Introduction
Chronic Kidney Disease (CKD) is becoming a major public health problem worldwide. The very diagnosis of CKD brings a plethora of psychological problems that adds to the agony of the debilitating illness. Financial difficulties apart from the excruciating physical burden of the disease, owing to series of psychosocial issues. Anxiety and depression are two major concerns that to be managed effectively to sustain the life of people undergoing Haemodialysis.
Aim
The study aimed at finding the effect of Cognitive Behaviour Therapy (CBT) on anxiety and depression among people undergoing haemodialysis.
Materials and Methods
An experimental approach with Randomized controlled trial design was adopted for the study. The instruments used for data collection were Background Proforma and Hospital Anxiety and Depression Scale (HADS). A total of 150 subjects undergoing haemodialysis in a tertiary care hospital of South Karnataka were screened for inclusion and exclusion criteria and 80 participants were recruited for the study. Through computerized block randomization 40 each were allotted to experimental and control groups whereas 33 and 34 respectively in both the groups completed the study. CBT, a structured individual therapy of cognitive, behavioural and didactic techniques, with 10 weekly sessions each was administered to the experimental group. Non-directed counseling, a psychological intervention with ten weekly sessions of individual counseling was given to the control group.
Results
The findings of the study revealed that there was a significant reduction of mean anxiety (F=76.739, p=0.001) and depression (F=57.326, p= 0.001) in the experimental group when compared with the control group.
Conclusion
Researchers concluded that CBT can be effectively utilized for people undergoing haemodialysis in order to obtain control over their negative thoughts thereby reducing anxiety and depression.
Introduction
As per WHO Global burden of disease project, diseases of the kidney and urinary tract contribute to the global burden with approximately 8,50,000 deaths every year [1]. CKD is a global threat to health in general and for developing countries in particular, because therapy is expensive and life-long. In India 90% of the patients cannot afford the cost [2] and care for kidney disease is available only at the higher-level hospitals. There is no formal referral system; patients can go to any hospital, including to referral hospitals anywhere in the country. A shortage in the number of publicly funded specialized hospitals forces patients to seek care in expensive private hospitals. A vast majority do not have access to health insurance, and hence, have to fund treatment from their resources [3].
The patients with an end stage renal failure will virtually face complications in every organ system and the commonly encountered psychiatric complications are depression, anxiety, dementia, delirium, coping difficulties and marital or family problems. There are numerous sources of severe psychological stress, including chronic fatigue, other physical symptoms, excessive dependence on other people, loss of previous social functioning and difficulties in maintaining hope in the face of uncertain future. These problems along with stress related to the health status, social relationships and social and vocational functions often show profound quality of life complications [4].
CKD leads to many physiological and cognitive problems due to metabolic abnormalities, toxic condition from organ failure and major lifestyle changes brought about by ongoing haemodialysis treatment and related complications. Maintaining quality of life, adjusting to haemodialysis, coping with chronic depression and hopelessness are common concerns of individuals with CKD. The treatment regimen demands may be overwhelming for a debilitated patient and further reduce the role functioning within the family. Also, severe fluid and dietary restrictions further increase discomfort and frustration with the disease [5].
Devi et al., interviewed 50 dialysis patients from Kasturba Hospital at Udupi District, Karnataka, India and identified a list of 27 problems which were commonly experienced by them. Majority of the patients (94%) experienced weakness after haemodialysis, 92% had worries about the possible complications and 88% had fear about being not able to work as before. Sleep disturbance was experienced by 78% of patients, 74% of them felt frustrated with their dependency. Most of them felt lack of interest in living (68%), easily annoyed (68%) and felt rejected because of the physical limitations (66%) [6].
A phenomenological study on the experience of people undergoing haemodialysis with their illness revealed 10 themes such as loss of hope, physical limitations, restriction, financial burden, lack of support, feelings towards the machine, search for hope and betterment, spirituality, marital relationship and uncertainty and fear about tomorrow. The detailed explorations of patients’ experience showed that the illness caused paraphernalia of problems in most of their life areas. Hence, the people undergoing haemodialysis are in need of a tailor made, sound psychological intervention that can help them to adapt with demands and restrictions of CKD and dialysis [7].
Anxiety and depression are common co-morbid conditions with any chronic medical illness and hence, they are the important targets of psychological assessment in patients diagnosed with CKD because it predicts the patient’s morbidity, mortality and poor quality of life [8,9]. There is a dearth of well-designed studies in the field of haemodialysis especially on the effect of psychological interventions in alleviating the anxiety and depression among this population in India. Considering the myriad psychological symptoms and psychosocial concerns of these people, researchers have attempted to test the effect of a structured, time limited and scientific intervention to achieve the set outcome, that is reduction in the mean scores of anxiety and depression in the immediate post intervention as well as follow-up periods.
