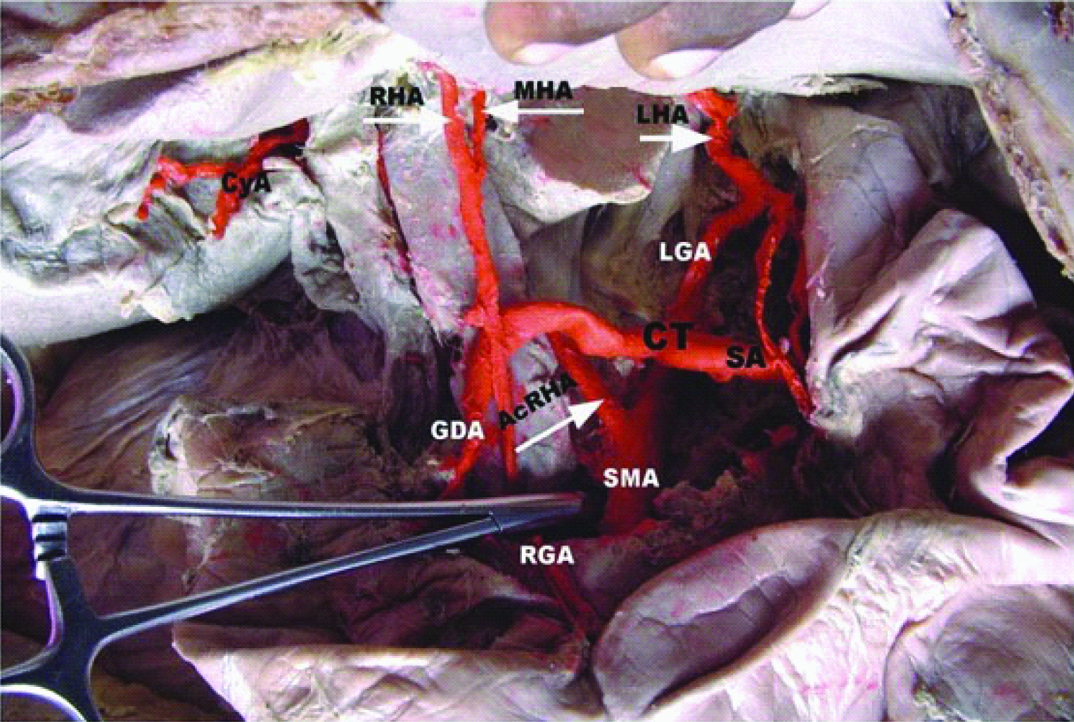
Accessory RHA arising from superior mesenteric artery.
AcRHA-accessory right hepatic artery, SMA-superior mesenteric artery, CT-coeliac trunk, LHA-left hepatic artery, MHA –middle hepatic artery, LGA-left gastric artery, SA-splenic artery, GDA-gastroduodenal artery, RGA-right gastric artery, CyA-cystic artery.
In 52 specimens, the RHA after its origin from the proper hepatic artery crossed anterior to the portal vein from left to right and passed behind the common hepatic duct to enter the Calot’s triangle where it coursed to the left of the cystic duct as it approached the cystic duct. Within the Calot’s triangle, the RHA gives origin to cystic artery and then it turned upwards behind the right hepatic duct to enter the right lobe of liver [Table/Fig-4]. In 5 specimens, the RHA after its origin from the proper hepatic artery crossed the common hepatic duct anteriorly from left to right to enter the Calot’s triangle was observed [Table/Fig-5]. The caterpillar like loop of the RHA was found in 2 specimens (3%). In 1 specimen the RHA crossed the common hepatic duct anteriorly to enter the Calot’s triangle, where it made a characteristic caterpillar like loop (hump) convexity of which pointed upwards and to the right and in another specimen the RHA crossed the common hepatic duct posteriorly to enter the Calot’s triangle where it made a characteristic caterpillar like loop convexity of which point towards the right and the convexity was less marked in this specimen [Table/Fig-6].
