Congenital Defect in Lesser Omentum Leading to Internal Hernia in Adult: A Rare Case Report
Surag Kajoor Rathnakar1, Shridhar Muniyappa2, Vikram Hubbanageri Vishnu3, Nagaraj Kagali4
1 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
2 Professor, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
3 Senior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
4 Assistant Professor, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Surag Kajoor Rathnakar, Kamal Dev Daycare Clinic, S.P Road, Sakleshpur, Hassan, Karnataka-573134, India.
E-mail: surag244@gmail.com
Intestinal obstruction is one of the common clinical condition which is encountered in emergency room. Internal hernia is one of the rare causes of small bowel obstruction accounting for less than 1% of cases. A congenital omental defect is very rare, but can potentially cause internal hernia leading to obstruction or strangulation of the bowel.
We present a case of a 54-year-old man who was brought to the emergency department with sudden onset of lower abdominal pain. He had no history of abdominal surgeries or history of trauma. An emergency laparotomy was performed. On exploring the abdominal cavity, the lesser omental defect was detected, 3cm in size. Loops of jejunum had gone through the defect. Congested bowel loop was pulled back and defect was approximated. An adult congenital omental defect is rare; however, it should be considered as one of the differential diagnoses in a relatively young patient with bowel obstruction without external hernia, previous abdominal surgery or trauma.
Congested bowel loop, Intestinal obstruction, Lesser omental defect, Transomental internal hernia
Case Report
A 54-year-old male patient came to the emergency with sudden onset of lower abdomen pain, vomiting and constipation since 1 day. There was no history of abdominal surgery or trauma. On physical examination his vitals was stable, abdominal distension was present, tenderness was present in umbilical and hypogastric region, bowel sounds were absent, per rectum examination was normal.
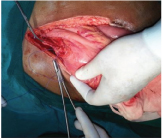
Routine haematological and biochemical tests were normal. Erect X-ray abdomen revealed bowel shadows with multiple air fluid levels suggestive of small bowel obstruction. Emergency CT scan facility was not available in the hospital and hence, an emergency laparotomy was performed under General Anesthesia (GA), by taking prior consent. Intra operative findings revealed a distended loop of jejunum passing through defect of 3x2cm in lesser omentum with congestion of bowel loop [Table/Fig-1,2 and 3]. Loop of jejunum was pulled back [Table/Fig-4] and warm mops were placed over it till it appeared pinkish and the defect was approximated with vicryl 2-0 sutures [Table/Fig-5]. Postoperative stay was uneventful with bowel sounds appearing after 2 days and the patient was discharged after 10 days after abdominal wound suture removal. On follow up, after 1 month, patient was found to be healthy.
Loop of jejunum through defect in lesser omentum.

Defect of 3x2 cm in lesser omentum;


Bowel loop being pulled back.