Aim
Therefore, study aimed at finding the effect of CBT on anxiety and depression among people undergoing haemodialysis.
Materials and Methods
The design adopted for the study was Randomized Controlled Trial (RCT) and registered in the Clinical Trial Registry of India (CTRI) under Indian Council of Medical Research with the number CTRI/2015/10/006253. The sample size was calculated based on the pilot study results and the required sample was 33 in each group. Considering 20% attrition, it was decided to take 40 each in experimental and control group and at the end 33 and 34 participants respectively in both the groups completed the study. The schematic presentation of the study design is developed according to the CONSORT statement 2010 [10] and presented in [Table/Fig-1].
Study design as per the CONSORT guidelines, 2010

Ethical clearance for the conduction of the study was obtained from the Institutional Ethics Committee and administrative permissions obtained from Medical Superintendent and Head of the Department. Written informed consent from the participants was taken prior to data collection. The participants for the study were CKD patients undergoing maintenance haemodialysis in the dialysis unit of a selected tertiary care hospital at Manipal. Eighty subjects were selected based on inclusion and exclusion criteria. The inclusion criteria for the participants were age between 20 and 65 years, on maintenance dialysis for a minimum period of one year, who can read and write Kannada or English, scores above 7 in any of the areas of anxiety or depression on the Hospital Anxiety and Depression Scale (HADS) [11] and willing to participate. Those who required full support for ambulation, waiting for transplant, diagnosed or on treatment for any of the psychiatric illness or received any form of psychotherapy, had significant vision or hearing impairments, were excluded from the study.
Further the entire samples were randomly allocated into experimental and control groups by using computer generated random order and block randomization procedure. The study was single blinded as the investigators only knew about who got which intervention whereas the study participants were not aware about the exact difference between the two psychological interventions; CBT and non-directive counselling.
The experimental group received CBT whereas the subjects in the control group received non-directive counseling while both the groups were receiving routine care. The observations were phased into three times; pre-assessment, after the therapy at three months and after six months.
Background Proforma and Hospital Anxiety and Depression Scale (HADS) which is a standardized scale to assess the anxiety and depression were used for data collection. The Background Proforma was developed by the researchers and validated by seven experts from the fields of nephrology, dialysis technology and medical surgical nursing. It had a total of 17 items on both demographic and clinical profile of the patients. HADS was developed by Zigmond and Snaith in the year 1983 [11]. This scale was specifically developed for use with physically ill patients [12]. Cronbach’s alpha for HADS-A varied from 0.68 to 0.93 (mean 0.83) and for HADS-D from 0.67 to 0.90 (mean 0.82). The sensitivity and specificity for both HADS-A and HADS-D of approximately 0.80. Pretesting of the Kannada version was done among five people undergoing haemodialysis, followed by the reliability checking among 20 patients and Cronbach’s alpha value obtained for the HADS was 0.73 and hence, it was considered reliable to be used in the study.
The researchers developed and validated CBT module for the people undergoing haemodialysis among clinical psychologists, psychiatric nurses, dieticians and other related area experts. The final module contained 10 weekly sessions, each with duration of 50 to 60 minutes. The CBT utilized cognitive, behavioural and didactic techniques in order to change the dysfunctional thoughts and behaviour and negative feelings of the people undergoing haemodialysis.
Results
SPSS version 16.0 was used for the statistical analysis. Chi-square and Fisher’s-exact test were computed to check the homogeneity of the two groups with respect to outcome variables and demographic variables among the people undergoing haemodialysis and thus, the two groups were considered equal. Majority of the participants, 66.67% and 64.71% (p=0.535) were in 43 to 65 years of age, males 69.7% and 70.59% (p=0.936) and Hindus 78.79% and 76.47% (p=0.969) in the experimental and control group respectively. The participants in the experimental group had education up to pre-degree (36.37%) whereas many of them (35.29%) in the control group had a better education; up to diploma or graduation (p=0.301).
Majority of the people undergoing haemodialysis were unable to attend a paying job (78.79% and 67.65%) whereas most of them in both the groups were non-professionals in the past (36.37% and 29.41%, p=0.66). Majority of the people undergoing haemodialysis were married (78.79% and 79.41%, p=0.809) and living with four to six family members (75.76% and 79.41%, p=0.39) in the experimental and control group respectively. Nearly half of the participants in both the groups (51.52% and 50%, p=0.678) had a family income of rupees 5001 to 10,000. Nearly half of the sample in experimental and control groups have stated that their CKD diagnosis revelation was sudden {57.58% and 55.88% (p=0.332)}.
