Health of woman is one of the major health challenges across the world. At present, the high and unacceptable level of maternal mortality is a common issue of global health and development [1]. Maternal mortality during pregnancy, birth, and up to 42 days after termination of pregnancy for any reason other than accidents is considered as the maternal mortality caused by pregnancy and birth complications [2]. Death of a mother causes irreversible damages to a family and a society [3]. Birth and pregnancy complications led to the 16.0 deaths per 100,000 live births in United States from 2006 to 2010 [4]. According to the latest report of the World Health Organization in 2013, there were 287,000 maternal mortalities in the world in 2010 [5]. Generally, this index is less than one percent in the developed countries [6]. Number of the maternal mortalities in 100,000 live births in the developing countries including Kenya, Zimbabwe, Somalia, and Afghanistan were 530, 790, 1200, and 1400, respectively [7]. Studies in Bangladesh show that the rate of maternal mortality is high despite the implementation of interventions such as family planning, menstrual regulation services and safe pregnancy [8]. In Iran, the indices were 274, 150, 94, and 38 in 1975, 1990, 1995, and 2005, respectively. The final report in 2013 showed the rate of 20.3 in 100,000 live births. According to the Fifth Development Plan law, the rate in Iran should reduce to 15 out of 100,000 live births [9].
Different reasons have been mentioned for maternal mortality in various studies. A large number of maternal mortalities occur immediately after birth and early postpartum, which is mainly due to haemorrhage [10]. Khajeian et al., showed that unwanted pregnancy played the major role in maternal mortality. The most common causes of maternal mortality in this study included haemorrhage (25%) and then amniotic fluid embolism (17.5%) [11]. However, in summary, haemorrhage, hypertension, and sepsis persist to form the maternal mortality triangle. With a view to the importance of maternal mortality index due to pregnancy and birth complications, countries have designed and executed suitable operational planes over the past few years to reduce maternal mortality, develop fertility health services, and preserve and promote women health, especially during pregnancy and birth [12]. At present, there is no direct intervention capable of reducing maternal mortality considerably; however, some people consider an effective health center, skilled service staff, and women’s right of health of woman important [1]. Numerous measures have been taken in our country in this regard, one is the establishment of country’s maternal mortality surveillance in all universities nationwide. A maternal mortality index indicates the adequacy degree of pregnancy cares and the economic and social conditions of a society [13]. This index is a function of the status of women’s education, rural road network, access to emergency obstetric services and household income. Based on the United Nations Millennium Development Goals, maternal mortality should be reduced by 75% by 2015, i.e., in proportion to its basic rate 1990 [14]; however, by 2005, it was only reduced by 5% [15,16]. Complications of pregnancy and birth in the developing countries often lead to maternal death [17]. Recognizing the causes and real problems of maternal death is necessary for its reduction. In addition, other major variables such as political instability, shortage of money and the corruption related to health indices involve it and some of these factors depend on training, economic condition, and health care system. Therefore, it seems necessary to determine causes of maternal mortality and its effective factors to execute an interventional program. Therefore, this study aimed at determining the frequency and causes of the maternal mortalities caused by birth in the urban and rural areas of Iranshahr County in 2009-2013.
Materials and Methods
Design and Location
This was a retrospective descriptive study. The statistical population included all the pregnant women who died in Iranshahr County between end of April 2009 and March 2013 in a census manner.
Instrument
Data collection tool was a researcher-made questionnaire based on the literature in this field [18]. In 8 sections: Section 1 included demographic data (age of mother’s death, year of death, residence, level of education, birth attendant, type of birth, quality of cares, period of death, place of birth, mother’s insurance status, cause of death, and place of death), which were completed based on the hospital records of pregnant woman. The following sections were completed based on the health records of woman, which included current pregnancy status, records of earlier pregnancies, record of a disease, high-risk behaviours of woman and their husbands, referral status of pregnant woman, tests of pregnant woman, high-risk cases and (postpartum) endangered cases. Validity of the tool was determined by content validity in a way that the form was given to 10 experts and CVR and CVI were 0.78 and 0.85, respectively. Reliability of the questionnaire was measured by internal consistency and its Cronbach’s alpha was 0.80.
Ethical Considerations
The researcher took samples after obtaining permission from the Faculty of Medical Sciences of Iranshahr, (2008),coordinating with the Health and Treatment Department and Iran and Khatam-al-Anbia hospitals and providing a letter of recommendation to the department and hospitals. The questionnaires were completed based on health and the hospital records of the dead people. If a record were incomplete, the researcher resolved the possible shortcomings by visiting family of the dead person. Ethically, all the information remained confidential and anonymous.
