A South Indian Cadaveric Study About the Relationship of Hepatic Segment of Inferior Vena Cava with the Liver
Satheesha B Nayak1, Sudarshan Surendran2, Venu Madhav Nelluri3, Naveen Kumar4, Ashwini P Aithal5
1 Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus) Manipal University, Manipal, Karnataka, India.
2 Associate Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus) Manipal University, Manipal, Karnataka, India.
3 Senior Grade Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus) Manipal University, Manipal, Karnataka, India.
4 Assistant Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus) Manipal University, Manipal, Karnataka, India.
5 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus) Manipal University, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satheesha B Nayak, Melaka Manipal Medical College (Manipal Campus) Manipal University, Manipal, Karnataka-576104, India.
E-mail: nayaksathish@gmail.com
Introduction
Inferior Vena Cava (IVC) is the largest vein of the body. It runs vertically upwards in the abdomen, behind the liver. Its course is very constant in relation to liver. However, the amount of liver parenchyma related to it can vary from person to person. The data regarding its course and relations may be very useful to radiologists and surgeons during surgical treatment procedures for Budd-Chiari syndrome, liver carcinoma, liver transplant, venous cannulations and many other clinical procedures.
Aim
Aim of this study was to document the incidence of straight and curved course of IVC in relation to liver and also to note the pattern in which the liver tissue was related to the IVC.
Materials and Methods
In the current study, 95 adult cadaveric livers were observed; specifically to study the course/direction of the hepatic segment of IVC in relation to the liver. The extent of liver tissue related to various aspects of IVC was also studied. The course of the IVC was classified as straight and curved; and the relationship of liver parenchyma to the IVC was classified into 6 categories. The data was expressed as percentage incidence.
Results
In 78.94% cases, the IVC had a straight course in relation to the liver; whereas in 21.06% cases, it had a left sided curve (concavity of the curve towards the caudate lobe) in its course. In 6.31% cases, IVC travelled in a tunnel, being encircled by the liver parenchyma all around; in 36.84% cases, it was covered by liver parenchyma on front and sides so that only posterior surface of IVC was visible; in 3.15% cases it was covered by liver tissue on front, sides and also partly on posterior aspect; in 50.52% of cases, its anterior surface, sides and left edge of the posterior surface was covered by liver tissue; and in 3.15% cases it was covered only from the front by the liver tissue.
Conclusion
The data being reported here might be useful for surgeons while planning and executing various hepatic surgeries and also to the radiologists in planning and performing venous cannulation and therapeutic procedures. Since in many livers, the curvature of IVC was associated with enlarged caudate lobe, the curved IVC could hint about the increase in the volume of caudate lobe or liver itself.
Caudate lobe, Cavoplasty, Variation, Venoplasty
Introduction
Inferior Vena Cava (IVC) is the largest vein in the body. It drains the blood from the lower limbs, pelvis and abdomen into the right atrium of the heart. It begins in front of the body of fifth lumbar vertebra, by the union of right and left common iliac veins. It runs vertically upwards in front of the vertebral column, being on the right side of abdominal aorta. In relation to the liver, it lies in a groove on its posterior surface or within a tunnel, surrounded by the liver tissue. It pierces the central tendon of the diaphragm and ends by opening into the right atrium of the heart [1].
Course of IVC is very constant, there being very few reports on its variant course and relation to the liver. Knowledge of exact course and relations of IVC with respect to liver is very important to surgeons dealing with hepatic transplantation and lobectomy. It is also very useful for radiologists, anatomists and pathologists. Since there is very little data available on the course and relation of hepatic segment of IVC with liver, we undertook this study. The main objective of our study was to document the incidence of straight and curved course of IVC in relation to liver and also to note the pattern in which the liver tissue was related to the IVC.