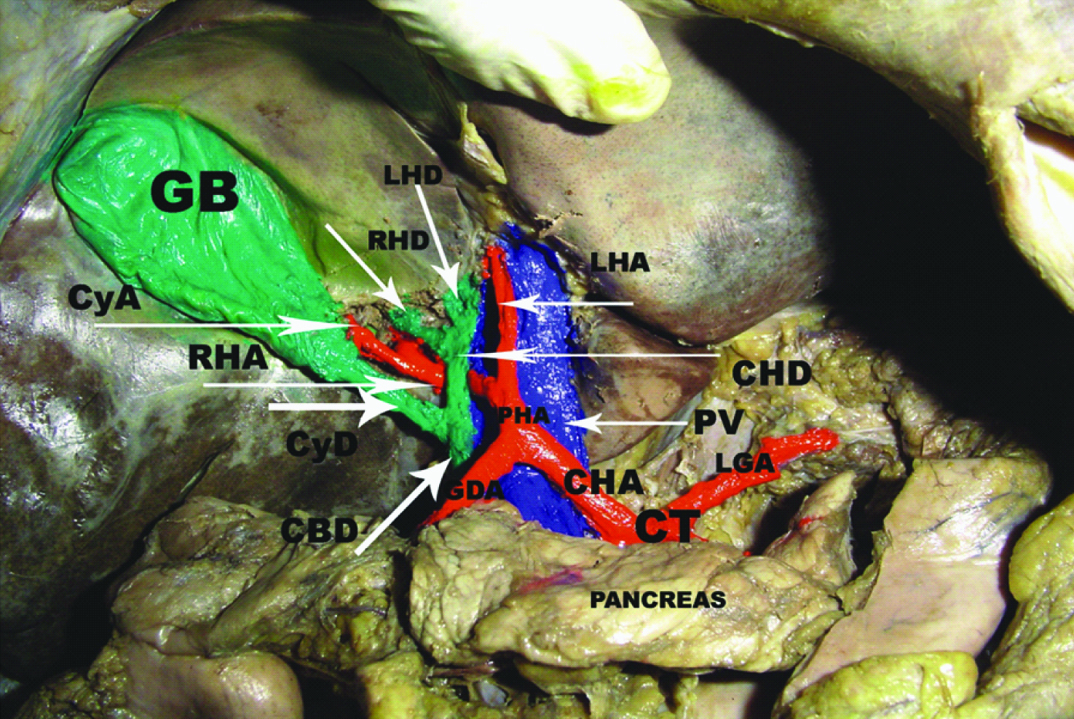
RHA passing dorsal to the common hepatic duct.
CHA-common hepatic artery, LHA-left hepatic artery, CT-coeliac trunk, PHA-proper hepatic artery, LGA-left gastric artery, GDA-gastroduodenal artery, CyA-cystic artery, PV-portal vein, GB-gall bladder, CHD-common hepatic duct, LHD-left hepatic duct, RHD-right hepatic duct, CyD-cystic duct, CBD-common bile duct.