Lesser omental defect being approximated with 2-0 vicryl.
Discussion
Internal hernia is protrusion of the bowel through the mesentry or peritoneum but which remains within the abdominal cavity. It is a very rare cause of small bowel obstruction with significant mortality. It can be congenital or acquired. Paraduodenal space, foramen of Winslow, defect in mesentry or omentum, transverse mesocolon, diaphragm, broad ligament are some of the potential sites of internal hernia. Internal hernia is a rare condition which accounts for 0.2–0.9% of cases of intestinal obstruction [1,2]. Transomental hernia accounts for 1–4% of all the internal hernias. Majority of them occurs through defect in the right side of the greater omentum without a sac and are always intraperitoneal. Internal hernia through defect in lesser omentum is extremely rare [3]. Congenital anatomic defects of the liver, lesser sac, mesentery, as well as the presence of adhesions or increased intra-abdominal pressure are some of the predisposing factors for transomental hernias [4]. The herniated bowel loops may return to its normal location or may develop gangrene depending on the size of the defect and length of the bowel loop which has gone through the defect. Internal hernia might occur after previous surgeries or following abdominal trauma. However a congenital defect in omentum is very rare that too presenting in middle age but can potentially cause internal hernia with subsequent strangulation of the small intestine [5]. There are reports of congenital defects leading to hernia in paediatric age group leading to unexpected death [6]. Intestinal obstruction due to internal hernia should be suspected in patients without external hernia or previous abdominal surgery or trauma. Sometimes it is difficult to diagnose internal hernia because of lack of specific signs and symptoms [7]. On the other hand, internal hernias are invariably manifested as acute intestinal obstruction that requires early diagnosis and immediate surgery. Radiological tools like CT scan will be most helpful preoperatively and can be diagnosed by characteristic findings on CT like stretched bowel sign” if it is kept in mind as a probable diagnosis [8]. However most of the time they are usually diagnosed on table for acute intestinal obstruction [9–12].
The management of acute intestinal obstruction will be adequate initial resuscitation and nasogastric tube decompression, followed by immediate laparotomy. A thorough examination of the abdominal cavity is done to identify the structures involved in the obstruction. Then the herniated structures are reduced, resection of ischemic intestinal segments done, followed by closure of the hernial orifice [13].
Conclusion
Internal hernia should be considered as one of the differential diagnoses in patient with bowel obstruction without external hernia, previous abdominal surgery or trauma. When omental defect is found on table in unrelated abdominal surgery, it should be closed to prevent it from causing internal hernia in future.
[1]. Hashimoto D, Hirota M, Sakata K, Yagi Y, Baba H, Adult transmesenteric hernia: Report of two casesSurg Today 2012 42:489-92. [Google Scholar]
[2]. Rehman Z, Khan S, Large congenital mesenteric defect presenting in an adultSaudi J Gastroenterol 2010 16:223-25. [Google Scholar]
[3]. Gulino D, Giordano O, Gulino E, Les hernies internes de l’abdomen. À propos de 14 casJ Chir (Paris) 1993 130:179-95. [Google Scholar]
[4]. Panda SK, Panda A, Strangulated internal hernia through lesser sac- An unusual case of small bowel obstructionAustin J Surg 2015 2(6):1072 [Google Scholar]
[5]. Crispín-Trebejo B, Internal Abdominal Hernia: Intestinal obstruction due to trans-mesenteric hernia containing transverse colonInternational Journal of Surgery Case Reports 2014 5(7):396-98.PMC. Web. 16 May 2016 [Google Scholar]
[6]. Katagiri H, Okumura K, Machi J, Internal hernia due to mesenteric defectJournal of Surgical Case Reports 2013 5 [Google Scholar]
[7]. Genovese AM, Taranto F, Fiore D, Segreto M, Giardinelli A, Cavallaro G, Internal abdominal hernia. Unusual case of intestinal occlusionMinerva Chir 2000 55:177-80. [Google Scholar]
[8]. Kundaragi NG, Vinayagam S, Mudali S, Stretched bowel sign in combined transmesocolic and transomental internal hernia: A case report and review of literatureThe Indian Journal of Radiology & Imaging 2014 24(2):171-74. [Google Scholar]
[9]. Pessaux P, Tuech JJ, Derouet N, Du Plessis R, Roncerray J, Arnaud JP, Internal hernia: A rare cause of intestinal obstruction. Apropos of 14 casesNan Chir 1999 53:870-73. [Google Scholar]
[10]. Zavan NP, Lee FT Jr, Yandow DR, Unger JS, Abdominal hernias: CT findingsAm J Roentgenol 1995 164:1391-95. [Google Scholar]
[11]. Blachar A, Federle MP, Dodson SP, Internal hernia: Clinical and imaging findings in 17 patients with emphasis on CT criteriaRadiology 2001 218:68-74. [Google Scholar]
[12]. Wachsber RH, Helinek TG, Merton DA, Internal abdominal hernia diagnosis with ultrasonographyCan Assoc Radio J 1994 45:223-24. [Google Scholar]
[13]. Ozenc A, Ozdemir A, Coskun T, Internal hernia in adultsInt Surg 1998 83:167-70. [Google Scholar]