Materials and Methods
This was a cross-sectional study, conducted in the month of February 2016. A total of 95 adult livers preserved in formalin tanks were used in this study. The livers belonged to cadavers, whose age ranged between 40 to 90 years. Gender wise separation was not done but approximately 10% of the livers belonged to female cadavers. Only healthy looking livers with presence of right and left lobes were used in the study. The livers with damaged lobes and obviously diseased ones were excluded from the study. In this study, we specifically observed the direction/course of hepatic segment of IVC (the part of IVC situated in the groove for IVC) and also noted its relationship with the liver. The direction/course of IVC was categorized as: i) Straight; and ii) Curved. The curved course was further classified as: i) curved to the left; and ii) curved to the right. The percentage of their incidence was calculated. As for its relationship with the liver, it was classified as: i) IVC completely encircled by liver tissue from all sides; ii) IVC covered by liver tissue on front and sides (right and left); iii) IVC covered by liver tissue on front, sides and both (right and left) edges of posterior surface; iv) IVC covered by liver tissue on front, sides and left edge of posterior surface; v) IVC covered by liver tissue on front, sides and right edge of posterior surface; vi) IVC covered by liver tissue only from the front. The percentage occurrence of these relations was calculated. Photographs of livers representing each of these categories were taken.
Results
A total of 75 livers (78.94%) had a straight course of IVC in relation to them. The IVC ascended vertically in relation to their posterior surfaces. In the remaining 20 (21.06%) livers it had a curved course. Among these 20 livers with curved course of IVC, all had a left sided curve. There was not even a single liver with a right sided curve of the IVC [Table/Fig-1].
Showing the number and percentage of straight and curved course of IVC. Total number of livers used in the study = 95.
| Direction/Course of IVC | Number of livers | Percentage (%) |
|---|
| Straight | 75 | 78.94 |
| Curved | 20 | 21.052 |
| Curved to the right | 0 | 0 |
| Curved to the left | 20 | 21.052 |
With respect to relationship of liver tissue with IVC, 6 livers (6.31%) had IVC totally encircled by liver tissue, there being no classic groove for IVC on the posterior surface of the liver. Thirty five livers (36.84%) had a normal groove for IVC, wherein, the liver tissue was related to the front and sides (right and left) of the IVC. In 3 livers (3.15%) the groove for IVC was very deep, where the liver tissue not only covered the front and sides of the IVC, but also covered the right and left edges of its posterior surface. It was interesting to note that in 48 livers (50.52%), the liver tissue covered the IVC from front, sides and the left edge of its posterior surface. In all these livers, it was the right edge of the caudate lobe of the liver encroaching on to the posterior surface of IVC. In 3 livers (3.15%) the IVC was totally outside the liver. In them, the anterior surface of IVC just touched the posterior surface of the liver. There was no groove for IVC in these livers. The hepatic veins just left the posterior surface and ended into the IVC in these livers [Table/Fig-2].
Table showing the extent of liver tissue covering the inferior vena cava. Total number of livers used in the study = 95.
| Relationshipof liver tissuewith IVC | Number of livers | Percentage (%) |
|---|
| Liver tissue encirclingIVC from all the sides | 6 | 6.31 |
| IVC covered by livertissue on front andsides (right and left) | 35 | 36.84 |
| IVC covered by livertissue on front, sidesand both (right and left)edges of posterior surface | 3 | 3.15 |
| IVC covered byliver tissue on front,sides and left edgeof posterior surface | 48 | 50.52 |
| IVC covered by livertissue on front,sides and rightedge of posteriorsurface | 0 | 0 |
| IVC covered byliver tissue onlyfrom the front | 3 | 3.15 |
The percentage statistics and the examples of curved course and relations of liver tissue to the IVC have been shown in [Tables/Fig-1,2,3,4,5,6,7,8,9 and 10].
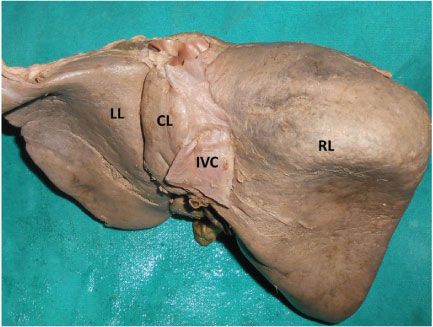
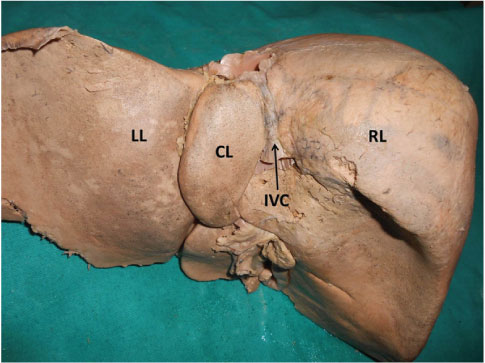
Photograph of posterior surface of the liver showing left sided curve of the inferior Vena Cava (IVC).
