Early Eruption of Maxillary Pre Molar with Turner’s Hypoplasia in a 5-Year-Old Boy
Nitya Rai1, Shivani Mathur2, Meera Sandhu3, Vinod Sachdev4
1 Postgraduate Student, Department of Pedodontics and Preventive Dentistry, I.T.S Centre for Dental Studies and Research, Ghaziabad, Uttar Pradesh, India.
2 Reader, Department of Pedodontics and Preventive Dentistry, I.T.S Centre for Dental Studies and Research, Ghaziabad, Uttar Pradesh, India.
3 Professor, Department of Pedodontics and Preventive Dentistry, I.T.S Centre for Dental Studies and Research, Ghaziabad, Uttar Pradesh, India.
4 Professor and Head, Department of Pedodontics and Preventive Dentistry, I.T.S Centre for Dental Studies and Research, Ghaziabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nitya Rai, 4-A Tilak Bridge Railway Colony, Behind Pragati Maidan Metro Station, New Delhi-110001, India.
E-mail: dr.nityarai@gmail.com
Early eruption of permanent maxillary premolar appears to be a unique finding, at such an early chronological age. Untimely eruption of permanent maxillary premolar is discussed in a 5-year-old male patient. On intra oral examination grossly carious primary maxillary first molar (tooth number 54,64) were reported. The erupting teeth presented with a hypomineralized cusp tip. Extraction following space maintainer in 64 region was given. Pediatric dentist should consider these kinds of rarities in eruption pattern while examining a pediatric patient.
Grossly carious, Hypo mineralized enamel, Premature loss
Case Report
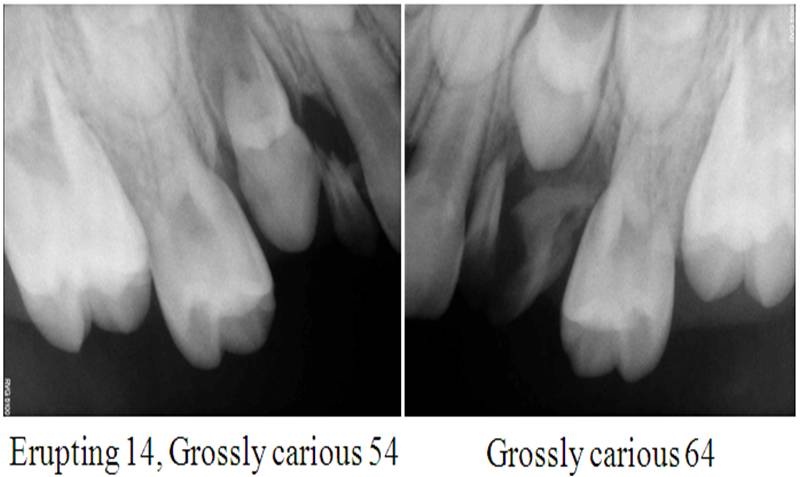
A 5-year-old male patient reported to the Department of Pedodontics and Preventive Dentistry, with the chief complaint of decayed tooth in upper left back region. There was no associated history of pain or swelling reported. Child was well nourished with no history of systemic illness. The intraoral examination revealed grossly decayed tooth no. 54,64 [Table/Fig-1]. Cusp of the erupting tooth no. 14 was seen through mucosa distal to tooth number 54. The cusp tip of tooth number 14 was hypo mineralized. Intra oral periapical radiograph showed erupting tooth number 14 with Nolla’s stage 6 [1] and root stumps with respect to tooth number 54, 64 [Table/Fig-2]. Extraction of root stumps (54, 64) was planned followed by band and loop space maintainer in relation to 64 tooth region. Follow-up was carried out at 1, 3, 6 months, during which the tooth showed asymptomatic eruption [Table/Fig-3]. Further recall visits were planned without any active dental intervention.
Intraoral view of grossly decayed tooth number 54, 64.

Intra oral periapical radiograph with erupting tooth number 14 and grossly carious tooth number 54, 64.
