It has been extremely difficult to treat patients with sepsis admitted in the Intensive Care Unit (ICU) due to various reasons. Unfortunately, due to the prevalence of resistant bacteria, even in the community, our in-house antibiotic armamentarium fails in such patients. This has been observed to be even more predominant in patients that are referred from another hospital. In fact, most intensive care units in India encounter the same problem. The advent of the so-called post antibiotic era seems imminent where we will be at the mercy of the so called “superbugs.”
From the time of the discovery of penicillin by Alexander Fleming until today, the beta-lactam group of antibiotics has been the mainstay in treating various infections [1]. However, these bacteria carry plasmids that harbour antimicrobial-resistant coding genes, which are responsible for the emergence of resistant bacteria. Therefore, these plasmids ensure resistance of the bacteria to beta-lactam and its inhibitors. They also encode resistant determinants for other antibiotics. Selective pressure from human and veterinary medicine promotes enhancement of these resistance mechanisms, limiting the choice of antibiotics for treatment. Methicillin was introduced in the year 1960 for treatment of penicillin-resistant Staphylococcus and in 1964, the first case of MRSA (methicillin-Resistant Staphylococcus aureus) was reported [2], followed by the emergence of similar conditions such as VISA (Vancomycin Intermediate Staphylococcus aureus), VRSA (Vancomycin-Resistant Staphylococcus aureus), ESBL (Extended Spectrum Beta Lactamase), etc [3–6]. Carbapenems (imipenem, meropenem, ertapenem, and doripenem) are often used as the last resort to inhibit ESBL producing and MDR Gram negative organisms [7]. Nevertheless, an increased resistance pattern has been observed with carbapenems drugs. Among these, the emergence of carbapenem-resistant Enterobacteriaceae has been recognized by Thomas Frieden, Director of CDC, as a triple threat [8]. It must be considered before it is too late.
The emergence of such dangerous bacteria has created a major public health problem, which is compounded by the shortage of new antibiotics for inhibiting CRE [9]. Members of the Enterobacteriaceae family are the most common clinical isolates found, and can be acquired in the community or at the hospital. Enterobacteriaceae are gut flora. They serve as reservoirs for contaminating the environment and fomites and therefore can spread more easily in the ICU. The resistance mechanisms in these organisms are easily transferred as they are located in jumping genes or transposons. The selection pressure of antibiotic abuse in veterinary and human medicine contributes to the emergence of resistance patterns like ESBL [10]. Carbapenems are one of the drugs we use as a last resort in such cases of resistance. However, there seems to be a disturbing trend of carbapenem-resistant Enterobactericeae among clinical isolates. Since we are aware of the colonising capabilities and the emergence of various resistance patterns in the community, we embarked upon this pilot study to understand the baseline epidemiology of CRE carriage rates among critically ill adult patients admitted directly from the community to the hospital ICU.
Materials and Methods
This pilot study was performed in January 2015 among patients admitted to the 16-bedded ICU of a tertiary care hospital in western Mumbai, Maharashtra, India. The study was approved by the hospital ethics committee.
Inclusion criteria: All adult patients directly admitted to the ICU of the hospital over a period of one month, i.e., in January 2015, from whom we could collect first stool samples at the time of admission were included in the study.
Exclusion criteria: Patients shifted from other units of our hospital/other hospitals/nursing homes to the ICU, paediatric patients and postoperative patients kept for observation were excluded. The target population was selected for two reasons. First, defined patient population and second patients had many reported risk factors for CRE colonization. A stool sample was collected on the day of admission and thereafter on the same day each week over the entire study period.
Microbial Culture and Identification
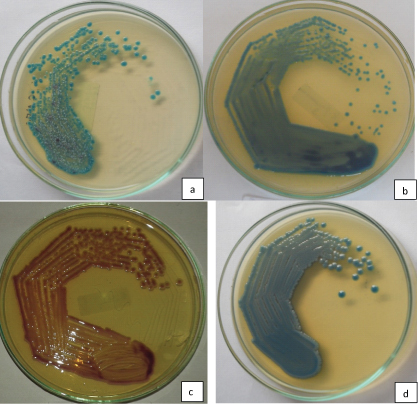
Sample Processing: CRE screening: On day one samples were inoculated on KPC agar (Hi-Media, Mumbai), and on day 2 any positive growth was identified according to the colony morphology on the KPC agar [Table/Fig-1]. Further identification and antibiotic sensitivity was confirmed by standard laboratory technique.