The [Table/Fig-2] presents the distribution of anxiety and depression among the people undergoing haemodialysis of the experimental and control groups and Independent sample t-test was computed to check the equality of groups.
Distribution of anxiety and depression among people undergoing haemodialysis.
| Outcome variables | Experimental | Control | t-value | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| AnxietyDepression | 10.7111.85 | 2.012.15 | 11.0011.21 | 2.382.53 | 0.5631.118 | 0.4100.482 |
n= 67 (33+34)
[Table/Fig-2] indicates that both the mean scores of anxiety 10.71± 2.01, 11± 2.37 (p=0.41) and depression 11.85±2.15, 11.21± 2.53 (p=0.48) were comparable in experimental and control group respectively and thus, the two groups were considered matched.
Effect of CBT on Anxiety
Based on the HADS scores, sample were categorized as having normal (score ranging from 0-7), borderline abnormal (8-10) and abnormal (11-21) anxiety across experimental and control groups over time and it is depicted in [Table/Fig-3].
Paired bar diagram showing the anxiety categories across groups over time
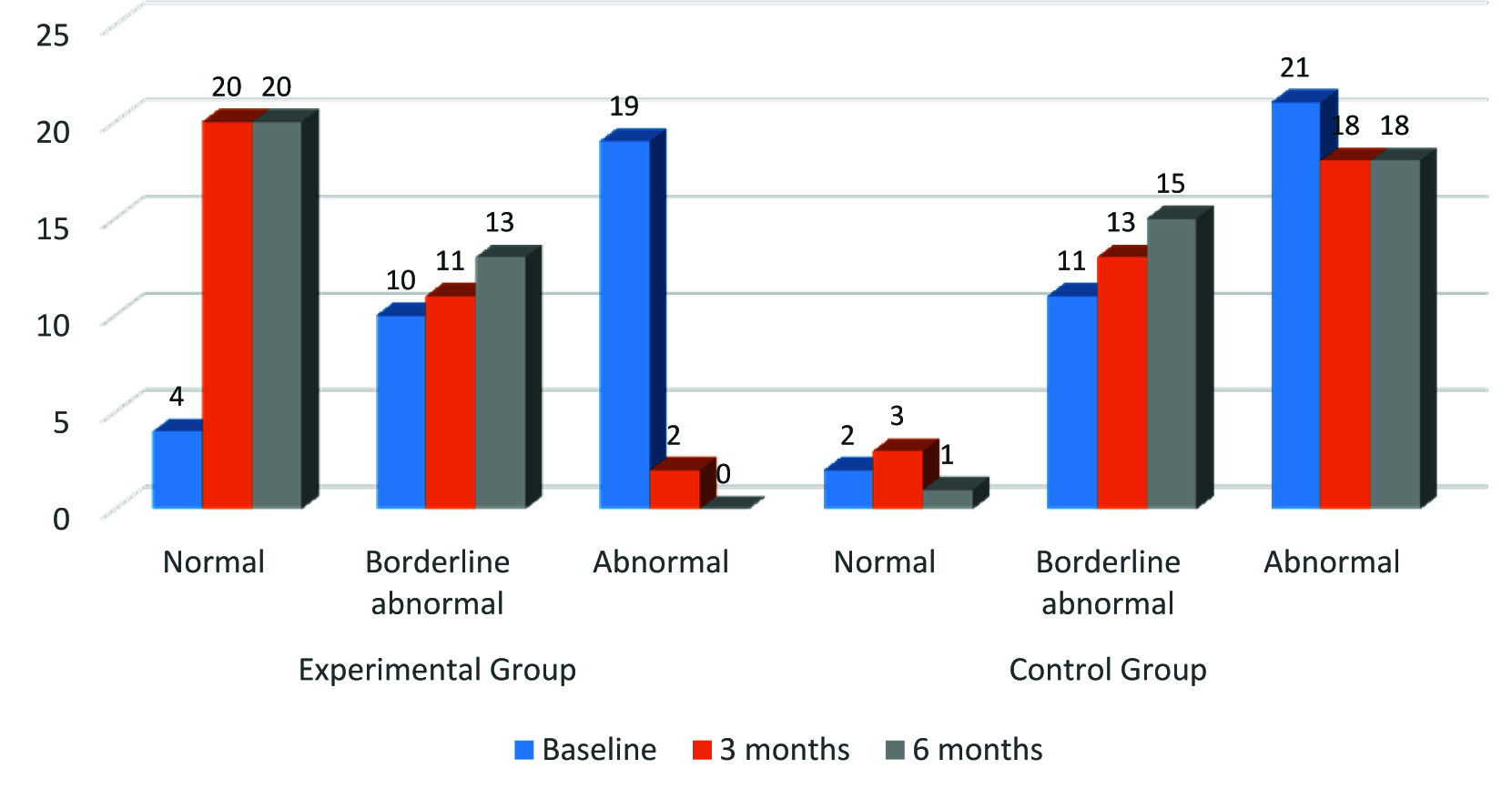
The data presented in the [Table/Fig-3] depicts that there was a considerable amount of reduction in the abnormal level of anxiety in the experimental group in the post intervention period; from 19 (51.58%) at baseline to 2 (6.06%) at third month and 0% at sixth month compared to the control group; from 21 (61.76%) at baseline to 18 (52.94%) at third month and sixth month.
