Serratiopeptidase – A Cause for Spread of Infection
Prashanth Rajaram1, Abhishek Bhattacharjee2, Smriti Ticku3
1 Senior Lecturer, Department of Oral and Maxillofacial Surgery, Vokkaligara Sangha Dental College and Hospital, Bengaluru, Karnataka, India.
2 Postgraduate Student, Department of Oral and Maxillofacial Surgery, Vokkaligara Sangha Dental College and Hospital, Bengaluru, Karnataka, India.
3 Postgraduate Student, Department of Oral and Maxillofacial Surgery, Vokkaligara Sangha Dental College and Hospital, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abhishek Bhattacharjee, Postgraduate Student, Department of Oral and Maxillofacial Surgery, Vokkaligara Sangha Dental College and Hospital, Bengaluru, Karnataka, India
E-mail: drabhishekbhattacharjee10@gmail.com
Serratiopeptidase is a proteolytic enzyme that has been used for reducing inflammation, it has antiedemic, analgesic, fibrinolytic and caesinolytic properties. Serratiopeptidase is often used in oral surgery for its anti-inflammatory purpose after impaction surgery, maxillofacial trauma and infections but its use should be limited in cases of abscess due to its fibrinolytic activity. Here, we report a case of a buccal space abscess which had spread into deeper muscular layers after serratiopeptidase administration in a 32-year-old male without any systemic condition. Patient presented with a painful swelling on the right mid region of the face since seven days. Serratiopeptidase was discontinued. After routine blood investigation and ultrasonography, incision and drainage was done and the patient recovered after seven days of treatment.
Abscess, Buccal space, Proteolytic enzyme
Case Report
A 32-year-old male was referred to the Department of Oral and Maxillofacial Surgery with a chief complain of swelling, pain in the right middle third of the face and inability to open his mouth since one week. Patient gave a history of root canal treatment followed by extraction of the offending tooth one week back. Patient was given antibiotics and analgesic along with serratiopeptidase. However, there was no relief with this treatment rather the swelling gradually increased in size, thus, he was referred to our institute for further consultation.
The pain was throbbing in nature, continuous, radiating towards the ear and lower jaw, aggravated on taking food, on lying down and during night and relieved for sometime after taking analgesics. There was a positive history of fever for the last three days.
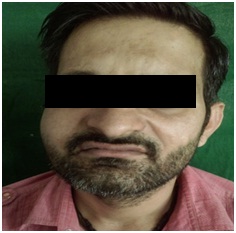
On examination, patient was moderately built and well nourished. Extraorally, a diffuse swelling measuring about 5x5cm was present, extending superioinferiorly from right infraorbital region to the upper lip and anterioposteriorly from right alar region to the anterior border of right masseter muscle. It was tender on palpation, hard in consistency and there was no local rise in temperature. There was obliteration of right nasolabial fold [Table/Fig-1]. On intraoral examination, there was trismus [Table/Fig-2], a dome shaped swelling was seen in the right buccal vestibule extending from vestibule with relation to tooth 17 into the buccal mucosa, measuring about 1x1cm, firm in consistency and tender on palpation [Table/Fig-3].
Pre-treatment frontal view of patient with buccal space abscess with obliteration of nasolabial fold on the right side.
Pre-treatment reduced mouth opening (1.6 cm).

Intraoral image showing dome shaped swelling with respect to tooth 17 from where the pus was drained.

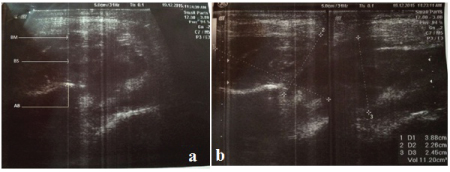
Patient was asked to stop serratiopeptidase and was adviced to take a combination of amoxicillin 500mg and potassium clavulanic acid 125mg two times daily, metronidazole 400mg three times daily, combination of chlorazoxazone, diclofenac sodium and paracetamol two times daily. Orthophantomogram was taken, but it did not reveal any significant finding [Table/Fig-4]. Ultrasound of the right infraorbital region revealed it to be a possible buccal space abscess which has extended into deeper tissue planes [Table/Fig-5]. The routine blood investigation revealed all parameters to be within normal range. Patient was reviewed the next day. There was no improvement in the mouth opening; swelling was still the same, so an incision and drainage was planned after taking a written consent.
OPG after extraction of tooth 17.

Ultrasonography images showing lesion in the region of buccal space suggesting of buccal space abscess. (a) - Ultrasonographic picture showing Buccinators Muscle (BM), Buccal Space (BS) containing the abscess and Alveolar Bone (AB). (b) – D1 depicts measurement in horizontal plane, D2 - depicts measurement in vertical plane, D3 - depicts measurement in oblique plane, total volume of the abscess was 11.20cm3.
A 1cm vestibular incision was given in the right upper buccal vestibule in the region of tooth 17 and pus was drained by Hilton’s method. The pus was sent for culture sensitivity test. The incision was left open and the patient was adviced to return if any further drainage occurs.
On the first post operative day, the swelling reduced and the mouth opening improved. The antibiotic was continued for four more days and mouth opening exercises were adviced. The culture sensitivity report revealed the organism to be group A streptococci. A week postoperatively the swelling resolved completely and mouth opening improved further. Patient was followed up for a month and he was symptom free [Table/Fig-6].
15th day post operative mouth opening (3 cm).