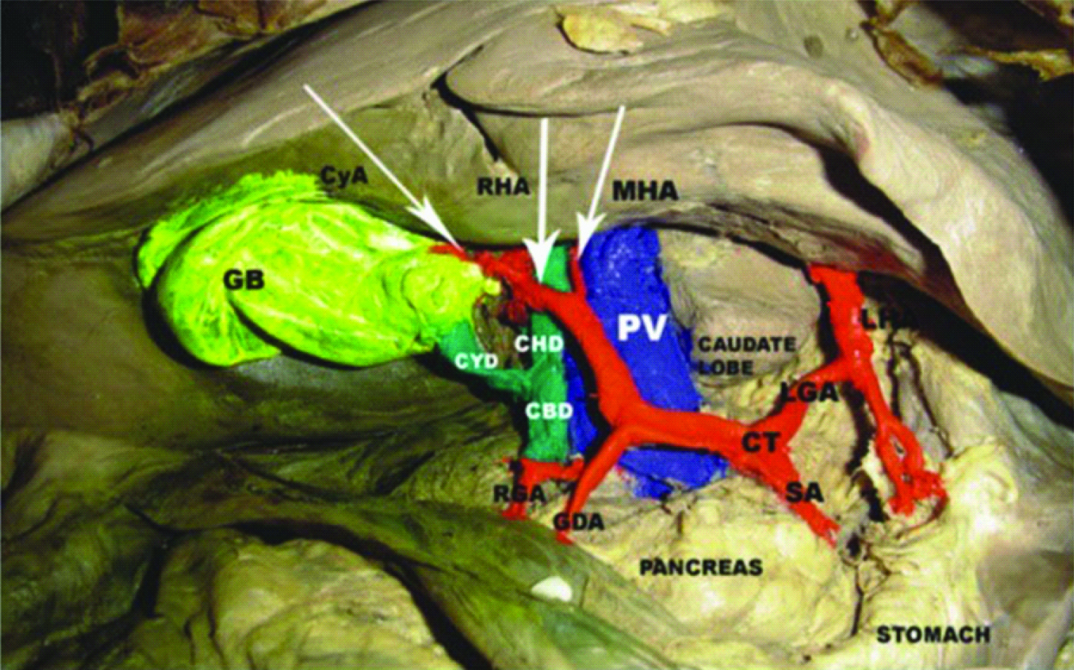
RHA passing ventral to the common hepatic duct.
LHA-left hepatic artery, CT-coeliac trunk, RHA –right hepatic artery, LHA-left hepatic artery, MHA-middle hepatic artery, LGA-left gastric artery, RGA –right gastric artery, GDA-gastroduodenal artery, CyA-cystic artery, PV-portal vein, GB-gall bladder, CHD-common hepatic duct, LHD-left hepatic duct, RHD-right hepatic duct, CyD-cystic duct, CBD-common bile duct.
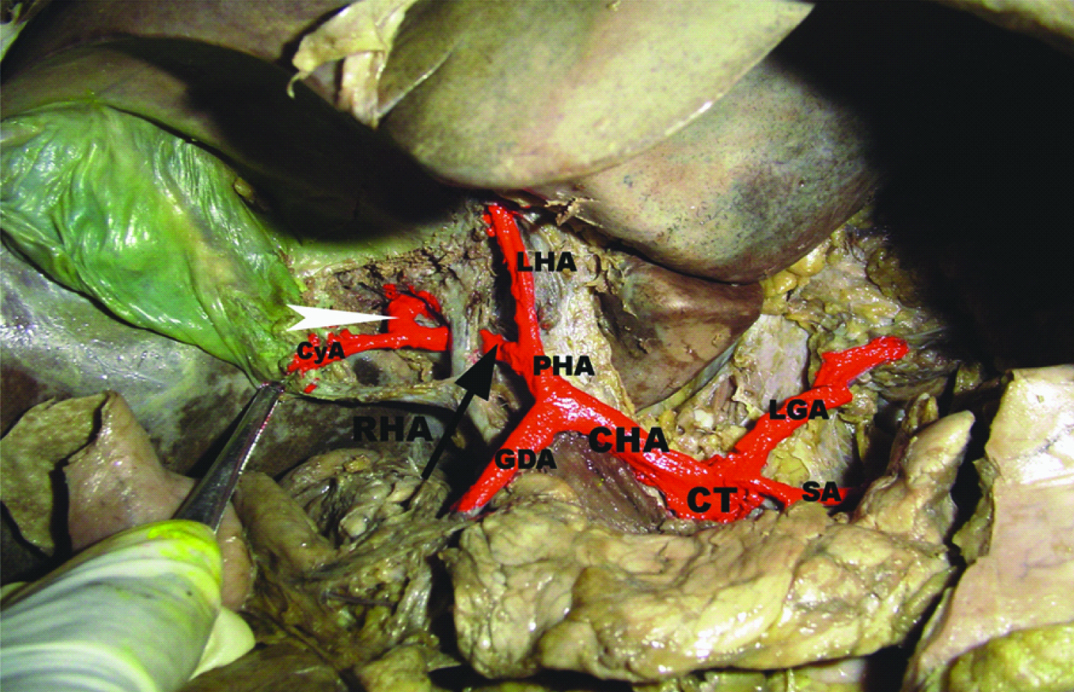
Caterpillar hump of RHA.
