Meningotheliomatosis: A Rare Cause of Diffuse Miliary Pattern Pulmonary Opacities
James Benjamin Gleason1, Jonathan Ryan Schroeder2, Jose Ramirez3
1 Chief Fellow, Department of Pulmonary and Critical Care Medicine, Cleveland Clinic Florida, Weston, Florida, USA.
2 Fellow, Department of Pulmonary and Critical Care Medicine, Cleveland Clinic Florida, Weston, Florida, USA.
3 Attending Physician, Department of Pulmonary and Critical Care Medicine, Cleveland Clinic Florida, Weston, Florida, USA.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. James Benjamin Gleason, 2950 Cleveland Clinic Blvd, Weston, Florida, USA.
E-mail: Gleasoj@ccf.org
Meningothelial like bodies, Surgical lung biopsy, Transbronchial biopsy
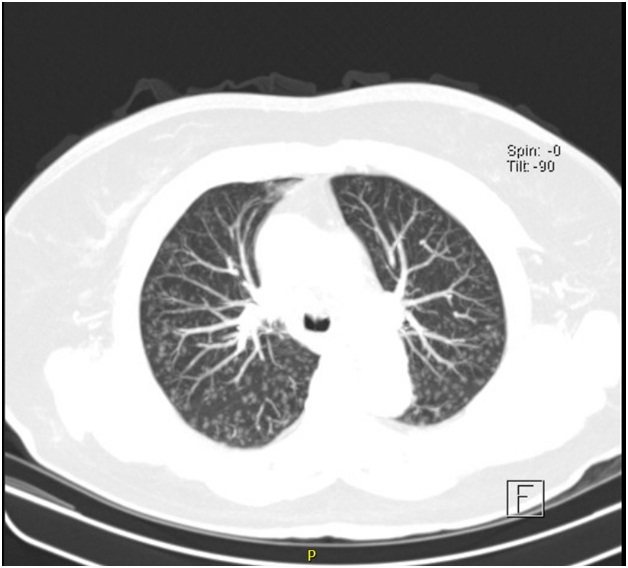
A 63 year old female presented for incidentally discovered pulmonary nodules. The Computed Tomography (CT) scan of the chest with contrast showed innumerable and diffusely distributed nodules up to 4mm in a military type pattern [Table/Fig-1]. There was no mediastinal or hilar adenopathy and she denied any respiratory complaints including dyspnea, cough or sputum production. She was born in Paraguay and moved to the United States of America in her early 30’s. Medical, social and family history was remarkable for a 10 pack-year smoking history and occupational chemical fume exposure, working in a compounding pharmacy.
Axial CT chest with contrast with maximum intensity projection processing demonstrating diffuse military pattern ground glass nodules.
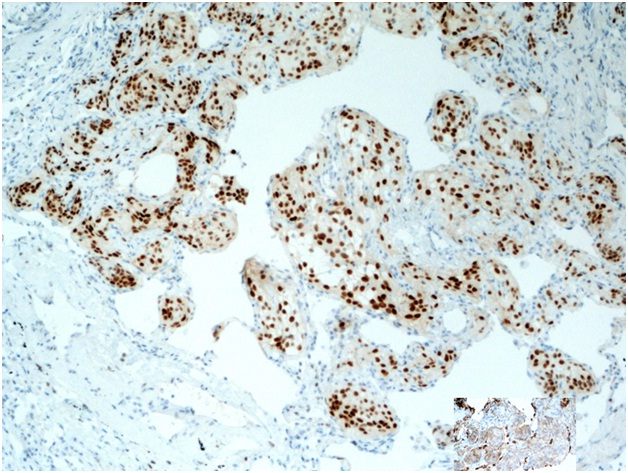
Human Immunodeficiency Virus (HIV), Tuberculosis, Autoimmune evaluations were negative. Spirometry was normal and Diffusing capacity of the Lungs for Carbon Monoxide (DLCO) was decreased. Bronchoscopy was performed, cultures were negative, transbronchial biopsies revealed many meningothelial like bodies confirming the diagnosis of Diffuse Pulmonary Meningotheliomatosis [Table/Fig-2,3].
Fragments of lung parenchyma with aggregates of meningothelial-like bodies which stain positively for progesterone receptor.
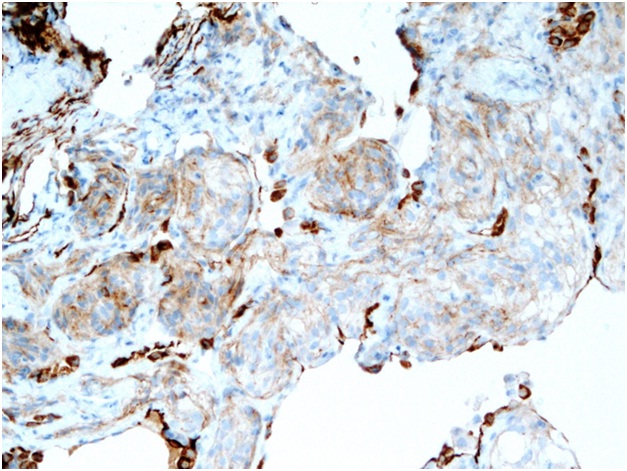
Higher magnification, demonstrating the typical positive staining for epithelial membrane antigen consistent with meningioma cells.
This exceedingly rare condition, typically asymptomatic and occurring in women near the sixth decade of life, is associated with an increased prevalence of pulmonary malignancy [1]. Positron Emission Tomography/Computed Tomography (PET/CT) scan of our patient did not reveal abnormalities suggestive of underlying malignancy. This condition is historically diagnosed with surgical lung biopsy [2] and we describe the second case diagnosed by transbronchial biopsy [3]. Diffuse pulmonary meningotheliomatosis should remain in the differential for miliary pattern nodules. Lastly, the diagnosis can be obtained from transbronchial biopsy possibly alleviating the need for surgical lung biopsy.
[1]. Mizutani E, Tsuta K, Maeshima AM, Asamura H, Matsuno Y, Minute pulmonary meningothelial-like nodules: clinicopathologic analysis of 121 patientsHuman Pathology 2009 40(5):678-82. [Google Scholar]
[2]. Suster S, Moran CA, Diffuse pulmonary meningotheliomatosisThe American Journal of Surgical Pathology 2007 31(4):624-31. [Google Scholar]
[3]. Bernabeu Mora R, Sánchez Nieto JM, Hu C, Alcaraz Mateos E, Giménez Bascuñana A, Rodriguez Rodriguez M, Diffuse pulmonary meningotheliomatosis diagnosed by transbronchial lung biopsyRespiration 2013 86(2):145-48. [Google Scholar]