Radiation is a component of man’s physical environment, and is broadly classified into ionizing and non-ionizing radiation. The most energetic form and of major public health significance is ionizing radiation. In normal circumstances 80% of our exposure to ionizing radiation comes from natural sources of which radon gas is by far the most significant, while the other 20% comes from man-made sources, primarily medical X-rays. Use of ionizing radiation in medical imaging for diagnostic and interventional purposes has risen dramatically in recent years with a concomitant increase in exposure of patients and health workers to radiation hazards; medical and dental X-rays now constitute the major man-made sources of radiation exposure [1–3]. While reports from studies demonstrated dramatic rise in the prevalence of adverse health effects following exposure to ionizing radiation over the past two decades [4,5], the documented evidence of poor knowledge of radiation safety among various cadres of health workers at risk of occupational exposure shows the enormity of the problem at hand [6–8].
Although the adverse health effects of ionizing radiation such as cataract, skin erythema, and cancers among others, are known to vary according to dose and duration of exposure, it is assumed that there is actually no safe dose of ionizing radiation [9]. The focal point for radiation safety based on this assumption is ‘the ALARA concept’ [10] this entails that radiation exposure be reduced to ’As Low As Reasonably Achievable (ALARA)’ but not exceeding the limit on effective dose recommended by the International Commission on Radiological Protection (ICRP) [11].
An estimated 20 to 30 percent of radiological examinations prescribed by doctors have been found to be of no use in the management of the patients for which they were ordered. Also, underestimation of doses associated with various imaging modal-ities was found to be prevalent among healthcare professionals [12,13]. These findings support the consensus of opinion that exposure to radiation hazards can be minimized through compliance with fundamental radiation protection principles of optimization and justification [14,15].
In recent years, accessibility to modern medical imaging machines in the healthcare facilities in Nigeria has improved tremendously; resulting in increased risk of radiation exposure to the patients and health workers. In recognition of this threat, the Nigeria Nuclear Regulating Authority (NNRA) had re-invigorated monitoring of facilities (both medical and non-medical) that use ionizing radiation in the country to enforce compliance with the Nigeria Basic Ionizing Radiation Regulations (NBIRR) 2003 [16].
The contents of the NBIRR 2003 are basically in line with the ICRP regulations. It recommended an effective dose limit of 100mSv in any period of five consecutive years (i.e., average of 20mSv per year) subjected to a maximum effective dose of 50mSv in any single calendar year for an employee aged 18 years and above and 6mSv for a trainee under the age of 18 years. An effective dose limit of 13mSv for a pregnant female at risk of occupational exposure to ionizing radiation in any consecutive period of 3 months during the gestation and 1mSv for any person other than an employee or trainee, including person below the age of 16 years [16].
Ominously, studies across the country reported significant level of exposure of radiation employees to ionizing radiation [17,18], although it is largely below the limits recommended by the NNRA [12], poor knowledge of basic principles of radiation protection and radiation dose received by patients was observed among healthcare professionals [19–21]; this implies that the situation could worsen in the near future.
Also, the previous studies across Nigeria were essentially focused on assessment of knowledge of radiation protection and radiation exposure status of employees, but sufficient attention was not paid to determination of their baseline clinical status, considering the fact that occupational health services in the country is still rudimentary. This could make an objective assessment of effects of occupational exposure to radiation among the employees impossible in the years to come, in addition to the professional and legal implications of such omissions.
Assessment of baseline knowledge of radiation hazards and radiation protection practices of special groups at risk is essential in designing appropriate strategies for the prevention of unnecessary exposure to ionizing radiation not only among health workers but their patients also. Similarly, assessment of the clinical profile of health worker at risk would be invaluable in detecting adverse health effects of radiation exposure, in addition to providing a baseline for comparison with the results of subsequent periodic examinations. This study, therefore, aimed to assess the knowledge of radiation hazards, radiation protection practices and clinical profile of health workers in UDUTH, Sokoto, Nigeria.