(LL – left lobe; CL – caudate lobe; RL – right lobe)
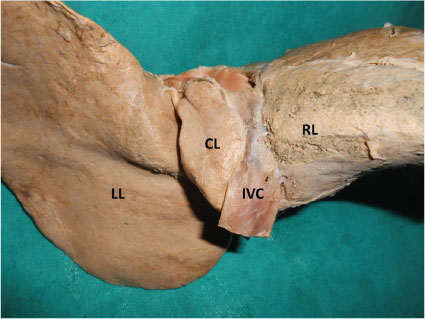
Photograph of posterior surface of the liver showing liver tissue incompletely covering the posterior surface of the inferior Vena Cava (IVC).
(LL – left lobe; CL – caudate lobe; RL – right lobe)
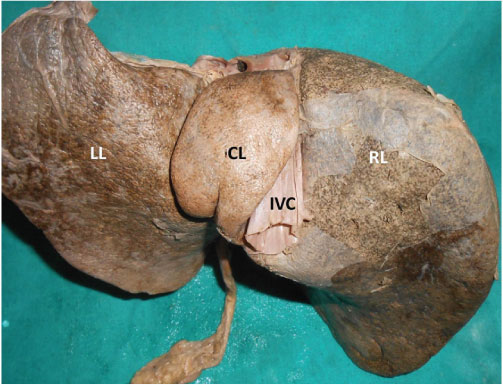
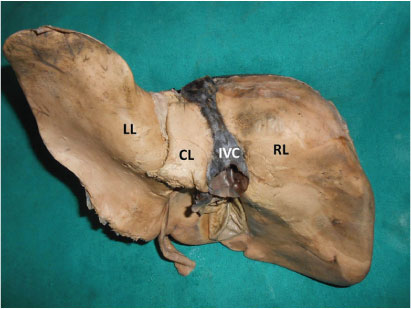
Photograph of posterior surface of the liver showing liver tissue encircling the inferior Vena Ccava (IVC).
(LL – left lobe; CL – caudate lobe; RL – right lobe)
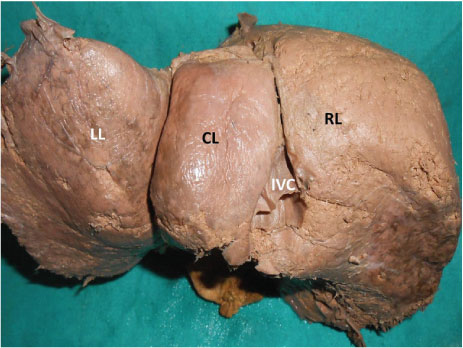
Photograph of posterior surface of the liver showing liver tissue encircling the posterior surface of the inferior Vena Cava (IVC).
(LL – left lobe; CL – caudate lobe; RL – right lobe)
Photograph of posterior surface of the liver showing liver tissue partially covering the posterior surface of the inferior vena cava (IVC) from left and right.
(LL – left lobe; CL – caudate lobe; RL – right lobe)
Photograph of posterior surface of the liver showing liver tissue partially covering the posterior surface of the inferior vena cava (IVC) from left and right.
(LL – left lobe; CL – caudate lobe; RL – right lobe)
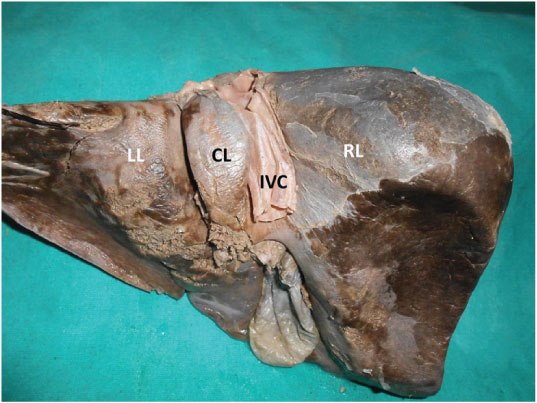
Photograph of posterior surface of the liver showing liver tissue covering the posterior surface of the inferior Vena Cava (IVC) from the left side only.
