Type IIA Monteggia Fracture Dislocation with Ipsilateral Distal Radius Fracture in Adult – A Rare Association
Raghavendra S Kembhavi1, Boblee James2
1 Assistant Professor, Department of Orthopaedics, Sree Lakshmi Narayana Institute of Medical Sciences, Pondicherry, India.
2 Professor, Department of Orthopaedics, Sree Lakshmi Narayana Institute of Medical Sciences, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghavendra S Kembhavi, Plot No 8, Rajaannamalai Nagar, Behind Police Quaters, Pondicherry-605006, India.
E-mail: kembhavi.raghavendra@gmail.com
Monteggia fracture constitutes about 5-10% of the forearm fractures. Monteggia fracture by definition is proximal ulnar fracture with disruption of proximal radioulnar joint. Bado classified Monteggia fracture dislocation into four types and Jupiter subclassified type II Bado’s fractures into four types. The associated injury in the form of distal radial fractures and distal humerus fractures are rare though many cases of distal radial physeal injuries have been reported in paediatric population. Hereby we report a rare association of type IIA Monteggia fracture dislocation with ipsilateral distal radius fracture in an adult patient. This case report also highlights on proper examination and full length radiographs of forearm to avoid missing injury at wrist in cases of elbow injuries. Management of such complex injuries included open reduction and internal fixation of olecronon fracture, distal radius fracture and radial head resection. Functional outcome at six months was good at wrist whereas at elbow, stiffness was a major concern with elbow range of movement from 40°-110°.
Dorsal barton, Olecronon, Prosthesis, Radial head, Stiffness
Case Report
A 60-year-old female was brought to our hospital casualty with left upper limb supported in a sling with history of injury to elbow and wrist following fall in the bathroom. There were no injuries in other parts of body. Past history showed old malunited distal radius fracture nine months back which was managed with local native bandages. There were no other co-morbidities. On examination, patient was right hand dominant with swelling, deformity and tenderness over left elbow and wrist with no external skin injuries or bruises. There were no distal neurovascular deficits. There were no injuries in the other parts of the body. Patient was admitted and above elbow plaster of paris slab was applied. Radiography showed displaced and comminuted olecronon fracture with radial head fracture dislocation [Table/Fig-1]. Wrist radiography showed distal radius intra-articular fracture with distal radioulnar joint disruption (Frykmans type V) with old malunited distal radius fracture [Table/Fig-2]. Computed Tomography (CT) showed clear fracture pattern with comminution at radial head with large radial head fragment lying at back of capitellum with undisplaced coronoid fracture [Table/Fig-3a-c]. CT at wrist showed minimally displaced intra-articular distal radius fracture with dorsal comminution with distal radioulnar joint disruption [Table/Fig-4]. Patient was worked up with all proper preoperative investigations and was planned for surgery two days after trauma once swelling had reduced. Patient was operated under general anaesthesia, in supine position with arm laid across the chest and under tourniquet. Preoperative antibiotics were administered before tourniquet inflation. Posterior approach was used and olecronon was reduced and fixed with 3.5 recon titanium locking plates [Table/Fig-5a]. Articular congruency at ulno-humeral joint was achieved. Coronoid fracture which was undisplaced was fixed via olecronon fracture with same posterior approach and implants used for olecronon fixation. After plating ulna, main fragment of radial head seen at the back of capitellum was resected and few comminuted radial head fragments were resected too. Irregular edge of proximal radius was smoothened. Radial collateral ligament and annular ligament were found disrupted whereas lateral ulnar collateral ligament was found intact. Minimal to moderate varus instability was seen at elbow following olecronon plating and radial head resection. To increase elbow stability, thick transolecronon Kirschner (K)-wire was passed into humerus [Table/Fig-5a]. Comminuted distal radius fracture was fixed with 3.5 dorsal buttress locking plate and distal radio ulnar junction disruption was reduced and fixed with K- wire [Table/Fig-5b]. Operating time was three hours.
Anteroposterior and lateral radiograph of elbow showing comminuted olecronon fracture with radial head fracture dislocation.

Anteroposterior and lateral radiograph of wrist showing distal radius intraarticular fracture with distal radioulnar joint disruption (Frykmans type V).