The effect of CBT was tested at 0.05 level of significance with the null hypothesis: ‘there will be no significant difference in the mean pre and post test scores of anxiety and depression among people undergoing haemodialysis in the experimental and control group’. Repeated measure ANOVA is chosen as the appropriate inferential statistics in order to check the effect of CBT on anxiety and depression. The sphericity of the data was tested through Mauchly test, and the correction by Greenhouse-Geisser test was used.
Data presented in [Table/Fig-4] reveals that there was a significant reduction of mean anxiety scores in the experimental group (from 10.7 to 7.18 at 3 months and 7.09 at 6 months) when compared with the control group (from 11 to 10.68 at 3 months and 11.29 at 6 months) (F=76.739, p=0.001). The profile plot is shown in [Table/Fig-5].
Comparison of anxiety across groups over time using repeated measure ANOVA. n= 67 (33+34)
| Anxiety | Experimental Group | Control Group | df | f-ratio | 95%Confidence Interval | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| Baseline | 10.70 | 2.01 | 11.00 | 2.37 | 2,130 | 76.739 | 9.167-10.147 | 0.001 |
| 3 months | 7.18 | 1.88 | 10.68 | 2.36 |
| 6 months | 7.09 | 1.63 | 11.29 | 2.54 |
Profile plot showing mean Anxiety scores
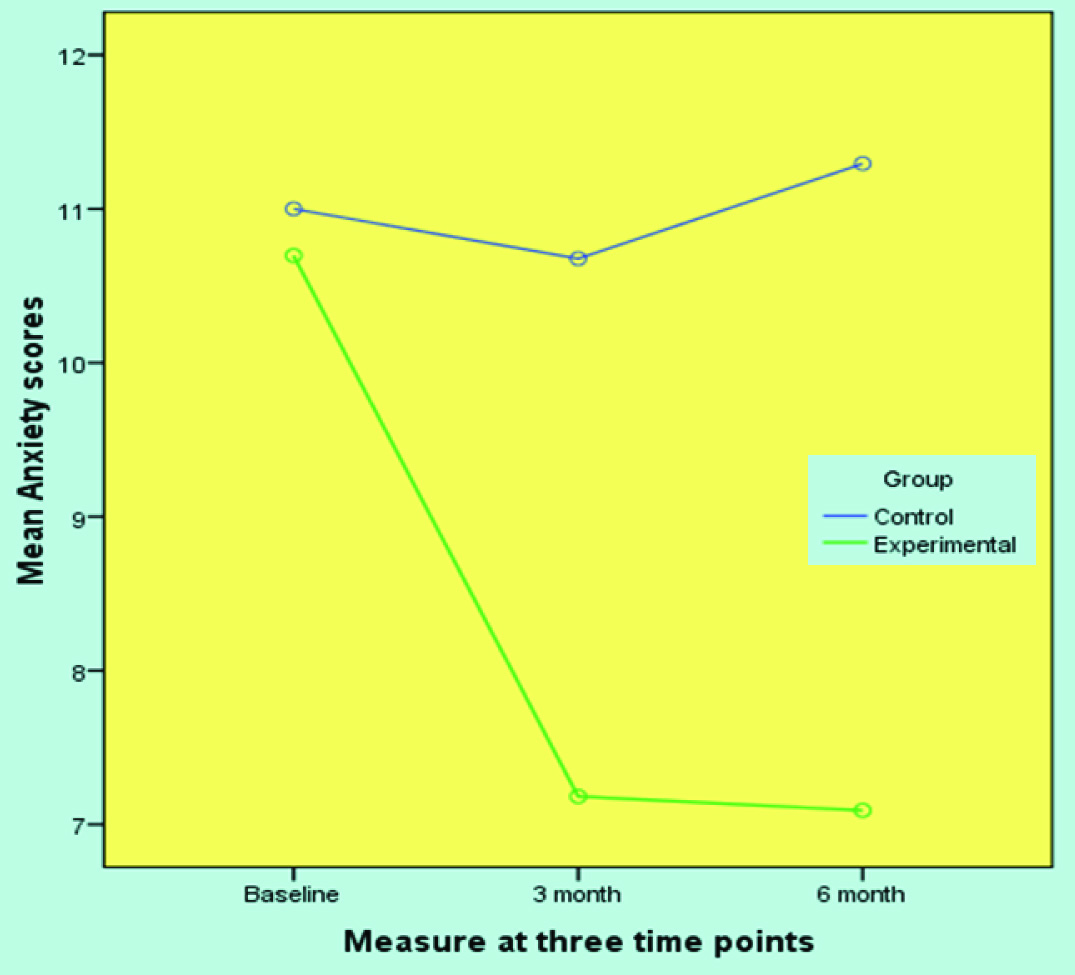
[Table/Fig-5] indicates that the reduction in the mean anxiety scores is higher among the experimental group.