Statistical Analysis
After collecting the data, they were analysed in SPSS (version 16.0). Chi-square test was used for examining the relationship between cause of death and place of death, type of birth, birth attendant and city of residence variables. The ANOVA test was used to examine the relationship between death and number of deliveries and mother’s age. A confidence level of 95% and a significance level of a=0.05 were considered in the tests.
Results
The mean age of participants were 30±6.4, range - 13 to 40 year old. The mean of deliveries of the participants was 3.9±2.5. As far as the level of education was concerned, 47% of research units were illiterate, 29.4% were at primary school level, 14.7% were at high school level, and 8.8% were at university levels. As far as economic conditions were concerned, 38.2%, 29.4%, and 32.4% of the research units were at good, average, and weak levels, respectively.
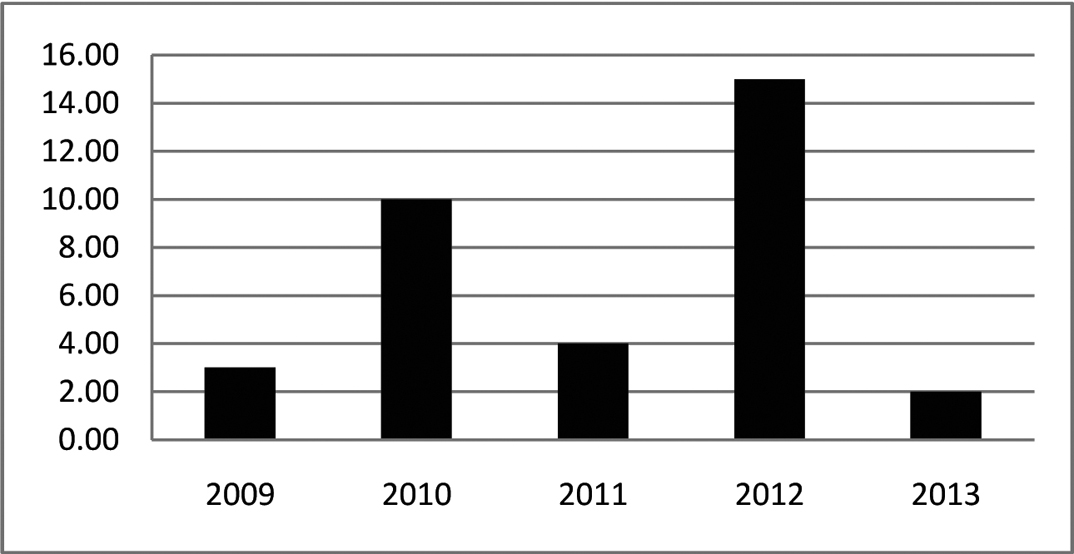
Frequency of maternal mortality between 2009 and 2013 was 34 in Iranshahr County. The maximum and minimum rates of maternal mortality were in 2012, and 2013, respectively [Table/Fig-1]. Out of 34 maternal mortalities, 35.3%, 35.3%, 14.7% and 14.7% were living in cities, main villages, satellite village, and wanderers, respectively. Out of the total deaths, 35.3% and 64.7% were at pregnancy level and postpartum level, respectively.
Frequency of maternal mortality for each year.
The results showed that the quality of 33.3% of prenatal cares was tailored to pregnancy and 66.7% was inappropriate cares. Most of them died in hospitals (50%), 48.5% died following vaginal birth, and 64.7% died after birth [Table/Fig-2&3].
Frequency distribution of place of birth of those who died in Iranshahr County between 2009 and 2013.
| Place of Birth | Frequency (%) |
|---|
| Hospital | 17 (50) |
| Labour facilities | 3 (8.8) |
| Home | 3 (8.8) |
| Undelivered | 11 (33.3) |
| Total | 34 (100) |
Frequency distribution of type of birth of those who died in Iranshahr County between 2009 and 2013.
| Type of Birth | Frequency (%) |
|---|
| Vaginal | 17 (48.5) |
| Cesarean | 6 (18.2) |
| Undelivered | 11 (33.3) |
| Total | 34 (100) |
The most common birth attendants were Specialist/GP/Midwife (52.9%), Rural Midwife/Midwife Social Worker (2.9%), respectively [Table/Fig-4].