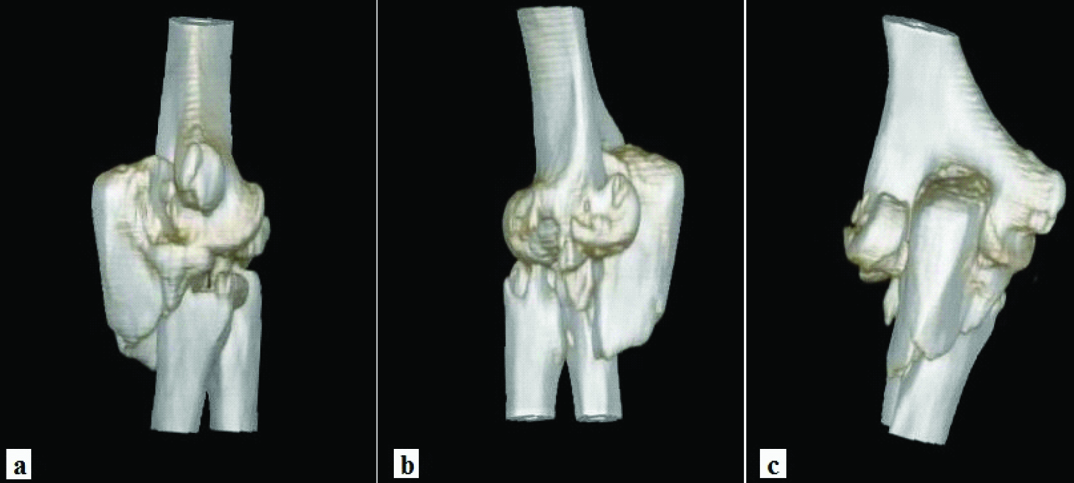
3D reconstruction CT showing (a) olecronon fracture with coronoid fracture, (b) comminuted radial head fracture and (c) main fragment of radial head lying at back of capitellum (c).
CT showing distal radius fracture intraarticular with dorsal comminution (arrow). 3D reconstruction CT showing distal radioulnar junction disruption.

a. Immediate postoperative lateral X ray of elbow showing olecronon fixation with recon titanium locking plate. To increase elbow stability, two transolecronon K-wires were passed, b. anteroposterior view of wrist showing distal radius fracture fixation with 3.5 dorsal buttress locking plate. Distal radioulnar junction was provisionally reduced with K-wire.

Postoperatively patient was immobilized in plaster slab for three weeks. At three weeks, K-wires were removed at elbow and wrist and range of movement exercises were started. At six weeks patient was allowed to perform light activities and at three months she was allowed to perform routine household works. Stiffness was a concern at elbow with elbow range of movement from 40° to 110° and functional assessment at five months with Mayo Elbow Performance Score showed fair result (score of 70 out of 100) [Table/Fig-6]. Modified Mayo Performance Scoring for wrist showed good result (score of 80 out of 100). Distal radioulnar joint disruption still persisted with increased positive ulnar variance compared to immediate post surgery probably due to proximal radius migration due to radial head resection [Table/Fig-7]. However, patient did not complain of pain at ulnar side of wrist.
At five months follow up, patient showed elbow range of movement from 40° - 110°.

Five months postoperative anteroposterior and lateral wrist X ray showing complete union of distal radius fracture. Distal radioulnar junction disruption still persisted with increased positive ulnar variance compared to immediate post surgery probably due to proximal radius migration resulted from radial head resection (a).

Postoperative radiographs were taken at 4 and 12 weeks. Good radiological union was seen at five months postoperatively at olecronon fracture site and distal radius site [Table/Fig-7,8].
Five months postoperative anteroposterior and lateral X-ray showing complete radiological union of olecronon fracture. Lateral radiograph showing radiocapitellar subluxation (b).

