Prosthetic Management of a Nasal Septal Defect using a Custom Made Unilateral Intranasal Stent: A Case Report
Teny Fernandez1, Harshakumar Karunakaran2, Sheela Virginia Rodrigues3
1 Senior Resident, Department of Prosthodontics, Government Dental College, Alappuzha, Kerala, India.
2 Professor and Head, Department of Prosthodontics, Government Dental College, Trivandrum, Kerala, India.
3 Professor and Head, Department of Prosthodontics, Government Dental College, Alappuzha, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Teny Fernandez, XVII/1657(B), Azhikkakath House, Mundamveli P.O., Ernakulam, Kerala-682507, India.
E-mail: tenyfernandez@gmail.com
Various etiologies including congenital malformations, infections, trauma, iatrogenic causes or complications of systemic diseases can result in perforation of the nasal septum. The common symptoms associated with such defects include difficulty in breathing, nasal twang in voice, rhinorrhea, etc. Obturation can be achieved by insertion of a unilateral nasal stent. An attempt has been made in the present report to address the prosthetic management of pateint having nasal septum perforation utilizing a unilateral, custom made heat cured acrylic stent and the details of the technique are presented.
Customized acrylic stent, Nasal stent, Nasal septal perforation
Case Report
A 35-year-old female patient was referred to the Department of Prosthodontics, for prosthetic rehabilitation of an intranasal septal defect. Three months earlier the patient had undergone a submucous resection surgery for deviated nasal septum. The previous surgery resulted in the defect of nasal septum due to which the patient reported difficulty in breathing, discomfort, nasal twang and nasal discharge.
The extent and configuration of the defect was examined using a nasal speculum and otoscope [Table/Fig-1]. During the examination of the defect revealed that the site had mild inflammation and was in healing stage. The patient was not willing for a repeated surgical procedure. Hence, a heat processed intranasal stent in one of the nostrils was planned for the patient. The medial wall of the stent would separate the right and left nasal cavities while prosthetically obturating the defect.
Examination of nasal septal defect using otoscope.

Procedure: The patient was made to sit upright and the inner surfaces of the nostrils were gently coated with petroleum jelly. The left nostril was blocked with gauze piece to prevent the flow of impression material into that nostril. The patient was instructed to breathe through mouth during the impression making procedure. Hollow portion of a stainless steel ‘ball pen refill’ was cut to the desired length for carrying the impression material. The edges of the cut portion were smoothened to prevent trauma. An impression of the right nostril was made with addition silicone putty and light body elastomeric impression material (Express Light Body, 3M ESPE) [Table/Fig-2]. Beading and boxing of the impression was done and impression was poured to obtain sectional casts [Table/Fig-3,4]. The repositioning of the stainless steel hollow tube was done by indexing using a bent orthodontic wire inserted 4mm into the two parts of the sectional cast on either side. Autopolymerizing acrylic resin was used to join this area to the orthodontic wire [Table/Fig-5]. The separable parts and indices could be used for the exact repositioning of the hollow tube [Table/Fig-6]. After removal of the impression material, the stainless steel hollow tube was repositioned and wax was poured into the cavity. Wax try-in of the prosthesis was done and necessary corrections were made [Table/Fig-7]. The try-in prosthesis was invested in a dental flask. The hollow portion of the tube was blocked out using putty impression material and dewaxing was done [Table/Fig-8,9]. Heat cure acrylic resin was mixed and packed into the mould and sufficient time was given for bench curing. A long curing cycle was employed so as to prevent the presence of any residual monomer. After deflasking, the extended portion of the stainless steel tube of the retrieved prosthesis was cut, putty material removed and the metal-acrylic margins were trimmed and made inconspicuous [Table/Fig-10]. The prosthesis was polished and inserted into the right nostril of the patient [Table/Fig-11].
Impression of the nasal septal defect.

Beading and boxing procedure.

Sectional casts obtained from the impression.

Indexing procedure using orthodontic wire and acrylic resin.
Separable parts after removal of the impression.

The wax try-in prosthesis invested.