Maxillary pre molar showing asymptomatic eruption of tooth number 14 at 6 month follow-up and band and loop space maintainer i.r.t. tooth number 64.

Discussion
There is evidence that early loss of primary teeth can affect the eruption of successors, but the exact effects appear to be variable depending on the stage of development and time of extraction [1].
In the present case the erupting tooth appeared to be the first premolar. Till date, to our knowledge no case report of early eruption of pre molar with Turner’s hypoplasia is reported in a 5 year old child. However, there have been two case reported in literature of early eruption of permanent canine [2,3]. According to Posen early eruption of permanent teeth could be due to premature loss of primary teeth if the loss occurs within one year before eruption [4]. But if the extraction is done at a very young age, the eruption of teeth is delayed [5].
Maxillary second premolar normally erupts at the age of 10.69 ± 0.39 years in boys [6], with root completion at 12–13 years. In the present case, maxillary right first premolar was seen erupting in the oral cavity at 5 years of age, whereas the left first premolar showed crown completion with Nolla’s stage 5 [1] and with 6mm of bone cover over it.
Mineralization of premolars begins at age 2-2.5 years. In the present case root stump in relation to tooth no. 54 was reported. Long standing grossly carious tooth, could have resulted in an infectious insult to the permanent tooth bud during its mineralization, which would have caused hypomineralization of permanent enamel i.e., Turner’s hypoplasia.
Bauer studied autopsy material from a grossly carious tooth histologically, and reported that periapical inflammation of primary teeth was not contained by the development of a fibrous wall but spread diffusely through the bone around the buds of the successor, thereby affecting the protective layer of young enamel i.e., reduced enamel epithelium [7].
Here, in the present case, no definite history regarding caries progression or extraction of deciduous maxillary first molar (54) was reported. But as stated above, the eruption should have been delayed for the present case if there was premature loss of deciduous teeth due to grossly carious lesion, whereas accelerated eruption was observed. The accelerated eruption of teeth can be attributed to local factors such as genetics, gender, pre term birth, hormonal disturbance and systemic diseases like hyperthyroidism, rickets, cherubism, acute lymphocytic leukaemia and early onset periodontitis [8]. However, in the present case accelerated eruption could be attributed to early bone destruction which occurred as sequel to periapical infection in relation to primary molar, though no definite cause can be attributed to this unique oddity.
Conclusion
Any variation from the normal tooth eruption sequence or timing is not a normal occurrence in dental practice. Only a prepared eye and adequate knowledge can judge the presence of such discrepancy. Adequate knowledge, in order to diagnose such rarities at an appropriate time is of paramount importance especially for a pediatric dentist in order to preserve such teeth on long term basis and preventing untimely extraction and future malocclusion.
[1]. Sachan K, Sharma VP, Tandon P, Realibility of Nolla’s dental age assessment method for lucknow populationJ Pediatr Dent 2013 1:8-13. [Google Scholar]
[2]. Turnbull NR, Lai NN, Eruption of a permanent mandibular canine in a 5 year-old boyInt J Paediatr Dent 2003 13:117-20. [Google Scholar]
[3]. Madhu S, Early eruption of permanent caninesIndian J Dent Res 2012 23:428-30. [Google Scholar]
[4]. Posen AL, The effect of premature loss of deciduous molars on premolar eruptionAngle Orthod 1965 35:249-52. [Google Scholar]
[5]. McDonald RE, Avery DR, Dean JA, Dentistry for the Child and Adolescent 2004 8th edMosby:176-82. [Google Scholar]
[6]. Singh K, Gorea R K, Bharti V, Age estimation from eruption of permanent teethJ Indian Acad Forensic Med 2005 27(4):231-35. [Google Scholar]
[7]. Bauer WH, Effect of peri-apical process of deciduous teeth on the buds of permanent teethAm J Ortho Oral Surgery 1912 32:233-38. [Google Scholar]
[8]. Almonaitiene R, Balciuniene, Janina TutkuvieneFactors influencing permanent teeth eruption. Part one-general factorsStomatologija 2010 12(3):67-72. [Google Scholar]