Discussion
Monteggia fracture dislocation by definition is proximal ulnar fracture with disruption of proximal radioulnar junction. Bado classified Monteggia fracture dislocations into four types depending on direction of radial head displacement. Bado’s type II injuries are the most common variety in adult population whereas Bado’s type I is common in paediatric population [1]. Adult Bado’s type II injuries are usually associated with radial head fractures and coronoid fractures [2]. Similarly, we had radial head fracture dislocation wherein radial head was comminuted with main fragment lying at back of capitellum. There are also fractures similar to Monteggia which are classified as ‘Monteggia equivalents and variants’ since they share similar radiological findings and biomechanism of injury [3]. Transolecronon fractures or anterior olecronon fractures differs from Monteggia fracture dislocation with minimal involvement of proximal radioulnar joint [4]. In our patient proximal radioulnar joint seemed disrupted. Jupiter again classified Bado’s type II fracture dislocations into four types depending on level of olecronon fracture. Type IIA fractures involves distal aspect of olecronon with coronoid fractures, type IIB fractures involves metadiaphyseal fractures without involving coronoid fractures, type IIC involving diaphyseal fractures of ulna and type IID fractures involving proximal one-third ulna fractures involving olecronon and coronoid process [2]. Looking at radiology and CT scan, Monteggia fracture-dislocation in our patient was classified as type IIA, according to Bado’s and Jupiter’s sub-classification.
Monteggia fractures dislocation in combination with ipsilateral distal radial physeal injuries have been described few times in children [5,6]. However, in adults such combination of Monteggia fractures with ipsilateral distal radius have been reported only once as per our knowledge [7]. On the other hand, ipsilateral Monteggia fractures and Gallezzi fracture dislocation have been explained few times in adults [8]. Mechanism of injury of such ipsilateral injuries is not very well understood. Probable mechanism could be, fall on outstretched hand with full pronated forearm which leads to distal radius fracture. While this happens, trunk continues to rotate and longitudinal force along with external rotatory force leads to Monteggia injury at elbow.
Essex Lopresti lesion is defined as proximal migration of radius with longitudinal disruption of interosseous membrane following radial head or neck fracture leading to distal radio-ulnar junction disruption or proximal radio-ulnar junction or both. In our patient, there was clear distal radioulnar junction disruption radiologically. Since patient also had old malunited distal radius fracture with distal radioulnar junction disruption as shown by older radiology, we attributed present distal radioulnar junction disruption to both older injury as well as present Essex Lopresti lesion based on clinicoradiological findings.
Management of these complex injuries are difficult. Paediatric Monteggia fracture dislocations with ipsilateral distal radius fractures have been managed by closed reduction and percutaneous K-wire fixation for the distal radius as well as radial head physeal injury and plating for ulnar shaft injuries. In adults, principles of such complex elbow injuries like type IID Monteggia fracture dislocation include radial head reconstruction or replacement by prosthesis after provisional fixation of ulna followed by definitive ulnar shaft plating. This is followed by coronoid process fixation and olecronon dorsal plating. Finally ligamentous component of injury has to be addressed [9]. In our case, due to extreme comminution which was not reconstructable we performed radial head excision. However due to intact lateral ulnar collateral ligament, age of patient and low functional demand of left elbow, we accepted minimal varus instability at the elbow after stable fixation of olecronon with plating and hence radial head excision was performed without radial head prosthesis. However to increase elbow stability, we fixed elbow with thick transolecronon K-wire. Jupiter et al., reported late radiocapitellar subluxation in complex Monteggia injuries with the radial head comminution who underwent radial head excision without proper anatomical reduction of proximal ulna [10]. In our patient too we noticed late radiocapitellar subluxation [Table/Fig-8b]. Along with that, stiffness was a major issue in our patient.
Conclusion
Monteggia fracture dislocation with ipsilateral distal radius fracture is a rare injury both in children and adults. Thorough examination and full length forearm radiographs should be taken to avoid missing ipsilateral wrist injuries in cases of elbow injuries. Stiffness is a major concern in managing such cases.
[1]. Ring D, Jupiter JB, Waters PM, Monteggia fractures in children and adultsJ Am Acad Orthop Sur 1998 6(4):215-24. [Google Scholar]
[2]. Scolaro J, Beingessner D, Treatment of Monteggia and transolecranon fracture-dislocations of the elbow - a critical analysis reviewJBJS Reviews 2014 2(1):e3 [Google Scholar]
[3]. Beaty JH, Kasser JR, Rockwood and Wilkins Fractures in Children: Monteggia Fracture-Dislocation in Chidren 2006 6th edition:447-551. [Google Scholar]
[4]. Doornberg J, Ring D, Jupiter JB, Effective treatment of fracture-dislocations of the olecranon requires a stable trochlear notchClin Orthop 2004 429:292-300. [Google Scholar]
[5]. Sood A, Khan O, Bagga T, Simultaneous monteggia type I fracture equivalent with ipsilateral fracture of the distal radius and ulna in a child: a case reportMed Case Reports 2008 2:190 [Google Scholar]
[6]. Williams HLM, Madhusudhan TR, Sinha A, Type III monteggia injury with ipsilateral type II Salter Harris injury of the distal radius and ulna in a child: a case reportBMC Res Notes 2014 7:156 [Google Scholar]
[7]. Lee PC, Su JY, Yeh WL, Adult monteggia fracture with ipsilateral distal radius fracture: case reportChang Gung Medical Journal 2000 23(1):38-42. [Google Scholar]
[8]. Malik M, Galfat DR, Ipsilateral Monteggia and Galeazzi fracture dislocation: a case reportInternational Journal of Orthopaedics Traumatology & Surgical Sciences 2015 1(2):53-55. [Google Scholar]
[9]. Beingessner DM, Nork SE, Angel J, Viskontas D, A fragment specific approach to Type IID Monteggia elbow fracture dislocationsJ Orthop Trauma 2011 25(7):414-19. [Google Scholar]
[10]. Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM, The posterior Monteggia lesionJ Orthop Trauma 1991 5(4):395-402. [Google Scholar]