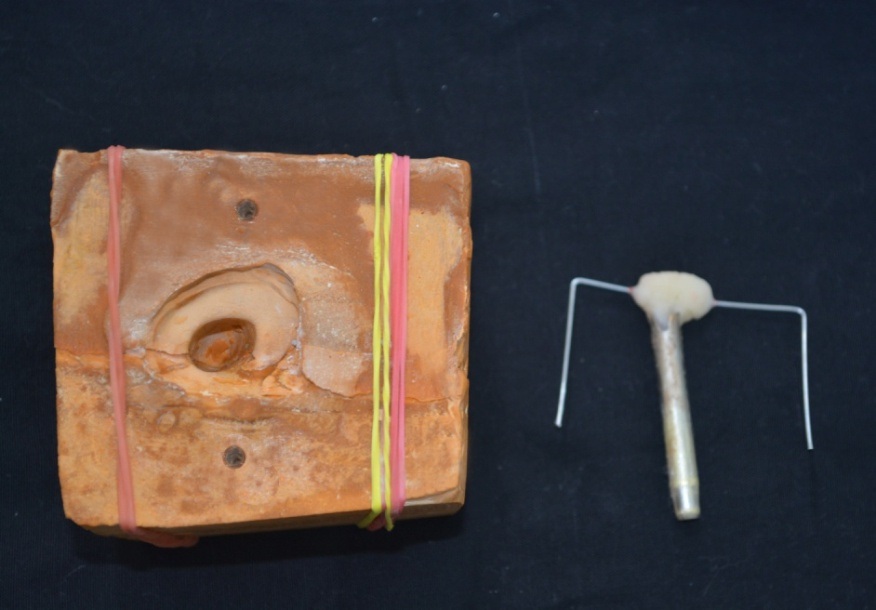
Casts after de-waxing procedure.

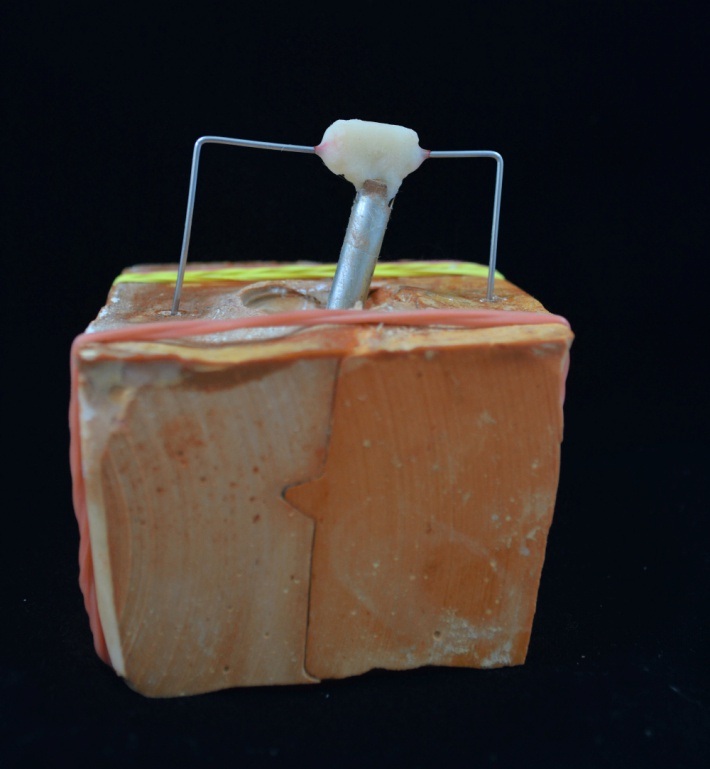
Heat cure acrylic processed intranasal stent.

Finished intranasal stent inserted.