Materials and Methods
This cross-sectional study was conducted at the Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria, from September 2013 to December 2013. The hospital serves the inhabitants of Sokoto state, neighboring states in North-Western Nigeria, and people from neighboring Niger Republic. Out of the 24 departments that provide clinical services in the hospital, health workers from the 3 departments that use ionizing radiation (radiology, radiotherapy and dentistry) were considered to be at high risk of occupational exposure, and all those that consented to participate were enrolled into the study.
A standardized, semi-structured, self- and interviewer-administered questionnaire was prepared, validated and used to obtain information on socio-demographic characteristics, knowledge of radiation hazards/personal protective devices and radiation protection practices of participants. Evaluation of face and content validity of the questionnaire was done by a team of experts that comprised of 4 Senior lecturers, 2 Assistant Professors and 2 Professors from the Department of Community Medicine and Department of Radiology of UDUTH, Sokoto. The relevance of each of the items on the questionnaire was rated on a 4-point Likert scale (1= Not relevant; 2 = Somewhat relevant; 3 = Quite relevant; 4 = Highly relevant). The Content Validity Index for items (I-CVI) was computed as the proportion of experts giving a rating of either 3 or 4 [22]. Items on the questionnaire with I-CVI of 0.88 were retained. Content Validity Index for scales (S-CVI) was computed as the proportion of items on the questionnaire that achieved a rating of 3 or 4 by the content experts [23]. A Content Validity Index for scales (S-CVI) of 0.92 was obtained. The reference values used for assessment of knowledge of radiation exposure were based on the recommendations of the ICRP [11] and NBIRR [16]. The questionnaire was pretested among 10 healthcare workers in the Radiology Department of Specialist Hospital, Sokoto, Nigeria (another tertiary healthcare facility); appropriate modifications were done based on the observations made during the pretest. The instrument shows good internal consistency (Cronbach’s alpha = 0.81) and reliability (2 weeks test-retest correlation coefficient = 0.74). Three resident doctors assisted in questionnaire administration after being trained on conduct of survey research, the objectives of the study and questionnaire administration.
The clinical status of the participants was assessed by physical examination, chest X-ray, abdominal ultrasound and Complete Blood Count (CBC) estimation. The investigations were funded by the Management of UDUTH, Sokoto, as part of the radiation protection services of the hospital. Data on participants’ radiation exposure were extracted from the database of the Radiation Protection Unit of the hospital; the records covered a period of 4 years (from August 2009 to August 2013). Under the radiation protection services of the hospital, it is mandatory for health workers of the 3 departments with high risk of occupational exposure to ionizing radiation to consistently wear their Thermoluminescent dosimeter (TLD) badges while on duty. The TLD badges are sent to the Centre for Energy Research and Training, Ahmadu Bello University, Zaria, Nigeria, for processing and reporting quarterly (every 3 months). The Centre in turn sends the results of the processed TLD badges with equal number of annealed badges back to the hospital quarterly (every 3 months). The reference values used for assessment of radiation exposure were also based on the recommendations of the ICRP and NBIRR [11,16].
Institutional ethical clearance was obtained from the Ethical Committee of UDUTH, Sokoto, Nigeria. Permission to administer the questionnaires was obtained from the management of the hospital and the heads of the respective departments, while informed consent was also obtained from all the participants.
Data were analysed using IBM SPSS version 20.0 computer statistical software package. Participants’ responses to the 8 statements used to assess knowledge of radiation hazards were scored and graded. One point was awarded for a correct response, while wrong response or non-response attracts no point. This gives a minimum score of ‘0’ and a maximum score of ‘8’ points. Participants that scored > 5 of 8 points were considered as having ‘good’ knowledge, while those that scored < 5 of 8 points were graded as having ‘poor’ knowledge.