CRE Isolates on KPC Agar (a) Klebsiella oxytoca, (b) Enterobacter aerogenes, (c) Escherichia coli and (d) Klebsiella pneumonia.
Antibiotic Sensitivity Test: The Enterobacteriaceae isolates were tested for antibiotic sensitivity based on standard laboratory technique as per Clinical and Laboratory Standards Institute (CLSI) guidelines with commercially available discs (Hi-Media, India [11]. Escherichia coli ATCC 25922 was used as control.
Phenotypic Confirmation of CRE was done by Modified Hodge test and Imipenem + Imipenem-EDTA disc synergy Test [12] (I+IE DST).
Modified Hodge test [11] was carried out in MHA (Hi-Media, Mumbai, India) as per CLSI 2014 guidelines. Overnight culture suspension of Escherichia coli ATCC 25922 and 10μg Ertapenem disc (BD-BBL) were used. After overnight incubation, the plates were observed for the presence of a “cloverleaf shaped” zone of inhibition. The plates with such zones were interpreted as modified Hodge test positive.
EDTA –Disc Diffusion Synergy Test: A 10μg of imipenem disc (Hi-Media, India) was placed on the agar and a 10μg imipenem-EDTA disc was placed 10mm apart from edge-to-edge. After overnight incubation, the presence of an enlarged zone of inhibition was interpreted as EDTA synergy positive.
Molecular Confirmation: CRE grown in KPC agar were further studied for molecular characterization [13]. We looked for VIM, IMP, NDM1, OXA, and KPC genes by PCR using the set of primers and PCR conditions mentioned in [Table/Fig-2].
Polymerase Chain Reaction Conditions, Primers and Amplicon Size for Detection of Carbapenemase Genes among CRE Isolates.
| Sr. No. | Gene | PCR conditions | Primers | Amplicon size |
|---|
| 1 | bla-VIM | 10 minutes at 94°C and 36 cycles of amplification consisting of 30 s at 94°C, 40 s at 52 °C and 50 s at72 °C, with 5min at 72 °C for the final extension | VIM-F-5-GATGGTGTTTGGTCGCATA-3VIM-F-5-CGAATGCGCAGCACCAG-3 | 390bp |
| 2 | blaIMP | 94°C for 5 minutes followed by 36 cycles of 94°C for 30 s, 52 °C for 40 s and 72 °C for 50 s and 5min at 72 °C | Imp-F-5-GGAATAGAGTGGCTTAAYTCTC-3Imp-R-5-CCAAACYACTASGTTATCT-3 | 188bp |
| 3 | blaKPC1 | 94°C for 5 minutes followed by 36 cycles of 94°C for 30 s, 52 °C for 40 s and 72 °C for 50 s and 5min at 72 °C | Kpc-F-5-CTTGCTGCCGCTGTGCTG-3Kpc-R-5-GCAGGTTCCGGTTTTGTCTC-3 | 490bp |
| 4 | blaNDM1 | 940 C for 10 min, followed by 36cycles of 940 C for 30 s,520 C for 40 s and 720 C for 30 s and 720C for 5 min | NDM-F-5 GGTTTGGCGATCTGGTTTTC-3NDM-F-5-CGGAATGGCTCATCACGATC-3 | 621 bp |
| 5 | blaOXA | 950 C for 5 min, followed by 32cycles of 950 C for 30 s, 560 C for40 s and 720 C for 50 s and 720 C for 10 min | OXA-F 5-ATGGAAGGGCGAGAAAAGG-3OXA-R 5-TTGCATGAGATCAAGACCGATA-3 | 127 bp |
Risk Factors for CRE Carriage: A case-control study was performed to identify factors associated with CRE faecal carriage. Cases were patients with a positive CRE screening culture and controls were patients with negative screening cultures.