Effect of CBT on Depression
The change in the depression categories across experimental and control group was visualized descriptively with the help of a paired bar diagram [Table/Fig-6].
Stacked bar diagram showing depression categories across groups.
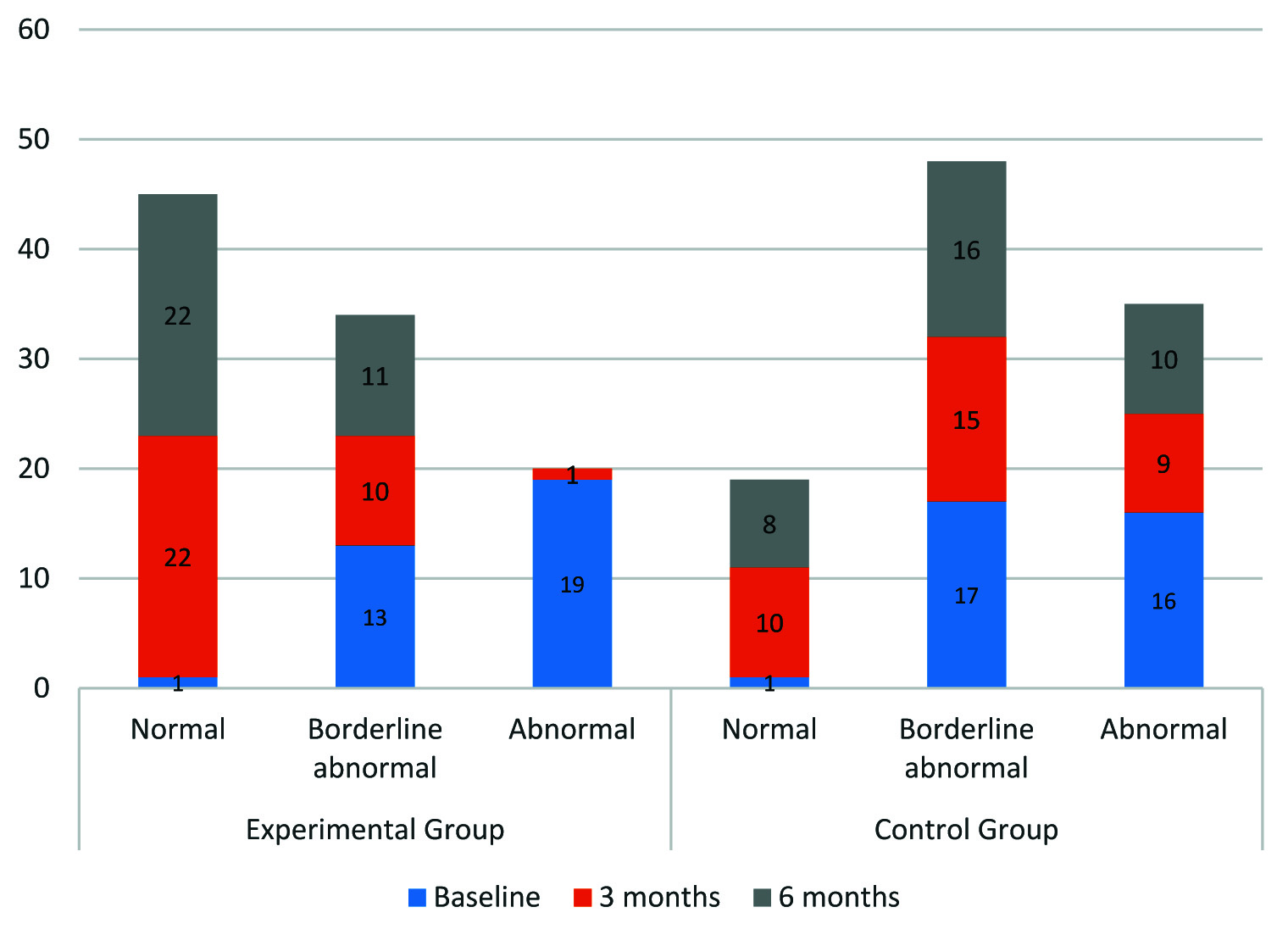
The [Table/Fig-6] depicts that there was a considerable amount of reduction in the abnormal level of depression in the experimental group in the post intervention period from 19 (51.58%) at baseline to 1 (3.03%) at third month and 0% at sixth month compared to the control group; from 16 (41.06%) at baseline to 9 (26.47%) at third month and 10 (29.41%) at sixth month.