Similarly, participants’ knowledge of Personal Protective Devices (PPDs) was scored and graded on a 5-item scale. One point was awarded for a correct response, while wrong response or non-response attracts no point. This gives a minimum score of ‘0’ and a maximum score of ‘5’ points. Participants that scored ≥ 3 of 5 points were considered as having ‘good’ knowledge, while those that scored <3 of 5 points were graded as having ‘poor’ knowledge. In order to obtain an unbiased assessment of radiation protection practices, the study participants were briefed on the objectives of the study and the need to give true responses on what they do. In addition, the questionnaires were administered to them while on duty; those who reported consistent use of dosimeter (TLD) badge were inspected on the spot for verification. The proportion of participants that reported consistent use of dosimeter (TLD) badge that were found wearing them at the time of questionnaire administration was used as indicator for the assessment of validity of self-reported radiation protection practices.
The chi-square test was used for bivariate analysis involving categorical variables. Logistic regression analysis was used to determine the variables that predict good knowledge of radiation hazards. All levels of significance were set at p < 0.05.
Results
All the questionnaires administered to the 110 participants who gave their consent to participate in the study were found to be complete and analysed. The participants were aged 20 to 65 years (mean = 34.04±8.83), and majority of them were in the second (35.5%) and third (41.8%) decades of life. Most of the participants were males (67.3%), married (66.3%) and practiced Islam as religion (70.9%). The Department of Radiology had the largest proportion of participants (42.7%), and the predominant cadres were doctors (21.8%) and ward assistants (21.8%). Almost all the participants (95.5%) have been in practice for less than a decade as shown in [Table/Fig-1].
Socio-demographic profile of participants.
| Characteristics | Frequency (%)n = 110 |
|---|
| Age groups (in years) |
| 20 – 29 | 39 (35.5) |
| 30 – 39 | 46 (41.8) |
| 40 – 49 | 18 (16.4) |
| 50 – 59 | 4 (3.6) |
| 60 and above | 3 (2.7) |
| Sex |
| Male | 74 (67.3) |
| Female | 36 (32.7) |
| Marital status |
| Single | 34 (30.9) |
| Married | 73 (66.4) |
| Widowed | 3 (2.7) |
| Religion |
| Islam | 78 (70.9) |
| Christianity | 29 (26.4) |
| Others | 3 (2.7) |
| Department |
| Radiology | 47 (42.7) |
| Radiotherapy | 38 (34.5) |
| Dentistry | 25 (22.7) |
| Cadre |
| Doctor | 24 (21.8) |
| Nurse | 20 (18.2) |
| Imaging scientist | 12 (10.9) |
| Radiographer | 8 (7.3) |
| Physicist | 3 (2.7) |
| Biomedical engineer | 2 (1.8) |
| Medical records staff | 8 (7.3) |
| Administrative staff | 9 (8.2) |
| Ward assistant/cleaner | 24 (21.8) |
| Length of practice (in years) |
| 1 – 9 | 105 (95.5) |
| 10 – 19 | 5 (4.5) |
Knowledge of Radiation Hazards among Participants
Although majority, 85 (77.3%) participants were aware that exposure to ionizing radiations could cause harm to the body or result in sickness, only 65 (59.1%) had good knowledge of radiation hazards. The radiation hazards most commonly known to the participants included congenital malformations in babies of exposed pregnant women (68.2%) and infertility in exposed men and women (67.3%). While half to two-thirds of participants knew the others radiation hazards, less than half of participants (49.1%) knew that exposure to ionizing radiation could lead to death [Table/Fig-2]. The proportion of participants with good knowledge of radiation hazards was significantly higher among males (79.4%) compared to females (55.6%), χ2= 5.341, p = 0.021. Similarly, a significantly higher proportion of professionals such as doctors, nurses and imaging scientists among others (81.4%) had good knowledge of radiation hazards compared with administrative and other supporting staff such as medical records staff, ward assistants and cleaners (35.0%), χ2= 15.176, p < 0.001. Noticeably, there was no association between good knowledge of radiation hazards and length of practice, and no predictor of good knowledge of radiation hazards was obtained on logistic regression analysis.