Statistical Analysis
Statistical analysis was carried out using Yates correction method for pooling the data under Chi-Square test among clinical conditions and CRE positive and CRE negative.
Results
Twenty eight (51.85%) Carbapenem-Resistant Enterobacteriaceae (CRE) isolates were obtained from 54 stool samples on KPC agar. The species distribution of the observed CRE isolates is listed in [Table/Fig-3]. Klebsiella pneumonia was the most common carbapenem-resistant isolate, closely followed by Escherichia coli. Phenotypic confirmation of the CRE isolates revealed 24 out of 28 screen positive isolates were MHT positive [Table/Fig-4]. All the Escherichia coli, 9 Klebsiella pneumoniae, 3 Klebsiella oxytoca, and 1 Enterobacter aerogenes strains were MHT positive [Table/Fig-5]. Four isolates that were MHT negative were subjected to MBL detection by I+IE DST. Two K.pneumoniae strains and one Klebsiella oxytoca strain were found to be positive and one K pneumoniae strain was MHT and I+IE DST negative.
Species distribution of CRE Isolates in Stool Samples.
| Organisms | Total |
|---|
| Klebsiella pneumonia | 12 (42.8%) |
| Escherichia coli | 11(39.2%) |
| Klebsiella oxytoca | 4(14.2%) |
| Enterobacter aerogenes | 1(3.5%) |
| Total | 28 |
Positive modified hodge test.

Modified hodge test results.
| Sr. No. | Organisms | MHT Positive | MHT Negative |
|---|
| 1 | Klebsiella pneumoniae | 9 | 3 |
| 2 | Escherichia coli | 11 | - |
| 3 | Klebsiella oxytoca | 3 | 1 |
| 4 | Enterobacter aerogenes | 1 | - |
| Total | 24 | 4 |
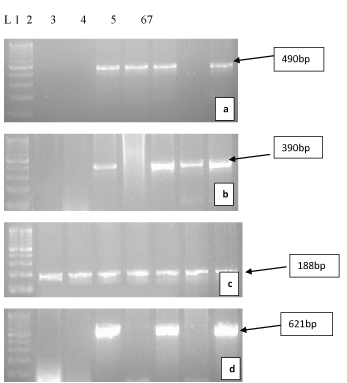
For genotypic characterization PCR was performed to look for VIM, IMP, NDM1, OXA, and KPC genes [Table/Fig-6]. Nine strains were positive for bla(KPC) gene, from which 7 were K.pneumoniae and one each of E.coli and K.oxytoca was observed. Fourteen strains were positive for VIM and 15 were positive for the IMP gene [Table/Fig-7,8].
Gel Electrophoresis Pictures of Resistant Genes [“L” is DNA ladder of 100 base pairs] a) KPC gene: 490 bps; b) VIM gene: 390 bps; c) IMP gene: 188 bps and d) NDM gene: 621 bps.
Phenotypic and genotypic characteristic of CRE isolates.