Frequency distribution of the birth attendants of those who died in Iranshahr County between 2009 and 2013.
| Birth Attendant | Frequency (%) |
|---|
| Specialist/GP/Midwife | 18 (52.9) |
| Rural Midwife/Midwife Social Worker | 1 (2.9) |
| Local Midwife/Untrained Midwife | 2 (5.9) |
| Undelivered | 11 (33.3) |
| Total | 34 (100) |
The most common cause of mortality among the study individuals included haemorrhage (38.2%) and eclampsia and preeclampsia (26.5%) [Table/Fig-5].
Frequency distribution of maternal mortality causes in Iranshahr County between 2009 and 2013.
| Cause of Death | Frequency (%) |
|---|
| Haemorrhage | 13 (38.2) |
| Eclampsia and Preeclampsia | 9 (26.5) |
| Infection | 1 (2.9) |
| Underlying Disease | 9 (26.5) |
| Pulmonary Edema | 1 (2.9) |
| Other Causes | 1 (2.9) |
| Total | 34 (100) |
Cause of deaths of woman had a significant relationship with number of deliveries (p=0.005). That is, it has a direct relationship with the number of deliveries increasing. However, it had no significant relationship with residence (p=0.1), birth attendant (p=0.6), type of birth (p=0.4), mother’s age (p=0.3) and place of birth (p=0.1). The main cause of maternal death in rural and urban population was haemorrhage.
Discussion
This study reported 34 maternal mortalities in Iranshahr County in 4 years (2009-2013). The minimum and maximum rates of maternal mortality occurred in 2013 and 2012, respectively. In this study, maternal mortality ratio exceeds the national index. Generally, maternal mortality rate reduced in Iran following the social and economic changes during recent decades, as it reached 255 in 100,000 births in 1974 to 37.4 in 100,000 live births in 1996. Over the last few years, it reduced to about 21 in 100,000 live births [19]. However, the rate is higher than the national index in Iranshahr due to deprivation of the area and lack of healthcare. Similar to other studies, Betren et al., showed a positive relationship between a healthcare system and variables and pointed out that training and economic variables should be taken into consideration and focused on [20]. Reasons for wide variation mortality in this year’s were: different in health care status and variation in age and educational status to attention residence (rural and urban).
The results of international studies have shown that mortality rate among Iranian mothers from 651 cases in 1990 has reached fewer than 197 in 2013. This suggests an improvement in indicators of quality of care during pregnancy and after pregnancy in Iranian society [21]. The study conducted by Mohammadi et al., showed that mortality rate in pregnant women from April 2002 to March 2010 was 307 with a ratio of 6.82 cases per 100,000 live births [22]. The most important causes of mortality included bleeding, place of delivery, number of pregnancies and delivery conditions. In terms of the rate of mortality, this is not consistent with the findings of the present study which may be due to different periods in these two studies. However, the results on the causes of mortality are the same in the two studies. Rajaee et al., studied the mortality rate among mothers in Hormozgan Province in the period 2005-2010. Their results indicated that the frequency of maternal mortality was 91 with a ratio of 7.39 cases per 100,000 live births. Similarly, bleeding was found to be the main cause of mortality [23].
Mohammadinia et al., reported 307 deaths in Sistan and Baluchestan Province in a 7-year period (2002 to 2009) and 25 out of 307 deaths were related to Iranshahr County [22]. This indicates that maternal mortality rate is still high in Iranshahr province and it has been rising as compared with the earlier study. This might be due to the high rate of deliveries in Iranshahr County, variability of study period, lack of access of woman to obstetric emergencies, and lack of expertise and adequate facilities [24]. The study of Choudhury et al., in Bangladesh proved that vaginal deliveries increased with the number of the users of extensive emergency obstetric services increasing. They probably reached the necessary level of knowledge and/or health care staff gained sufficient skill in the complicated management of vaginal birth and maternal mortality reduction [14].
The study of Safizadeh et al., in Kerman in a three-year period, and the study of Mobasheri et al., in Chaharmahal and Bakhtiari Province in a ten-year period reported 25, 28, and 28 maternal mortalities, respectively [25,26]. The maternal mortality rate in our study is higher than other studies. The difference might be due to specific regional conditions, age of marriage and pregnancy in the area, and lack of expertise deprivation of Iranshahr County.
Maternal mortality rates in other countries out of 100,000 live births were reported as follows: Sweden and Denmark (lower than 10) [27]. Therefore, pregnancy and birth complications are also seen in the developed countries. However, women are not provided with sufficient and immediate treatment in the developing countries. Therefore, their mortality rate is higher. Prashant Kumar Singh et al., proved that the role of strengthening public health infrastructures across the study region, raising awareness on available health and treatment services and subsidy plan in a society to support rural and deprived societies is a participatory approach, which is effective in maternal mortality reduction [28].