(LL – left lobe; CL – caudate lobe; RL – right lobe)
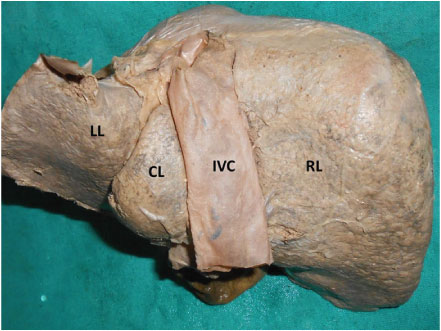
Photograph of posterior surface of the liver showing the inferior vena cava (IVC) which is covered by liver only on its front surface.
(LL – left lobe; CL – caudate lobe; RL – right lobe)
Discussion
Most of the reported variations of the IVC are its congenital anomalies. The popular among them include congenital absence of IVC [2] and its duplication [3–5]. Azygos continuation of IVC is another one among its noted anomalies [6]. The above said anomalies are usually associated with other anomalies, either of heart or any other viscera. As far as the course of IVC in relation to the liver is concerned, very few studies have been conducted in the past. In a study conducted by Sahni et al., the IVC formed a gentle left sided curve in 33.6% of livers. This study was conducted on livers of northwest Indian population [7]. Our study was on South Indian livers and we documented the left sided curvature of IVC in 21.06% of cases, which is lower compared to the northwest part of India. We could not get even a single case where the IVC had a curvature to the right. Even in literature survey, we could not find any reports on right sided curvature of the IVC in relation to the liver. In most of the livers with a left sided curvature, the right border of the caudate lobe was also curved. The possible reason for the curvature of the IVC was the extra growth of the right border of the caudate lobe. But in our study we did not see the associated enlargement of caudate lobe in most of the livers. Curvature in the IVC might cause complications in invasive procedures. A haemodialysis catheter may be misdirected when the IVC is curved [8]. The curved course also might cause problems in procedures like IVC filter placement [9] and IVC filter retrieval [10]. The radiologists may be in a disadvantage when the IVC is curved in procedures like Trans jugular Intrahepatic Portosystemic Shunt [11] and Trans-femoral Trans-caval Core-Needle Liver Biopsy [12].
The relationship of liver tissue to the surfaces of IVC is variable and systematic studies about this fact are lacking. IVC may range from being totally outside the liver tissue to totally within the liver, being surrounded by a ring of hepatic tissue. The classic text book description about relationship of IVC says that it is found in a deep groove called “groove for inferior vena cava”. We categorized this relationship of liver parenchyma with the IVC into 6 types. Type 1 is where the IVC was totally embedded in the liver parenchyma and Type 6 is where it was totally outside the liver. In the past, a study somewhat similar to our study was conducted by Bundi et al., on Kenyan population. In their study, IVC was found in a complete tunnel in 32.5% of the cases and in incomplete tunnel in 43.8% of the cases [13]. In our study, the incidence of complete tunnel for IVC was five times less compared to their study (6.31%). In some conditions like Budd-Chiari syndrome, the caudate lobe enlarges. In such cases, the IVC gets surrounded by the hypertrophied caudate lobe resulting in its placement in a complete tunnel [14,15]. All livers included in our study looked healthy without any signs of overgrowth of caudate lobe.