Discussion
Serratiopeptidase (serratiapeptase/serralysin/serrapeptase) is a pro-teolytic enzyme isolated from the non pathogenic enterobacteria serratio E15 found in silk worm. It has been successfully used since many years in Japan and Europe for pain and inflammation due to arthritis, trauma, surgery, sinusitis, bronchitis, carpel tunnel syndrome and painful swelling of the breast [1].
This enzyme has been used in maxillofacial surgery, in cases of trauma, impaction surgery, abscess. As in this case, serratiopeptidase was used for the patient who had a buccal space abscess.
Buccal space is the most commonly involved fascial space by a dental abscess [2]. Infections originating in either maxillary or mandibular teeth can spread into the buccal space, usually maxillary molars and premolars or mandibular premolar [3]. Many a times buccal space infection spreads in both direction i.e., in the buccal vestibule and drains intraorally or into buccal space, as buccintor is a partial barrier after odontogenic infection, and erodes the buccal cortical plate of the maxilla or mandible [4].
Serratiopeptidase is been used for management of such cases. Serratiopeptidase is a single chain protein with a molecular mass of about 55 KDa and a pI between 4.5 and 5.5. The primary structure of serralysin is also been determined [5]. The enzyme is absorbed through the intestine and transported directly into the blood stream [6]. Serratiopeptidase should be enterically coated or else it may get destroyed by acid in the stomach before it gets into small intestine [7,8]. This enzyme is believed to induce degradation of insoluble protein products like fibrin and inflammatory mediators. It reduces the viscosity of exudates facilitating drainage and alleviates pain by inhibiting the release of bradykinin [6,9].
An abscess is surrounded by haemorrhage, fibrin and inflammatory cells [10]. Around the necrosed part fibrin gets deposited in the form of membrane and thus, it also separates the dead part from the living. The wall of the abscess is formed by the effused and organised fibrin. Sometimes the fibrin wall is not strong enough; in those cases the pus finds its way into surrounding cellular texture and results into a diffuse abscess [11].
One of the important aspects of serratiopeptidase is its fibrinolytic activity [12]. In the indexed case a periapical abscess may have been present which on administration of serratiopeptidase caused the spread of abscess into deeper planes.
Other alternatives to serratiopeptidase could be bromelain obtained from pineapple, papain from papaya, rituside, trypsin, chymotrypsin etc., [13].
Conclusion
Serratiopeptidase is a systemic enzyme which has a wide range of functions but still its use can sometimes cause unwanted results, so its use should be limited in cases of abscess.
[1]. Nirale NM, Menon MD, Topical formulations of serratiopeptidase: Development and pharmacodynamic evaluationIndian journal of Pharmaceutical Science 2010 72(1):65-71. [Google Scholar]
[2]. Kerawala C, Newlands C, Oral and Maxillofacial SurgeryOxfordOxford University Press:374-375. [Google Scholar]
[3]. Tucker MR, Contemporary Oral and Maxillofacial Surgery5th edSt. Louis, MoMosby Elsevier:317-333. [Google Scholar]
[4]. Wray D, Stenhouse D, Lee D, Clark AJE, Textbook of general and oral surgeryEdinburgh [etc.]Churchill Livingstone:263-267. [Google Scholar]
[5]. Baumann U, Serralysin and related enzymes. In: barrett AJ, Rawlings ND, Woessner JF, editorsHandbook of Proteolytic Enzymes c2013 LondonElseiver academic press:864-865. [Google Scholar]
[6]. Bhagat S, Agarwal M, Roy V, Serratiopeptidase: A systematic review of the existing evidenceInternational Journal of Surgery 2013 11(3):209-17. [Google Scholar]
[7]. Moriya N, Nakata M, Nakamura M, Takaoka M, Iwasa S, Kato K, Intestinal absorption of serrapeptase™ (TSP) in ratsBiotechnol Appl Biochem 1994 20(Pt1):101-08. [Google Scholar]
[8]. Miyata K, Intestinal absorption of serratia peptidaseJ Appl Biochem 1980 2:111-16. [Google Scholar]
[9]. Mazzone A, Catalani M, Costanzo M, Drusian A, Mandoli A, Russo S, Evaluation of serratia peptidase in acute or chronic inflammation of otorhinolaryngology pathology: a multicentre, double-blind, randomized trial versus placeboJ Int Med Res 1990 18(5):379-88. [Google Scholar]
[10]. Beasle MB, The respiratory system. In: Rubin E, Reisner HM, editorsEssentials of Rubins pathology 2014 PhiladelphiaMichael Tully:326 [Google Scholar]
[11]. Hooper R, Physiology and general pathologyWilliam Augustus GUY Dr Hooper’s Physician’s Vade-mecum New edition enlarged with an outline of general Pathology and Therapeutics 1846 LondonH Renshaw:59-60. [Google Scholar]
[12]. Kakinuma A, Moriya N, Kawahara K, Sugino H, Repression of fibrinolysis in scalded rats by administration of serratia proteaseBiochemical Pharmacology 1982 3(18):2861-66. [Google Scholar]
[13]. Kaur R, Abmwani S, Mehta B, Trypsin, rutoside and bromelain alone and fixed dose combination: a natural, safer and effective anti-inflammatory agentJournal of Drug Delivery & Therapeutics 2014 4(1):108-10. [Google Scholar]