Knowledge of radiation hazards among participants.
| Variables | Correct response (%)n = 110 |
|---|
| Which of the following do you know as radiation hazards (i.e., harm to the body or sickness due to exposure to ionizing radiations)? | |
| Acute radiation sickness such as nausea and vomiting | 62 (56.4) |
| Skin injuries such as erythema, skin pigmentation, dermatitis, hair loss and skin desquamation | 71 (64.5) |
| Cataract of the eye lens | 59 (53.6) |
| Bone marrow depression | 67 (60.9) |
| Infertility in men and women | 74 (67.3) |
| Congenital malformations in babies delivered by pregnant women exposed to ionizing radiations | 75 (68.2) |
| Cancers such as skin cancer, leukaemia etc. | 70 (63.6) |
| Death | 54 (49.1) |
| Grading of participants’ knowledge of radiation hazards | Frequency (%) |
| Good | 65 (59.1) |
| Poor | 45 (40.9) |
Participant’s Knowledge of Dose and Device for Measuring of Radiation Exposure
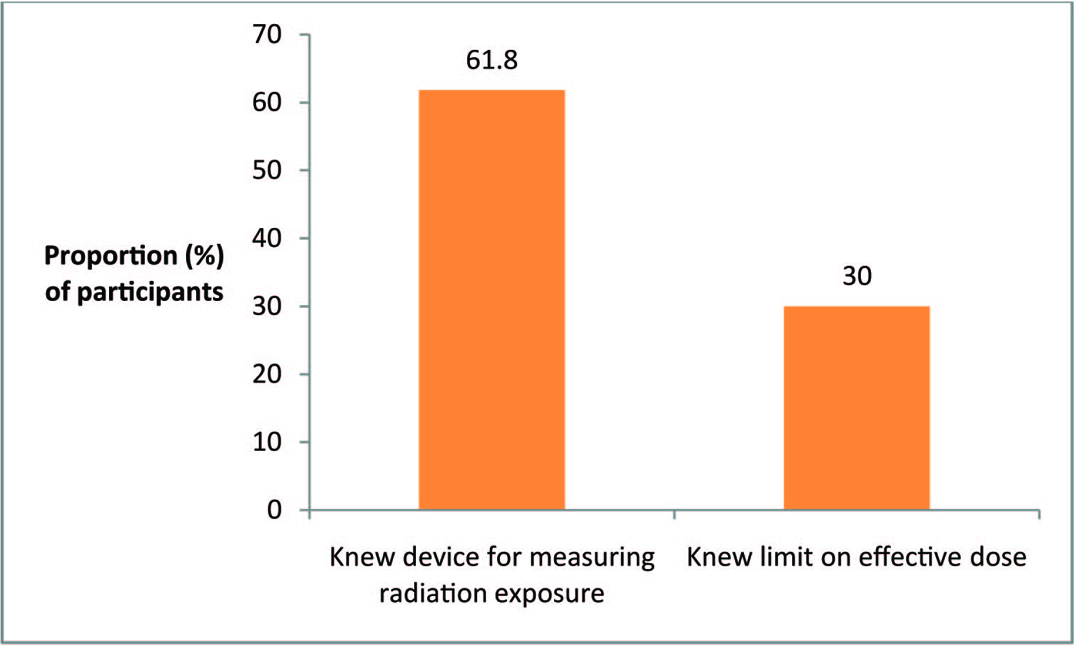
While 68 (61.8%) participants knew dosimeter as the device for measuring radiation exposure, only 33 (30.0%) knew that the limit on effective dose of ionizing radiation for a radiation worker aged 18 years and above in any single calendar year is 20mSV [Table/Fig-3]. Knowledge of device for measuring radiation exposure or limit on effective dose of ionizing radiations was not associated with the socio-demographic characteristics of participants.
Participants’ knowledge of dose and monitoring of radiation exposure.