| Sr.No | Organism | MHT | I/IETest | Genotypic Characterization |
|---|
| OXA | VIM | IMP | NDM1 | KPC |
|---|
| 1 | Kpn | + | - | - | + | + | - | - |
| 2 | Kpn | + | - | - | + | + | + | + |
| 3 | Kpn | - | + | - | + | + | + | - |
| 4 | Koxy | - | + | - | - | - | - | - |
| 5 | Kpn | + | - | - | - | - | - | - |
| 6 | Kpn | - | + | - | + | + | + | + |
| 7 | Kpn | + | - | - | + | + | + | + |
| 8 | Kpn | + | - | - | + | + | + | + |
| 9 | Eco | + | - | - | - | - | - | - |
| 10 | Kpn | + | - | - | - | - | + | + |
| 11 | Eco | + | - | - | - | - | - | - |
| 12 | Kpn | + | - | - | - | - | - | - |
| 13 | Eco | + | - | - | + | + | - | - |
| 14 | Eco | + | - | - | - | - | - | - |
| 15 | Koxy | + | - | - | - | + | - | - |
| 16 | Eco | + | - | - | - | - | - | - |
| 17 | Koxy | + | - | - | + | + | + | + |
| 18 | Eaer | + | - | - | + | + | + | - |
| 19 | Eco | + | - | - | - | - | - | - |
| 20 | Kpn | - | - | - | - | - | - | - |
| 21 | Eco | + | - | - | + | + | - | - |
| 22 | Eco | + | - | - | + | + | - | + |
| 23 | Koxy | + | - | - | - | - | - | - |
| 24 | Kpn | + | - | - | + | - | - | + |
| 25 | Eco | + | - | - | - | + | - | - |
| 26 | Eco | + | - | - | + | + | - | - |
| 27 | Kpn | + | - | - | - | + | - | + |
| 28 | Eco | + | - | - | + | + | + | - |
| | | | 0 | 14 | 16 | 9 | 9 |
Distribution of KPC and OXA Genes among Different Isolates.
| Sr. No. | Organisms | KPC Producers | KPC Non-Producers |
|---|
| 1 | K. pneumonia | 7 | 5 |
| 2 | E. coli | 1 | 10 |
| 3 | K. oxytoca | 1 | 3 |
| 4 | E aerogenes | Nil | 1 |
| Total | 9 | 19 |
Six isolates were harbouring all the three genes and among them four were K.pneumoniae, one was E.coli, and one was K.oxytoca. Seven isolates had both VIM and IMP genes: four E.coli, 2 K.pneumoniae, and 1 K.oxytoca. Among K.pneumoniae, one had VIM and KPC genes and one had IMP and KPC genes together. One of the K.oxytoca isolate, which was DST positive, did not contain any of the genes [Table/Fig-8]. Antibiotic Sensitivity Test of the isolates showed maximum sensitivity to Colistin (100%) and Tigecycline (95%), followed by Cotrimoxazole (23%), Tobramycin, and Gentamicin 7.69%. Levofloxacin and Amikacin showed 3.85% sensitivity pattern.
Statistical analysis showed significant difference between the clinical conditions of patients and colonization/carriage of CRE at 5% and 1% level of significance.
Discussion
Members of the family Enterobacteriaceae are among the most important bacterial human pathogens, accounting for the majority of the bacteria isolated from clinical samples. A major concern is that these Gram-negative bacilli rapidly acquire resistance to one or more antimicrobial agents traditionally used for treatment. One of the most concerning emerging resistance traits among Gram-negative bacteria is the ability of the organisms to produce carbapenem-hydrolyzing β-lactamases, which confer resistance to almost all β-lactams [14]. The occurrence of multidrug resistant carbapenem hydrolysing Gram-negative bacteria is increasing worldwide.
The most clinically significant carbapenemases are KPC, MBLs (namely VIM, IMP, NDM types) and OXA. These genes are located on mobile genetic elements, allowing them to spread easily. Recognition of the presence of carbapenemase producers is of paramount importance for effective treatment and control. Currently, MBLs and KPC are considered a major threat in Enterobacteriaceae [Table/Fig-9], representing a potential source of clinical failure in patients treated with almost all beta-lactam agents [15].
Distribution of Metallobetalactamase Genes (VIM, IMP and NDM1).
| Sr. No. | Organisms | VIM | IMP | NDM1 |
|---|
| 1 | Klebsiella pneumoniae | 7 | 7 | 6 |
| 2 | Escherichia coli | 5 | 5 | 1 |
| 3 | Klebsiella oxytoca. | 1 | 2 | 1 |
| 4 | Enterobacter aerogenes | 1 | 1 | 1 |
| Total | 14 | 15 | 9 |
In India, there is large variance in the reported carbapenem resistance rate among GNB with the lowest documented occurrence of carbapenem resistance among Enterobacteriaceae being 1.8% and the highest being approximately 51% [16]. Taneja et al., found it to be 36.4%, whereas Datta et al., reported the presence of 7.87% carbapenem resistant strains in their study [17,18].
