Minor Salivary Gland Carcinoma of Hard Palate with CT Findings- Report of a Case
Amit Thorawat1, Prajwal K Shetty2, Bassel Tarakji3
1 Assistant Professor, Department of Oral and Maxillofacial Sciences, Al-Farabi College of Dentistry, Riyadh, Kingdom of Saudi Arabia.
2 Lecturer, Department of Oral Medicine and Radiology, Bapuji Dental College and Hospital, Davangere, Karnataka, India
3 Professor and Head, Department of Oral and Maxillofacial Sciences, Al-Farabi College of Dentistry, Riyadh, Kingdom of Saudi Arabia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amit Thorawat, Assistant Professor, Department of Oral and Maxillofacial Sciences, Al-Farabi College of Dentistry, Riyadh - 11691, Kingdom of Saudi Arabia.
E-mail: amitnaisa@gmail.com
Adenocystic, CT imaging, Microscopy, Perineural extension
A 58-year-old male patient presented to the Department of Oral Medicine and Radiology, with a complaint of pain in the right maxillary posterior region since one month. Patient had intermittent pain which was of throbbing type and temporarily relieved with medication. Past medical events were not significant.
Clinically, lesion extended from mid-palatine raphe medially to buccal vestibule with respect to 16, 17 and 18 tooth region laterally, 16 region anteriorly and extending posteriorly till soft palate. Lesion was approximately 3cm X 4cm in size. On palpation, margins of lesion were smooth palatally and irregular buccally, soft in consistency [Table/Fig-1]. Submandibular lymph nodes were tender, enlarged, fixed and firm bilaterally. Provisional diagnosis of carcinoma involving palate and maxillary tuberosity on right side was given. Differential diagnosis such as adenoid cystic carcinoma and mucoepidermoid carcinoma were included.
Tumor extended from mid-palatine raphe to buccal vestibule medio-laterally and 16 region till soft palate antero-posteriorly.

Lab investigations were advised and were within normal limits. Orthopantomograph findings were not informative and further patient was subjected to advanced radiographic procedures.
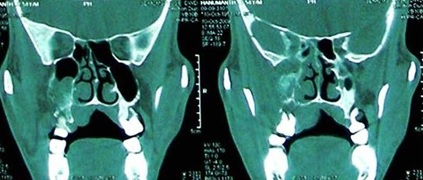
Coronal Computed Tomography (CT) sections revealed right sided space occupying lesion with infiltrative margins involving pterygopalatine fissure, naso and oro-pharyngeal mucosal space. There was associated permeated erosion of medial wall and floor of maxillary antrum [Table/Fig-2].
Coronal CT sections showing right sided space occupying lesion with infiltrative margins and permeated erosion of medial wall and floor of maxillary antrum.
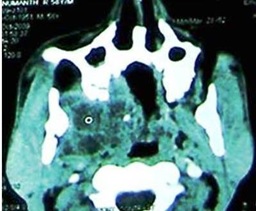
Axial CT sections revealed a mass measuring about 5.2cm X 4.4cm and shows extensive cystic/necrotic areas. Further there was involvement of deep masticator muscles (pterygoids and temporalis) [Table/Fig-3]. Coronal sections showing growth noted on right side extended from inferior orbital fissure to foramen ovale region (5.2cm X 4.4cm in size) [Table/Fig-4].
Axial CT sections showing extensive cystic/necrotic areas and involving deep masticator muscles (pterygoids and temporalis).
Coronal sections showing growth noted on right side extended from inferior orbital fissure to foramen ovale region (5.2cm X 4.4cm in size).

Chest X-ray was carried out to rule out distant metastasis to the lungs and appears to be clear.