Participant’s Knowledge of Personal Protective Devices for Reducing Radiation Exposure
Even though majority, 86 (78.2%) participants were aware of protective devices that can be worn to reduce exposure to ionizing radiation, only 58 (52.7%) had good knowledge of the various Personal Protective Devices (PPDs). While most of the participants knew lead apron as a PPD for reducing radiation exposure, just about half or less than half of the participants knew the other PPDs such as lead goggles (51.8%), lead gloves (51.8%), thyroid shields (43.6%) and gonad shields. (46.4%) as shown in [Table/Fig-4]. The proportion of participants with good knowledge of PPDs was significantly higher among males (74.24%) compared to females (50.0%), χ2 = 3.889, p = 0.049; and among those that were married (80.8%) compared to the singles (50.0%), χ2 = 8.775, p = 0.003, but no predictor of good knowledge of PPDs was found on logistic regression analysis.
Participants’ knowledge of Personal Protective Devices (PPDs).
| Variables | Correct response (%)n = 110 |
|---|
| Which of the following do you know as a personal protective device for reducing radiation exposure? | |
| Lead goggles | 57 (51.8) |
| Lead apron | 79 (71.8) |
| Lead gloves | 57 (51.8) |
| Thyroid shield | 48 (43.6) |
| Gonad shields | 51 (46.4) |
| Grading of participants’ knowledge of PPDs | Frequency (%) |
| Good | 58 (52.7) |
| Poor | 52 (47.3) |
Participant’s Attitude, Risk Perception and Protective Practices
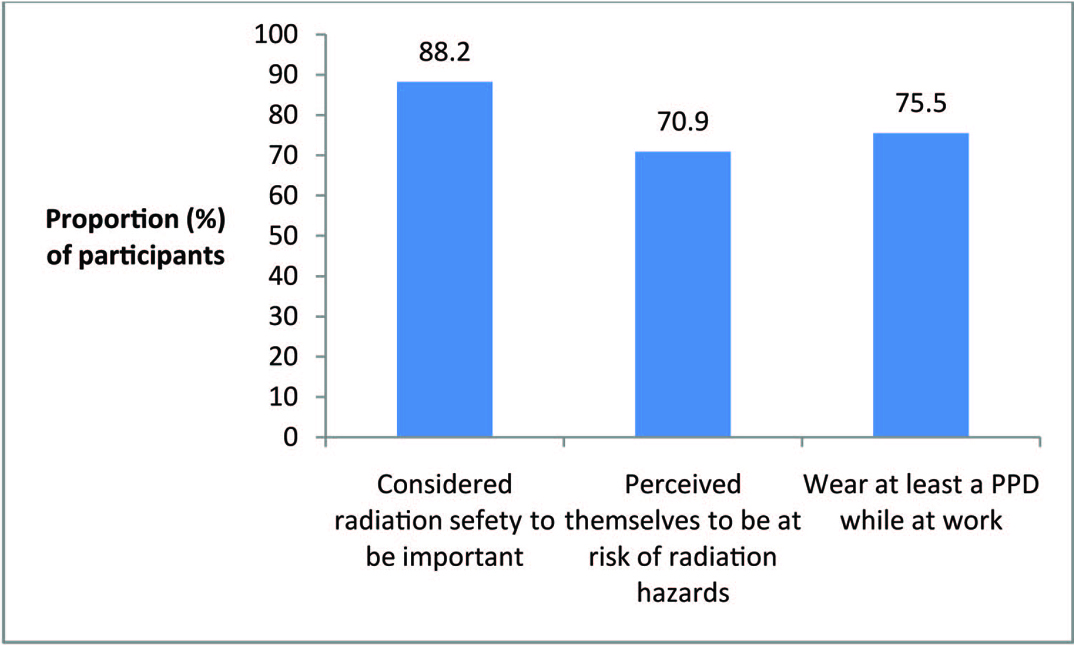
Ninety seven participants (88.2%) considered radiation safety to be important, and majority of participants (70.9%) perceived themselves to be at high risk of occupational exposure to radiation hazards. While a large proportion of participants (75.5%) reported wearing at least a type of PPD while at work to prevent exposure to radiation hazards [Table/Fig-5], consistent use of the various PPDs and dosimeter (TLD badge) was alarmingly low [Table/Fig-6]. On inspection,all the 30 participants (100%) that reported consistent use of dosimeter (TLD) badge were found wearing them at the time of questionnaire administration.