The effect of CBT on depression was analysed using repeated measure ANOVA as presented in [Table/Fig-7].
Comparison of depression across groups over time using repeated measure ANOVA.
| Depression | Experimental Group | Control Group | df | F ratio | 95% CI | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| Baseline | 11.85 | 2.15 | 11.21 | 2.53 | 2,130 | 57.326 | 8.690-9.976 | 0.001 |
| 3 months | 6.82 | 1.86 | 9.21 | 2.69 |
| 6 months | 6.73 | 1.53 | 9. 74 | 2.71 |
n= 67 (33+34)
Data presented in [Table/Fig-7] shows that there was a reduction of mean depression scores in the experimental group (from 11.85 to 6.82 at third month and 6.73 at sixth month) when compared with the control group (from 11.21 to 9.21 at third month and 9.74 at sixth month follow up), F=57.326, at 0.001 level of significance. The repeated measure profile plot was shown in [Table/Fig-8].
Profile plot showing mean depression scores.
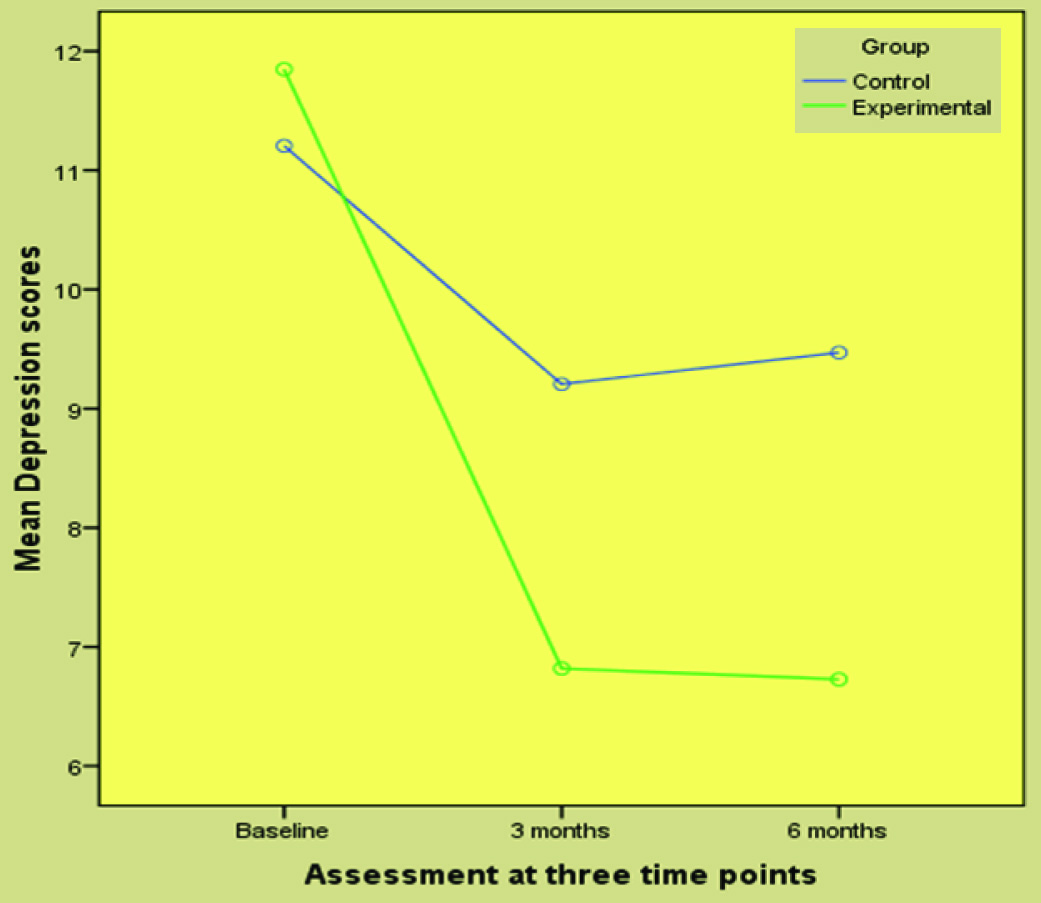
The [Table/Fig-8] shows that the fall in depression was consistently maintained by the intervention group over time.