CT-coeliac trunk, CHA-common hepatic artery, SA-splenic artery, PHA-proper hepatic artery, RHA-right hepatic artery, LHA-left hepatic artery, LGA-left gastric artery, GDA-gastroduodenal artery, CyA-cystic artery, Arrow head- caterpillar hump of RHA.
Aberrant (replaced and accessory) RHA arising from the SMA was found in 8 specimens (13.3%). The aberrant RHA passed upward from left to right dorsal to the portal vein and common hepatic duct to reach the Calot’s triangle where cystic artery was given and then ascended upwards behind the right hepatic duct to reach the right lobe of liver.
Discussion
During development, the coeliac axis is derived from the 10th ventral segmental artery and SMA from the 13th segmental artery. The 11th and 12th segmental arteries normally regress [4,5]. Variations occur during this development and regression of the ventral segmental arteries lead to the multiple anomalies. Following normal development, the common hepatic artery usually arises as one of the three major branches of the coeliac axis. The common hepatic artery continued as the proper hepatic artery which gives the origin of the RHA. There are numerous anatomic variations of the hepatic arterial tree in the adult which results from variable persistence of elements of the embryologic blood supply [6].
RM Jones and KJ Hardy reported the origin of RHA from the proper hepatic artery 75%, Sureka et al., 79.6%, Bhardwaj 65% and Molmenti et al., 80%. In the present study it is 86.6%. So in the present study, the normal origin of RHA is higher than previous studies [7–10]. Baburao Kardile et al., reported RHA arising from the proper hepatic artery of hepatomesenteric trunk, and its source of origin from abdominal aorta [11]. Such findings were not found in the present study.
The presence of aberrant RHA in the present study was compared with earlier research findings. Our study was in par with Thompson study [12]. However, in our study the percentage of aberrant RHA was lower than others study [Table/Fig-7] [2,7,10,12–14]. The lower percentage of occurrence of aberrant RHA in the present study could be due to the less number of specimens studied compared to the earlier reports.
A comparative data on the occurrence of aberrant right hepatic artery.
| Authors Study | Aberrant RHA (%) |
|---|
| Thompson [12] | 13 |
| Daseler et al., [13] | 24 |
| Nicholas A Michels [2] | 26 |
| Van Damme JP [14] | 24 |
| R.M.Jones and K.J. Hardy [7] | 25.6 |
| Molmenti et al., [10] | 20 |
| Present Study | 13.3 |
In the present study, the presence of replaced and accessory RHA and its source of origin were compared with previous studies [Table/Fig-8,9] [2,8–10,13,15,16]. In our study, all the replaced and accessory RHA arose from the superior mesenteric artery alone. Nicholas A. Michels reported that in addition to the SMA, replaced RHA also found arising from coeliac trunk in 3%, from aorta in 2% and from the left gastric artery in 0.5% [2]. In the present study such origins of replaced RHA were not observed.
A comparative data on the presence of replaced and accessory right hepatic artery.
| Authors Study | Replaced right hepatic artery(%) | Accessory right hepatic artery(%) |
|---|
| Adachi [15] | - | 12.3 |
| Daseler et al., [13] | 16.8 | 7.2 |
| BinitSureka et al., [8] | 15.16 | 5.16 |
| NikhaBhardwaj [9] | - | 5 |
| Nicholas A.Michels [2] | 18 | 8 |
| Molmenti et al., [10] | 15-20 | 5 |
| Arunthathy Thangarajah and Ramesh Parthasarathy [16] | 9 | 3.5 |
| Present study | 8.3 | 5 |
A comparative data on the source of origin of aberrant right hepatic artery.