Instructions were given to the patient regarding the method of insertion and removal of the prosthesis. Post insertion appointments were scheduled to ascertain that the nasal mucosal tissue surrounding the intranasal stent was not inflamed.
Discussion
Nasal deformities can arise from trauma, congenital defects, surgical procedures, infections or as a complication of some systemic diseases [1,2]. Local factors cause nasal septal perforations more frequently than systemic factors [3]. The submucous resection surgical procedure for deviated nasal septum removes most of the quadrangular cartilage, leaving an inverted L-shaped strut for support. The major complications of submucous resection surgery include incomplete correction with persistent symptoms, external nasal deformity and septal perforation [4]. The rate of nasal septal perforation after septoplasty procedure ranges from 1.6% to 6.7% [5,6]. Patients with septal perforations suffer from recurrent epistaxis, nasal obstruction, discharge, crusting, dryness, pain and whistling due to the complete defect of mucosal and cartilaginous tissues of the nasal septum [7]. Various methods for surgical management have been proposed including the application of septum shortening procedure, mucosal flaps, composite free graft from anterior end of middle turbinate and fascia and free pericardium autografting technique [8]. But such procedures may result in the breakdown of the surgical site area. Prosthetic rehabilitation using nasal stents may be necessary in such cases particularly those involving cartilaginous perforations.
An intranasal stent is a removable prosthesis that can be inserted into the nasal cavity to support the form of nose [9,10]. Nostril retainer or nasal stent can be used after cartilage graft replacement surgery to retain the corrected position of the nose [11,12]. Resorbable plates when used as internal nasal splints, resulted in postoperative exposure and extrusion [12]. Constructing a nasal septal obturator from an accurate impression of the defect has been proven to be the most logical approach in managing these defects [13]. Yeow et al., analysed the benefit of postoperative nasal splinting and concluded that the use of splint resulted in improved aesthetic outcome and nasal symmetry [14]. A transparent heat cure acrylic resin was used in this case to make it indistinguishable. Since the risk of dislocation of the stent and subsequent aspiration was over-ruled as the stent was customized for the patient with a wing of acrylic, which allowed easy removal of the stent. Also the nasal stents made from heat processed acrylic are safe, convenient and economic. Due to lack of flexibility, the fabrication of customized heat-processed nasal stent is limited to small defects that occur in the anterior septum [3].
Conclusion
The present case report describes the various laboratory procedures involved in the fabrication of a customized intranasal stent used in the management of a septal defect. The prosthetic septal insert helps in the partitioning of nasal cavity. In addition, a customized nasal stent is easy to fabricate, non invasive and economical.
[1]. Parel SM, Intranasal conformersJ Prosthet Dent 1980 43(4):439-44. [Google Scholar]
[2]. Beumer J, Curtis TA, Marunick MT, Maxillofacial rehabilitation prosthodontic and surgical considerations 1996 3St LouisIshiyaku EuroAmerica:455-77. [Google Scholar]
[3]. Zaki HS, Myers EN, Prosthetic management of large nasal septal defectsJ Prosthet Dent. 1 997 77(3):335-38. [Google Scholar]
[4]. Fettman N, Sanford T, Sindwani R, Surgical management of the deviated septum: techniques in septoplastyOtolaryngol Clin North Am 2009 42(2):241-52. [Google Scholar]
[5]. Kantas I, Balatsouras DG, Papadakis CE, Marangos N, Korres SG, Danielides V, Aesthetic reconstruction of a crooked nose via extracorporeal septoplastyJ Otolaryngol Head Neck Surg 2008 37(2):154-59. [Google Scholar]
[6]. Yanagisawa E, Ho S.Y., Unintended middle turbinectomy during septoplastyEar Nose Throat J 1998 77(5):368-69. [Google Scholar]
[7]. Teymoortash A, Werner JA, Repair of nasal septal perforation using a simple unilateral inferior meatal mucosal flapJ Plast Reconstr Aesthet Surg 2009 62(10):1261-64. [Google Scholar]
[8]. Fairbanks DN, Fairbanks GR, Surgical management of large nasal septum perforationsBr J Plast Surg 1971 24(4):382-87. [Google Scholar]
[9]. The glossary of prosthodontic termsJ Prosthet Dent 2005 94(1):10-92. [Google Scholar]
[10]. Seals RRJr, Bohnenkamp LG, Parel SM, Intranasal prostheses, splints, and stentsJ Prosthet Dent 1988 60(5):595-601. [Google Scholar]
[11]. Salyer K.E, Early and late treatment of unilateral cleft nasal deformityCleft Palate Craniofac J 1992 29(6):556-69. [Google Scholar]
[12]. Wong G.B, Burvin R, Mulliken J.B, Resorbable internal splint: an adjunct to primary correction of unilateral cleft lip-nasal deformityPlast Reconstr Surg 2002 110(2):385-91. [Google Scholar]
[13]. Moergeli J.R, Jr. An improved obturator for a defect of the nasal septumJ Prosthet Dent 1982 47(4):419-21. [Google Scholar]
[14]. Yeow VK, Chen PK, Chen YR, Noordhoff SM, The use of nasal splints in the primary management of unilateral cleft nasal deformityPlast Reconstr Surg 1999 103(5):1347-54. [Google Scholar]