The knowledge of relationship of liver parenchyma with the hepatic segment of IVC is of importance in many clinical, radiological and surgical procedures. It is essential for the success of hepatic venoplasty and cavoplasty for Budd-Chiari syndrome with obstructed retro-hepatic IVC [16]. The understanding of the exact relationship of IVC with liver could be of utmost importance in venoplasty of hepatic veins during liver transplant surgeries [17], in hepatectomy with caudate lobe resection [18], Surgery for retro-hepatic caval thrombus [19], IVC resection and hemi-hepatectomy for leiomyosarcoma [20] also. Some other procedures which require the knowledge of precise relations of IVC with the liver and its possible variations include living donor liver transplant with IVC replacement [21], resection of IVC and liver in hepatic malignancy [22], extended right hepatectomy with a modified hanging maneuver [18] and laparoscopic caudate lobe resection [23]. The observations of the current study could be useful in surgeries like retro-hepatic vena caval thrombus removal [19], endovascular treatments like stent placements in cases of iatrogenic injuries of IVC [24], Intra hepatic porto-caval shunt placement [25] and in ultrasonography techniques to assess the infiltration of malignant cells into retrohepatic segment of IVC [26].
Limitation
One of the limitations of the current study is the small sample size. The same study can be extended to more than thousand livers. We did not study the segmental structure of the liver and correlate it with the IVC. Future studies could be designed in this direction.
Conclusion
The current study is a unique study since there are very few reports in literature on such studies. The data gathered through this study might help surgeons during partial or extended hepatectomy, caudate lobe excision, in hepatic venoplasty and cavoplasty, IVC filter placement and retrieval. It may also help in radiological procedures like trans-femoral, trans-caval core needle liver biopsy. Since in some of the livers, the curvature of IVC was associated with enlarged caudate lobe, the curved IVC could hint about the increase in the volume of caudate lobe or liver itself.
[1]. Standring S, Gray’s Anatomy 2008 40th EdLondonChurchill Livingstone:1075 [Google Scholar]
[2]. Cho BC, Choi HJ, Kang SM, Congenital absence of inferior vena cava as a rare cause of pulmonary thromboembolismYonsei Med J 2004 45:947-51. [Google Scholar]
[3]. Lataifeh AR, Anderson P, Duplication of inferior vena cava: a rare but clinically significant anatomical variationN Z Med J 2014 7;127(1405):84-86. [Google Scholar]
[4]. Ang WC, Doyle T, Stringer MD, Left-sided and duplicate inferior vena cava: a case series and reviewClin Anat 2013 26(8):990-1001. [Google Scholar]
[5]. Eid N, Ito Y, Otsuki Y, The left inferior vena cava: a surgically important variant tributary of left renal veinSurg Radiol Anat 2013 35(5):455-56. [Google Scholar]
[6]. Shen Y, Zhuang X, Xiao P, Dai W, Li Q, Oesophagectomy in a patient with azygos vein continuation of the inferior vena cava: report of a caseWorld J Surg Oncol 2015 13:242 [Google Scholar]
[7]. Sahni D, Harjeet Chawla YK, Indar Jit, Gross anatomy of the retrohepatic segment of the inferior vena cava in northwest IndiansIndian J Med Res 2006 124(1):63-70. [Google Scholar]
[8]. Akturk Y, OzbalGunes S, Akturk OM, Akcalar S, Hekimoglu B, A rare cause of abdominal pain: Catheter in the middle hepatic veinHaemodial Int 2016 20(2):E18-20. [Google Scholar]
[9]. Lee SH, Kim HK, Hwang JK, Kim SD, Park SC, Kim JI, Efficacy of retrievable inferior vena cava filter placement in the prevention of pulmonary embolism during catheter-directed thrombectomy for proximal lower-extremity deep vein thrombosisAnn Vasc Surg 2016 33:181-86. [Google Scholar]