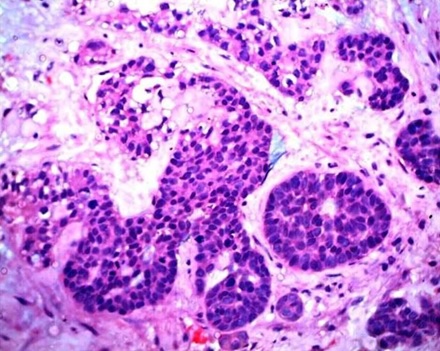
Patient underwent incisional biopsy and the mass was sent for histopathology. Histopathologic sections showed lobules of tumor epithelial cells arranged in solid and cribriform pattern and shows pseudocystic spaces filled with coagulum [Table/Fig-5]. Based on histopathology sections, diagnosis of adenoid cystic carcinoma was provided. Wide surgical excision with adjuvant radiotherapy was planned for the patient after the final histopathological diagnosis. Unfortunately our patient succumbed to the death two months after diagnosis.
Histopathologic sections showing lobules of tumor epithelial cells arranged in solid pattern and pseudocystic spaces filled with coagulum.
Discussion
Adenoid Cystic Carcinoma (ACC) occurs on the palate with the frequency of 8%-15% of all the palatal salivary neoplasms [1]. In the present case we documented a case of ACC affecting the palate, retromolar region, extending to the masticatory space and causing erosion of floor of maxillary antrum and pterygoid plates. ACC may be seen at any age, however in most of the cases individuals are middle aged or over [1]. Women are commonly affected. It can occur in any salivary gland site, but approximately 50% occur within the minor salivary glands [1]. Above findings were in favour of present case. Neoplasms emerging in the hard palate or maxillary antrum exhibits osseous destruction radiographically [1]. Above findings were in favour of present case such as permeated erosion of medial wall and floor of maxillary antrum on CT images.
Histopathology is considered to be the gold standard for the diagnosis of ACC. Advanced imaging modalities such as CT and Magnetic Resonance Imaging (MRI) also provide identical gravity in detection of perineural invasion with inclination to MRI because of its high soft tissue contrast [2].
Therapeutic intervention of ACC usually requires wide surgical excision of tumour, probably since the neoplastic cells expand well beyond the margins appearing clinically and radiographically and neoplasm undergoes both perineural invasion and spread [3]. Adjunctive radiotherapy of 6000 - 7500 cGy is generally provided post-operatively [4].
ACCs emerging from the palate and parotid gland have better prognosis where as from maxillary sinus and submandibular gland have worst prognosis [4]. Distant metastasis exist in 25%-50% of cases, even several years after primary treatment and lung is the most involved site [5].
ACC is the third more frequently detected neoplasm of submandibular and minor salivary glands, of malignant origin. Early diagnosis and intervention is of paramount importance because of its aggressiveness due to perineural spread and distant metastasis. Comprehensive head and neck evaluation should be obtained with adjunctive radiological investigations since the neoplasm has a tendency to spread perineurally to the cavernous sinus from cardinal sites along the path of three divisions of 5th cranial nerve. As recurrence and metastasis is very frequent with ACC, follow-up for a long period is necessary.
[1]. Neville Damm Allen Bouquot Oral and Maxillofacial Pathologysecond edition:426-28. [Google Scholar]
[2]. Shimamoto H, Chindasombatjaroen J, Kakimoto N, Kishino M, Murakami S, Furukawa S, Perineural spread of adenoid cystic carcinoma in the oral and maxillofacial regions: evaluation with contrast-enhanced CT and MRIDentomaxillofac Radiol 2012 41(2):143-51. [Google Scholar]
[3]. Robert E. Marx, Diane Stern, Oral and Maxillofacial Pathology, A rational for diagnosis and management:550-53. [Google Scholar]
[4]. Gumgum S, Oner B, Ustay C, Rapidly growing adenoid cystic carcinoma in mandible: A case reportOral Oncology Extra 2005 41:142-45. [Google Scholar]
[5]. Locati LD, Guzzo M, Bossi P, Massone PP, Conti B, Fumagalli E, Lung metastasectomy in adenoid cystic carcinoma of salivary glandOral Oncol 2005 41(9):890-94. [Google Scholar]