The average reduction of mean scores of anxiety and depression in the experimental group was greater than the control group (p=0.001). This reduction was retained after six months of CBT. Hence, the H01 was rejected and it can be interpreted that the CBT was effective in bringing down the anxiety and depression among people undergoing haemodialysis.
Discussion
Present study categorized the people undergoing haemodialysis into three groups based on the scores on the Hospital Anxiety Depression Scale (HADS): normal (score ranging from 0-7), borderline abnormal (8-10) and abnormal (11-21) across experimental and control groups over time. There was reduction in the abnormal level of anxiety in the experimental group in the post intervention period; from 19 (51.58%) at baseline to 2 (6.06%) at third month and 0% at sixth month compared to the control group; from 21 (61.76%) at baseline to 18 (52.94%) at third month and sixth month. Repeated measures ANOVA showed significant reduction of mean anxiety scores in the experimental group (10.7 to 7.18 at 3 months and 7.09 at 6 months) when compared with the control group (from 11 to 10.68 at 3 months and 11.29 at 6 months) (F=76.739, p=0.001). This was indicative of the effect of CBT in contributing to clinically and statistically significant outcome in anxiety reduction. The increase of mean anxiety in the control group at six months could be due to their exposure to ongoing symptoms and stressors of the illness itself.
This result supports the finding of randomized controlled trial conducted by Hare, et al., that the CBT brought significant differences in HADS anxiety (t14=2.32; p=0.034) (t14=2.73; p=0.016) among the people undergoing peritoneal dialysis [13]. Matusiewicz, et al., reported participants in the experimental group after listening to a CD with a psychological intervention had reduction in the level of anxiety t(30)=2.99; p<0.05, a weaker intensity of cognitive appraisal of the treatment situation as a threat t(30)=3.48; p<0.05, a weaker intensity of cognitive appraisal of the situation as a harm/loss t(30)=2.75; p<0.05 and a stronger intensity of cognitive appraisal of the situation as a challenge t(30)=3.49; p<0.05 when compared with the control group [14].
In the current study, there was reduction in the abnormal level of depression in the experimental group in the post intervention period; 19 (51.58%) at baseline to 1 (3.03%) at third month and 0% at sixth month compared to the control group; from 16 (41.06%) at baseline to 9 (26.47%) at third month and 10 (29.41%) at sixth month. There was also reduction in the mean depression scores in the experimental group (from 11.85 to 6.82 at third month and 6.73 at sixth month) when compared with the control group (from 11.21 to 9.21 at third month and 9.74 at sixth month follow up), F=57.326, at 0.001 level of significance. CBT was found very effective in bringing down the depression scores of exposed group.
The current finding concur with Duarte et al., who reported significant reduction of BDI cognitive and somatic subscales and overall BDI mean scores at third and ninth month assessments (p<0.001) after CBT whereas the control group had substantially lower changes. Mini International Neuropsychiatric Interview (MINI) also found to be lower in the CBT group at third (p<0.001) and ninth month assessments (p=0.031). There was significant improvement in the risk of suicide, with in the intervention group after three and nine months (p=0.019 and p=0.002) whereas, no difference was observed in the control group [15]. Marvi et al., brought out the results that the experimental group had significant reduction in their depression scores in the post test, t=8.678 (p<0.001) [16].
In line with the present findings, Weiner et al., reported that the participants of CBT after attending a class on stress management (through communication and problem solving) showed significant improvement in depression scores {(56% only had depressed mood at follow-up against the initial 65%) (p<0.05)}, compared to the control group [17]. Cukor also found that the average BDI-II scores declined from 28.9 to 18.5 at the end of CBT and to 18.8 at a three month follow-up, indicating both a significant and sustained reduction in depression of heamodialysis patients [18]. Cukor et al., reported that the treatment-first group achieved significantly greater reductions in BDI II (p=0.03) and Hamilton Depression Rating Scale (p<0.001) scores after CBT [19]. The comparison of studies showed that CBT is effective intervention to bring down the anxiety and depression among the target population in a desirable way thus, the objective to check the effectiveness of CBT in this direction was achieved.