Participants’ attitude, risk perception and radiation protection practices.
Consistent use of PPDs and dosimeter by participants.
| Items | Consistent use (%)n = 110 |
|---|
| Lead goggles | 5 (4.5) |
| Lead apron | 12 (10.9) |
| Lead gloves | 5 (4.5) |
| Thyroid shield | 3 (2.7) |
| Gonad shields | 5 (4.5) |
| Dosimeter (TLD) badge | 30 (27.3) |
Level of Radiation Exposure and Clinical Profile of Participants
The cumulative exposure over a period of 4 years for the participant with the minimum exposed dose was 0.19mSV; this was equivalent to an average annual exposure of 0.0475mSv. Also, the cumulative exposure over a period of 4 years for the participant with the maximum exposed dose was 7.49mSv; this is equivalent to an average annual exposure of 1.8725mSv.
The prevalence of abnormal clinical findings was very low among the participants. Only 1 (1.2%) of 86 participants had an abnormal finding on chest X-ray (enlarged thyroid gland). Also, 8 (9.4%) of 85 participants had abnormal abdominal ultrasound findings; of these, 4 (50.0%) had only fatty liver, while 1 (12.5%) each had fatty liver / splenomegaly, cholecystitis, uterine fibroid, and dilated aortic artery. Hematological tests also show that 17 (15.5%) and 11 (10.0%) of 110 participants had anemia and leucopenia respectively as shown in [Table/Fig-7].
Clinical profile of participants.
| Type of examination | Normal findingsFrequency (%) | Abnormal findingsFrequency (%) |
|---|
| Chest X-ray (n = 86) | 85 (98.8) | 1 (1.2) |
| Abdominal ultrasound (n = 85) | 77 (90.6) | 8 (9.4) |
| Hematological tests (n =110) | | |
| *Hb concentration | 93 (84.5) | 17 (15.5) |
| *WBC count | 99 (90.0) | 11 (10.0) |
Discussion
A large proportion (59.1%) of the participants in this study demonstrated good knowledge of radiation hazards. This finding is consistent with that obtained in a study conducted in three hospitals in Port Harcourt, Nigeria, in which 58.7% of radiographers were aware of the dangers of ionizing radiation [24]. On the contrary, Famurewa et al., reported poor level of awareness of the basic principles of radiation protection and patients’ exposure in a study among doctors in Ile-Ife, Nigeria [19], while Booshehri et al., reported poor knowledge of radiation protection among dentists in Yazd dental office [8]. This could affect their risk perception of radiation hazards and by extension their compliance with radiation protection practices.
Whereas, awareness of dosimeter as the device for measuring radiation exposure was high among the participants, less than a third (30.0%) knew the limit on effective dose of ionizing radiation for a radiation worker. This is of serious concern because they could develop complacent attitude towards radiation safety challenges at work, more so that studies conducted among various specialties of health workers demonstrated poor knowledge of radiation dose imparted during common radiological procedures and the consequent risk to themselves and their patients [25–29]. A major concern about the prevalent underestimation of radiation dose exposures in these studies was exposure of patients to increasing radiological investigations and the attendant radiation hazards.