Either stools or rectal swabs (with or without enrichment in the presence of a carbapenem) can be plated on selective media for CRE screening; however, rectal/ peri-rectal swabs are less sensitive than stool specimens [19]. Hence we choose stools as the samples for our study.
No consensus on the optimal method for CRE screening is available yet. The CDC method (CDC-TS) of CRE screening comprises inoculation of the sample onto a Tryptic soy broth with a 10μg meropenem disc then swabbing it the next day onto MacConkey agar. Different studies have used different culture-based techniques like MacConkey agar plates supplemented with 1μg/ml imipenem, CHROM agar KPC, MacConkey Agar with imipenem, meropenem and ertapenem disc (10μg), and two-step selective broth enrichment method using a 10μg carbapenem disc to evaluate gut colonization with CRE with good performance [20]. We have used CHROM agar KPC for CRE screening of our patients. Evaluation of CHROM agar KPC for Rapid Detection of Carbapenem-Resistant Enterobacteriaceae by Samra et al., showed a sensitivity and specificity of 100% and 98.4%, respectively, relative to PCR [21]. Gilad et al., reported that CHRO Magar KPC can be employed for processing of specimens used for monitoring carbapenem-resistant Enterobacteriaceae; however, in the presence of KPC-negative ertapenem-resistant strains or in the detection of KPC-producing E.coli, its application may be limited due to its limited performance [22]. In our study, the overall CRE carriage rate was 51%. There is a paucity of data on carriage rates of CRE in stool samples. In one study by Swaminathan et al., the overall prevalence of CRE carriage was 5.4% [23]. CRE carriage rate was 7.1% in another study [24]. In a prospective study by Kothari et al., 75 healthy, vaginally delivered, antibiotic naive, breast fed neonates were studied for gut colonization and it was found that colonization with CRE was rare with only one detected isolate of Enterobacter [25]. Twenty four (9.9%) isolates demonstrated carbapenemase activity among 242 screened Enterobacteriaceae isolates in a study from Delhi [26]. Out of 62 isolates, 12 (29.26%) E.coli and 8 (38.09%) Klebsiella spp. were found to be positive for MBL production in a study by Aggarwal et al., [27]. Our results demonstrate a disturbingly high carriage rate, which could just be the tip of the iceberg and more patients might be carrying such resistant bugs, which could have been successfully screened if a supercarba medium was used. In one study, various screening methods were compared and it was found that the supercarba medium was highly sensitive in the detection of CRE carriage in stool, including the detection of OXA type genes [28].
Accurate detection of CRE by phenotypic and genotypic assays has an important clinical and epidemiological value [29]. The MHT based on in-vivo production of a carbapenemase by a carbapenemase-producing strain has been suggested for phenotypic confirmation of carbapenem resistance by CLSI, and can be used as the first step in detecting the carbapenemase activity of candidate isolates [29]. The sensitivity and specificity of MHT in our study, when compared with the genotypic method, were 85.71% and 28.57%, respectively. MHT often lacks specificity (e.g., false-positive results for high-level AmpC producers or CTX-M-type ESBL producers, Enterobacter species) and sensitivity (e.g., weak detection of NDM producers), but works well for the detection of KPC and OXA-48 producers [29].
The most classified carbapenemase gene in India is NDM. Two hundred and thirty-five ertapenem-non-susceptible (MIC≥0.5 mg/L) isolates of Enterobacteriaceae from the worldwide Study for Monitoring Antimicrobial Resistance Trends (SMART) 2009 programme were screened using a multiplex PCR for the presence of bla (KPC), bla (OXA-48), bla (VIM), and bla (NDM-1) genes. Bla (NDM-1) was identified in 33 isolates and all of them were from India [30]. Recent studies on the isolation of CRE (NDM-1) from environmental samples and community acquired infections indicate that the NDM-1 enzyme, which produces CRE, may be widely distributed in India [31]. However, there is paucity of data regarding faecal carriage of CRE. Regarding the faecal carriage of VIM/IMP genes, perhaps this is the first study from India. As per our knowledge There are very few reports of VIM/IMP type MBLs in Enterobacteriaceae from clinical isolates in India [19,25]. The most common MBL subtype in one study was the bla(IMP), followed by bla(VIM) and bla (SIM), again from clinical isolates. The study also demonstrated concurrent occurrence of multiple MBL genes in a single isolate [32].