Limitation
The research had self-report measurements where there could be participant bias.
Conclusion
The authors concluded that the people undergoing haemodialysis suffer considerable amount of anxiety and depression. Further, it was concluded that the CBT is effective in reducing the anxiety and depression among people undergoing haemodialysis. Inclusion of certified mental health professionals in the CKD treating team and incorporating CBT as part of haemodialysis treatment will be a challenge especially for developing countries. Such initiatives and its cost effectiveness and feasibility can be tested in future studies.
n= 67 (33+34)
[1]. World Health Organisation. Burden of disease project available at: http://www.3.who_int/whosis/menu.cfm?path=evidence, burden & language accessed on August 2007 [Google Scholar]
[2]. Lysaght MJ, Maintenance dialysis population dynamics: Current trends and long-term implicationsJ Am Soc Nephrol 2002 13:S37-S40. [Google Scholar]
[3]. Jha V, Chugh KS, Dialysis in developing countries: Priorities and obstaclesNephrology 1996 2(2):65-71. [Google Scholar]
[4]. Yu BH, Dimsdale JE, Psychiatric and psychosocial complications in chronic dialysis. Lamerine N, Mehta RL editorsComplications of dialysis 2000 New YorkMarcel Dekker Inc [Google Scholar]
[5]. Barry PD, Psychosocial nursing, care of physically ill patients and their families 1996 PhiladelphiaLippincott [Google Scholar]
[6]. Devi ES, Prabhu R, Bhanumathi PP, Sequiera L, Mayya SS, Bairy KL, Identification of health problems of patients undergoing hemodialysis using self care deficit theory and application of nursing process approach careInternat J of Nurs Educ 2012 4(1):15-17. [Google Scholar]
[7]. Valsaraj BP, Bhat SM, Prabhu R, Dinesh N, A qualitative research on the experience of haemodialysis in South Karnataka: Lived experience of persons undergoing haemodialysisJKISMU 2014 3(2):90-100. [Google Scholar]
[8]. Kimmel PL, Thamer M, Richard CM, Ray NF, Psychiatric illness in patients with end stage renal diseaseAm J of Med 1998 105(3):214-21. [Google Scholar]
[9]. Dogan E, Erkoc R, Eryonucu B, Sayarliogu H, Agargun MY, Relation between depression, some laboratory parameters, and quality of life in hemodialysis patientsRen Fail 2005 27(6):695-99. [Google Scholar]
[10]. Schulz KF, Altman DJ, Moher D, CONSORT GroupCONSORT 2010 Statement: updated guidelines for reporting parallel group randomized trialsBMJ 2010 340:c332 [Google Scholar]
[11]. Zigmond AS, Snaith RP, The hospital anxiety and depression scaleActa Psychiatrica Scandinavia 1983 67(6):361-70. [Google Scholar]
[12]. Herrmann C, International experiences with the hospital anxiety and depression scale-a review of validation data and clinical resultsJournal of Psychosomatic Research 1997 42(1):17-41. [Google Scholar]
[13]. Hare J, Clark-Carter D, Forshaw M, A randomized controlled trial to evaluate the effectiveness of a cognitive behavioural group approach to improve patient adherence to peritoneal dialysis fluid restrictions: a pilot studyNephrol Dial Transplant 2014 29(3):555-64. [Google Scholar]
[14]. Matusiewicz KB, Green AT, Kozowska A, The influence of psychological intervention on cognitive appraisal and level of anxiety in dialysis patients: a pilot studyThe Open Nutraceuticals Journal 2011 4:61-64. [Google Scholar]
[15]. Duarte PS, Miyazaki MC, Blay SL, Sesso R, Cognitive-behavioural group therapy is an effective treatment for major depression in hemodialysis patientsKidney Int 2009 76(4):414-21. [Google Scholar]
[16]. Marvi A, Bayazi MH, Rahmani M, Deloei AK, Studying the effect of cognitive behavioural group training on depression in hemodialysis patientsProcedia-Social and Behavioural Sciences 2011 30:1831-36. [Google Scholar]
[17]. Weiner S, Kutner NG, Bowles T, Johnstone S, Improving psychosocial health in hemodialysis patients after a disasterSoc Work Health Care 2010 49(6):513-25. [Google Scholar]
[18]. Cukor D, Use of CBT to treat depression among patients on hemodialysisPsychiatric Services 2007 58(5) [Google Scholar]
[19]. Cukor D, Halen NV, Asher DR, Coplan JD, Weedon J, Wyka KE, Psychosocial intervention improves depression, quality of life, and fluid adherence in hemodialysisJ Am SocNephrol 2014 25:196-206. [Google Scholar]