The research findings showed that the participants were between 13 and 40-year-old; 2.9% were below 18 and 26.5% were above 35. The maternal mortalities in high-risk age groups were below 18 and above 35. A study showed that young age and old age pregnancies accompany the increased risk of complications and threaten maternal health [3], which indicates pregnancy at all productive ages and non-observance of family planning in Iranshahr County. This might be due to the special ethnic and cultural characteristics of the region. Old age pregnancy is a risk factor. Study showed that gestational diabetes, eclampsia, and postpartum haemorrhage occur significantly higher in old age pregnancy [26].
Scientific resources prohibit fertility in these age groups; however, this happens repeatedly and old age pregnancy might be due to increased marriage age in the country, especially in some regions, which necessitates attention of authorities and society individuals to solve youths’ marriage problems. Moreover, pregnancy at the ages below 18 may be due to low marriage age in particular ethnicities and cultures. Therefore, health authorities should take a particular attention to adopt a family planning and consultation program for young age pairs. Singh et al., showed those economic, social, and cultural factors are effective in using maternal health and treatment services by rural adolescent girls in India. Therefore, the existing healthcare programs should take vulnerable groups such as adolescent poor rural married women into consideration and make plans to allow them to use maternal healthcare services and deal with their unsatisfied needs [29].
The study findings showed that 47% of the deceased women were illiterate. Maternal death index is a function of their literacy status. Improvement of woman’ educational level plays a crucial role in improving their health, which may lead to learning educational materials, timely referral of expectant woman, and proper functioning of health and treatment staff for them [24]. Aggarwal et al., proved that women should be trained on the importance of prenatal care and regular check-ups. Untrained midwives should be trained. Obstetric complications at early stages and high-risk individuals should be referred to the health system for better control [30].
The study findings showed that the most common cause of mortality of the study woman included haemorrhage, eclampsia and preeclampsia. In 2011, the statistics department of maternal health center for Zahedan University of Medical Sciences announced haemorrhage, underlying disease, and preeclampsia as the marital mortality causes, similar results were also obtained from the studies carried out in other provinces. For instance, Mobasheri et al., mentioned haemorrhoid as the most common maternal mortality in Chaharmahal and Bakhtiari Province [26], Gholami Taromsari announced haemorrhoid as the most common maternal mortality in Kohgiluyeh and Boyer-Ahmad Province (41%) [31]. Ghulmiyyah et al., proved that the most common mortality in the developed countries were eclampsia and preeclampsia, which were reduced considerably upon the access of society to suitable cares at the appropriate time [32].
Therefore, eclampsia was the most common causes of maternal mortality in the developing countries. With respect to the most common maternal mortality in Iranshahr County, the measures such as a quick access to blood products, emergency obstetric and quick referral to equipped specialized centers, regular and effective control of blood pressure, regular examination and monitor of woman in terms of increased blood pressure, eclampsia, training pregnant woman of the early symptoms of such disorders may be effective in saving lives of woman.
This study showed a significant relationship between maternal mortality and number of pregnancies. Abdolahipour et al., showed a significant relationship between number of pregnancies and maternal mortality [33]. In terms of number of pregnancies, Akhlaghi et al., proved that the highest mortality occurred for those woman with more than 6 pregnancies [34]. The study of Mohammadinia et al., in Sistan and Baluchestan Province announced that the most mortality was related to those with more than 4 pregnancies [22]. One of the major causes of maternal mortalities in Third World countries is their large number of pregnancies and no referral to receive healthcare. This study showed no significant relationship between the underlying variables and mortality. Of course, lack of a significant relationship does not denote lack of a real relationship because sample size of this study has not been satisfied for examining these relationships. With respect to the number of these variables, a higher sample size is needed for examining these relationships.
Limitation
The limitation of the present study was that, the information obtained from recorded documents were not of sufficient quality and correct information could not be obtained from them. We missed some data due to incomplete documents and unregistered cases.
Conclusion
With respect to the central role of mother in family and health indices of each country, it is possible to reduce rates of maternal mortality considerably through some short- and long-term measures such as increasing prenatal care and birth, raising awareness of woman and trainers, preventing deliveries by untrained midwives, encouraging deliveries in health centers and hospitals, preventing unnecessary cesareans and encouraging painless birth.
Funding
This research work was funded by Iranshahr University of Medical Science.