Despite high level of awareness (78.2%), only about half (52.7%) of the participants knew the various personal protective devices (PPDs) that can be worn to reduce exposure to ionizing radiation. Although, most of the participants demonstrated positive attitude towards radiation safety (88.2%) and perceived themselves to be at risk of occupational exposure to radiation hazards (70.9%), consistent use of the various PPDs and dosimeter (TLD badge) was alarmingly low. However, the fact that all the 30 participants (100%) that reported consistent use of dosimeter (TLD) badge were found wearing them at the time of questionnaire administration suggests high validity of self-reported radiation protection practices. Although use of PPDs was low in this study, it is far better than the finding in a study conducted in different hospitals in Nepal, in which around 65% of the radiation workers studied have never been monitored for radiation exposure, and there was no quality, control program in any of the surveyed hospitals [30]. The reverse is true of the findings in a study by Mojiri et al., that reported high awareness of necessity of application of film badges (70%) and periodic examination (63%) among the participants; as well as application of protective devices for themselves (83.1%) and their patients (78.9%) [31].
In another study, among invasive cardiologists [32], whereas almost all the participants (93%) consistently used lead apron, less than half of them used other radiation protective measures including thyroid collar and lead eye glasses; and only 7% regularly utilized a radiation dose badge to monitor their exposure to ionizing radiation. This was attributed to the fact that while lead apron was available, the other devices were available to less than a third of participants.
The level of radiation exposure was low among the participants in this study. This finding is in concordance with the reported low level of radiation exposure among radiation staff of Lagos University Teaching Hospital [18], and the relatively low whole body doses of radiation exposure among occupationally exposed workers in Nigeria [17]. The study also reported that, the mean annual radiation exposure of all radiation workers in Nigeria increased from 3.6mSv in 1999, to 4.7mSv in 2000, and 7.7mSv in 2001 [17]. These findings and the increasing utilization of ionizing radiation for diagnostic and interventional purposes in the health facilities across Nigeria, reaffirm the need to contain the budding problem of radiation exposure hazards in the country.
The prevalence of abnormal clinical findings was very low among the participants in this study, this is reassuring and it elucidates the importance of a functional occupational health service in radiation hazards prevention in addition to providing baseline information for ascertaining development of diseases related to occupational exposure to ionizing radiation in the respective workers later in life, even after retirement from service. Reports from studies across the globe (including China, United States and Britain) had established strong links between some cancers and occupational exposure to ionizing radiations among health workers. A study among medical X-ray workers in China reported significant cancer risk (Relative Risk (RR) = 1.2, 95% Confidence Interval (CI) = 1.1 – 1.3). Significantly elevated risks were found for leukaemia and cancers of the skin, female breast, lung, liver, bladder, esophagus and thyroid [33].
Another study in the United States reported higher risk for breast cancer (RR = 2.92, 95% CI = 1.22 – 7.0) among radiologic technologists first employed prior to 1940, compared to those first employed in 1960 or later, and the risks declined with more recent calendar year of first employment irrespective of employment duration [34]. Similarly, a study that examined the mortality pattern among British radiologists over a period of 100 years (1897 – 1997) reported that among those who registered before 1950, there was 41% excess risk of cancer mortality among those registered for more than 40 years (SMR = 1.41, 95% CI = 1.03 – 1.90), and there was no evidence of an increase in cancer mortality among radiologists who first registered after 1954 [35]. These findings may not be unconnected with the improvement in radiation hazards preventive practices in the respective countries where the studies were conducted in recent years, and they provide strong evidence in support of the fact that, to guarantee the health and safety of workers at risk of occupational exposure to ionizing radiation in Nigeria, full compliance with radiation safety regulations is sacrosanct.
Limitation
The probability of deliberate mis-information by the participants makes an unbiased assessment of their radiation protection practices difficult despite the measures taken. Also, the records of findings of the pre-employment medical examination done for the respective participants at the time of engagement were unavailable for comparison with the findings obtained in this study, this makes it difficult to attribute the abnormal findings observed among the participants to their workplace exposure.
Conclusion
This study demonstrated poor radiation protection practices despite good knowledge of radiation hazards among the participants, but radiation exposure and prevalence of abnormal clinical conditions were found to be low. There is therefore need for periodic in-service training and regular monitoring of occupationally exposed health workers to ensure compliance with radiation safety regulations.