Stool samples were screened for the presence of CRE in a Chinese university hospital and out of the eight CREs detected two were KPC (IMP-4 and NDM-1) [33]. In another study, from Greece with a total of 226 patients, 164 (72.6%) were colonized with KPC-Kp within an average of 9.1 days of ICU stay [34]. In our study, 9 out of 28 patients (32.1%) were found to be harbouring the bla(KPC) gene. Colonization with CRE was found to be rare in one of the Indian studies where only one baby harboured Enterobacter species and was found to be positive for bla(KPC-2) [25]. We did not find any carriage of OXA gene in our study. Shanti M et al., observed that OXA-48/OXA-181 is not a major mediator of carbapenem resistance among Enterobacteriaceae [35].
Yet again, there is limited data related to the risk factors for acquiring CRE and its clinical outcomes. Considering these facts, this study attempted to analyze the factors influencing the acquisition of carbapenemase producing Enterobacteriaceae and its clinical outcomes. Analysis revealed that past usage of more than 1 class of antibiotics emerged as a significant risk factor that influenced the acquisition of CRE [Table/Fig-10].
Significant risk factors associated with CRE.
| Characteristics | CarbapenemaseProducers (n=26) | Non-Carbapenemase producers (n=26) | p-value* |
|---|
| Presensence ofcomorbidities | 19 | 07 | 0.0095 |
| Prior antibiotic use(3months before) | 20 | 05 | 0.0013 |
Use of several classes of antimicrobials, namely cephalosporins, fluoroquinolones, metronidazole, and carbapenems, contributes significantly to the development of resistance to carbapenems [36]. Mechanical ventilation {odds ratio (OR), 11.5}, pulmonary disease (OR, 5.2), days of antibiotic therapy (OR, 1.04), and CRE colonization pressure (OR, 1.15) were independently associated with CRE acquisition [23]. In another study, the independent predictors for CRE colonization included Charlson’s score greater than 3 {OR, 4.85 (95% confidence interval (CI), 1.64-14.41)}, immunosuppression {OR, 3.92 (95% CI, 1.08-1.28)}, presence of indwelling devices {OR, 5.21 (95% CI, 1.09-2.96)}, and prior antimicrobial exposures {OR, 3.89 (95% CI, 0.71-21.47)} [24].
This is the first study where we have looked for the carriage rate of CRE among critically ill patients along with molecular characterization. There are not many, hardly any reports from India that have studied the presence of genes like VIM/ IMP or KPC.
Limitation
A major drawback of our current study is that it was performed as a pilot study over a very short duration. Due to time and resource constrains, characterization of other non-enzymatic mechanisms mediating carbapenem resistance, such as upregulated efflux pumps, porin defects, and hyper production of AmpC beta-lactamase, were not performed in this study.
Conclusion
The results of this study indicate a high prevalence of faecal carriage among patients hospitalized in our ICU, which is a cause of concern. Microbial surveillance of rectal flora in stools of patients in ICUs can guide clinicians about gut colonization of CRE as these groups of patients are at risk of possible endogenous infection, underlining the necessity for proper management of antibiotic therapy within healthcare units as well as stringent infection control and prevention practices like strict contact precautions for all CRE positive carriers. In order to prevent the spread of CRE prospective cases, a controlled study with adequate sample size and a primary objective to identify the risk factors for infection with carbapenemase-resistant Enterobacteriaceae and the outcome of such infections is essential to have a clear understanding of this problem. Based on this study, it seems that the prevalence of CRE colonisation in patients admitted to our hospital is very high. This should be confirmed with a larger study to assess causality. From this study, it seems prudent to screen patients for CRE as contact isolation precautions for these patients would go a long way in restricting the spread of these organisms and contamination of the environment.