[10]. Guzman AK, Zahra M, Trerotola SO, Raffini LJ, Itkin M, Keller MS, IVC filter retrieval in adolescents: experience in a tertiary pediatric centerPediatr Radiol 2016 46(4):534-40. [Google Scholar]
[11]. Pereira K, Carrion AF, Salsamendi J, Doshi M, Baker R, Kably I, Endovascular management of refractory hepatic encephalopathy complication of transjugular intrahepatic portosystemic shunt (TIPS): comprehensive review and clinical practice algorithmCardiovasc Intervent Radiol 2016 39(2):170-82. [Google Scholar]
[12]. Cynamon J, Shabrang C, Golowa Y, Daftari A, Herman O, Jagust M, Transfemoral transcaval core-needle liver biopsy: an alternative to transjugular liver biopsyJ Vasc Interv Radiol 2015 23:piiS1051-0443(15)01103-03 [Google Scholar]
[13]. Bundi KP, Ogeng’o JA, Hassanali J, Odula PO, Course of the hepatic inferior vena cava in a Kenyan populationClin Anat 2009 22(5):610-13. [Google Scholar]
[14]. Kikuchi Y, Yoshida H, Mamada Y, Taniai N, Mineta S, Yoshioka M, Huge caudate lobe of the liver due to Budd-Chiari syndromeJ Nippon Med Sch 2010 77(6):328-32. [Google Scholar]
[15]. Mehta RI, Mitchell DG, Kayler L, Doria C, Bergin D, Parker L, Inferior vena cava encirclement by caudate lobe hypertrophy: evaluation by MRI and CT and its impact on caval preservation during orthotopic liver transplantationAbdom Imaging 2010 35(3):322-27. [Google Scholar]
[16]. Dohi K, Asahara T, Fukuda Y, Marubayashi S, Yahata H, Haruta N, Successful treatment by simultaneous hepatic venoplasty and cavoplasty for Budd-Chiari syndrome with obstruction of retrohepatic inferior vena cavaSurgery 1993 113(5):574-79. [Google Scholar]
[17]. Thorat A, Jeng LB, Yang HR, Li PC, Li ML, Yeh CC, Outflow reconstruction for right liver allograft with multiple hepatic veins: "V-plasty" of hepatic veins to form a common outflow channel versus 2 or more hepatic vein-to-inferior vena cava anastomoses in limited retrohepatic spaceLiver Transpl 2016 22(2):192-200. [Google Scholar]
[18]. Perini MV, Coelho FF, Kruger JA, Rocha FG, Herman P, Extended right hepatectomy with caudate lobe resection using the hilar "en bloc" resection technique with a modified hanging maneuverJ Surg Oncol 2016 :18 [Google Scholar]
[19]. Polańska-Płachta M, Proczka R, Dudek M, Ostrowska M, Polański JA, Surgery for retrohepaticcaval thrombus in patients with advanced renal cell carcinoma: a case seriesWorld J Surg Oncol 2016 14(1):11 [Google Scholar]
[20]. Miles LF, Hu R, Jones RM, Carson S, McCall PR, Inferior vena cava resection and hemihepatectomy for leiomyosarcoma, utilizing cardiopulmonary bypass, in situ hepatic perfusion, and distal hypothermic circulatory arrestJ Cardiothorac Vasc Anesth 2016 30(1):169-75. [Google Scholar]
[21]. Yagci MA, Tardu A, Karagul S, Ince V, Ertugrul I, Kirmizi S, Living Donor Liver Transplantation With Vena Cava ReplacementTransplant Proc 2015 47(5):1453-57. [Google Scholar]
[22]. Hemming AW, Mekeel KL, Zendejas I, Kim RD, Sicklick JK, Reed AI, Resection of the liver and inferior vena cava for hepatic malignancyJ Am Coll Surg 2013 217(1):115-24. [Google Scholar]
[23]. Gringeri E, Boetto R, Bassi D, D’Amico FE, Polacco M, Romano M, Totally laparoscopic caudate lobe resection: technical aspects and literature reviewSurg Laparosc Endosc Percutan Tech 2014 24(6):e233-36. [Google Scholar]
[24]. Briggs CS, Morcos OC, Moriera CC, Gupta N, Endovascular treatment of iatrogenic injury to the retrohepatic inferior vena cavaAnn Vasc Surg 2014 28(7):1794.e13-15. [Google Scholar]
[25]. Yu SP, Chu GL, Yang JY, He L, Wang HQ, Direct intrahepatic portocaval shunt through transhepatic puncture via retrohepatic inferior vena cava: applied anatomical studySurg Radiol Anat 2009 31(5):325-29. [Google Scholar]
[26]. Kaneko T, Nakao A, Nomoto S, Endo T, Itoh S, Takagi H, Intracaval endovascular ultrasonography for preoperative assessment of retrohepatic inferior vena cava infiltration by malignant hepatic tumorsHepatology 1996 24(5):1121-27. [Google Scholar]