| Authors Study | Replaced RHA | Accessory RHA |
|---|
| Source of origin | Source of origin |
|---|
| SMA | CT | AORTA | LGA | SMA | CT | RDA | DPA | RGA |
|---|
| Adachi [15] | - | - | - | - | 10.3% | 2% | - | - | - |
| Nicholas A Michels [2] | 12.5% | 3% | 2% | 0.5% | 4.5% | 0.5% | 2% | 0.5% | 0.5% |
| Molmenti et al., [10] | 15-20% | - | - | - | 5% | - | - | - | - |
| Arunthathy Thangarajah and Ramesh Parthasarathy [16] | 9% | - | - | - | 3.5% | - | - | - | - |
| Present Study | 8.3% | - | - | - | 5% | - | - | - | - |
SMA - superior mesenteric artery, CT - coeliac trunk, LGA - left gastric artery, RDA -retroduodenal artery, DPA - dorsal pancreatic artery, RGA - right gastric artery.
Nicholas A Michel’s found accessory RHA in 8%, Binit Sureka et al., in 5.16%, Nikha Bhardwajin 5% and Molmenti et al., in 5%, Daseler et al., in 7.2%, Adachi in 12.3% [2,8,9,10,13,15]. In the present study accessory RHA was found in 5%, so the present study is in accord with Binit Sureka et al., Nikha Bhardwaj and Molmenti et al., study and lower than Adachi, Nicholas A. Michels and Daseler et al., study. Adachi also reported that the accessory RHA arising from the coeliac trunk in 2% in addition to SMA [15]. Nicholas A. Michels found it in addition to the SMA, 0.5% from the coeliac trunk, from retroduodenal artery in 2%, dorsal pancreatic artery in 0.5% and from the right gastric artery in 0.5% [2]. In the present study, all accessory RHA took origin from the SMA only. Braun MA et al., reported an unusual aberrant RHA arising from the right renal artery [17]. In the present study no such finding was observed.
According to Nicholas A Michels, Thompson, and Henry Hollinshead the coeliacal RHA may have a retrobiliary course in 85% (dorsal to duct system) and prebiliary course in 15% (ventral to duct system) [2,12,18]. Daseler et al., found in 80% the RHA coursing dorsal to duct and in 20% ventral to duct [13]. RHA was dorsal to duct in 75% and ventral to duct in 25% as per Russell T Wood Burne [19]. In the present study, in 86.6% RHA passes behind the duct system and in 8.3% the RHA passes anterior to the duct system.
The aberrant RHA from the SMA as per observation of Nicholas A Michels, in most instances proceeded upward dorsal to the portal vein [2] and Russell T Wood Burne stated that if the RHA appeared as the highest branch of the SMA, then it has to ascend through the lesser omentum posterior to the portal vein [19]. In the present study all the aberrant RHA (both replaced and accessory -13.3%) arising from the SMA passed upward from left to right and dorsal to the pancreas and portal vein and the common hepatic duct to reach the Calot’s triangle. The present study is in accordance with Nicholas A Michels and Russel T Wood Burne [2,19].
Limitation
The present study was done only at cadavers from South Indian locality. Prevalence of aberrant, replaced and accessory RHA based on genetic determination might limit generalization of findings to universal population. However the confidence intervals of three types of RHA (aberrant, replaced and accessory) in our study accommodate the percentages given by most of the author’s study in our comparison, justifying the generalization of study findings.
Conclusion
Right hepatic artery is subject to anatomical variations in its origin and course. Our study identified the variations in the origin and course of right hepatic artery. Thus a thorough knowledge of the right hepatic arterial anatomy and its variations in origin and course is mandatory for surgeons and radiologists in performing hepatic surgery and hepatic arteriography to avoid surgical injuries in the liver during operation procedures.
N= 60
SMA - superior mesenteric artery, CT - coeliac trunk, LGA - left gastric artery, RDA -retroduodenal artery, DPA - dorsal pancreatic artery, RGA - right gastric artery.