Introduction
Proximal humerus fractures comprise upto 4-5% of all fractures [1,2] and they are the most common of humerus fractures (45%). The increased incidence of proximal humerus fracture in older population is related to osteoporosis [3]. Proximal humerus fractures are the 3rd most common fracture in elderly patients [4,5]. Due to osteoporotic bones, fixation of proximal humerus fractures especially in the elderly patients is difficult and is associated with high complication rates [3].
Most common mechanism of injury is fall on an outstretched hand typically in older osteoporotic women. Younger patients typically present with proximal humerus fracture following high energy trauma such as motor vehicle accident [6]. An 80% of proximal humeral fractures are non or minimally displaced fractures - can be treated non-operatively [6]. Non operative treatment and fixation using K-wires lead to stiffness and decreased range of motion [7–9].
Optimal treatment of displaced or unstable fractures remains controversial. Various techniques, including open reduction and internal fixation with proximal humeral plates, intramedullary nailing, percutaneous or minimally invasive techniques with pins or screws and arthroplasty, have been described in literature [7,10–13]. Proximal Humerus Internal Locking System (PHILOS) plate was designed to provide angular stability especially in osteoporotic bones and to decrease the high complication rates associated with these fractures [8,9,11,14,15]. Non-locking plates like T-plates and cloverleaf plates have high failure rate in weak osteopenic bones and complication rates of upto 40% which includes subacromial impingement, screw loosening and avascular necrosis [16,17]. Various studies have reported no benefit of Tension Band wiring used in treatment of proximal humerus fractures [18,19]. Blade plates were later introduced which were a more rigid construct than previously used conventional plates but due to their larger profile and insufficient hold in osteoporotic bones, these plates have high failure rates [20]. Load sharing devices like intramedullary nails have reduced lever arm but due to insufficient purchase of proximal screws, were associated with high complication rates (31%) [21]. Loosening or backing out of the proximal screw was the most common complication seen. Results were satisfactory mainly in two part proximal humerus fractures [21,22].
Locking plates were designed giving consideration to the anatomy of proximal humerus. These plates have low profile and are biomechanically better suited for fixation of proximal humerus fracture [23]. They provide angular stability and locking screw anchorage in weak osteoporotic bones [24]. In addition to multiple locking screws, these plates also have small holes to fix rotator cuff with sutures or cerclage wires. This plate also provides multiple locking screw options which can be inserted in convergent/ divergent fashion for better pull-out strength [23,25]. Locking plates are being widely used now for fixation of proximal humerus fractures due to low complication rates [24–30].
Current study was undertaken to assess the functional outcome and complications associated with PHILOS plate used for treating displaced proximal humerus fracture and to compare the results of two approaches used for exposure.
Materials and Methods
This was a prospective study conducted at a tertiary level hospital, from September 2011 to December 2013, on 26 patients with fractures of the proximal humerus. These patients were managed with PHILOS plate. All fractures were classified as per the criteria of Neer classification [31] (a part is defined as displaced more than 1cm or with an angulation of more than 450). Study inclusion criteria were non compound fractures of proximal humerus in skeletally mature patients (18-70 years), fractures of proximal humerus Neer type 2,3,4 and fractures of the proximal humerus which are less than 1 month old. Exclusion criteria were pseudoarthrosis, pathological fracture, refracture, open fracture, fracture more than one-month-old and associated post-traumatic brachial plexus injury or peripheral nerve palsy.
All fractures were classified by single experienced trauma surgeon using plain radiographs (anteroposterior and transscapular view). Surgery was performed through a deltopectoral approach in 13 patients and through an anterolateral deltoid-splitting approach in 13 patients [Table/Fig-1]. The cases were operated by two Professors of the department (having a minimum 20 years of experience in the field of orthopaedics). Random allocation was done for every case, on alternate basis; with first case falling into deltoid splitting group and second case into deltopectoral and then third into deltoid spliting and henceforth. Each professor is attached to separate units and this pattern of randomisation was followed in these two units.
Evaluation on basis of age group of patients and average of constant shoulder score.
| NeerClassification | Total No.of Cases (n) | Deltoid SplittingApproach | DeltopectoralApproach |
|---|
| 2 Part | 5 | 2 | 3 |
| 3 Part | 12 | 7 | 5 |
| 4 Part | 9 | 4 | 5 |
| Total | 26 | 13 | 13 |
Postoperative Protocol
Three doses of intravenous antibiotics (first generation cephalosporin) were given to all the patients with first dose preoperatively and other two doses postoperatively. Shoulder pendulum, active assisted and passive exercises were started on first postoperative day. Active shoulder exercises were started once fracture union was evident on radiographs. Early mobilisation reduces pain in postoperative period and also motivates the patient to continue physiotherapy when discharged.
Clinical and radiographic evaluation
Functional assessment was done using Constant shoulder score [32]. Follow-up done at 1st, 3rd, 6th, & 12th weeks, 6 month and thereafter. The constant score was graded as poor (0-55 points), moderate (56-70), good (71-85), excellent (86-100). Radiographs were taken at each follow-up to evaluate fracture union and any complication like fracture displacement, loss of reduction or varus-valgus angulation was also noted. Failure was defined as backing out of the screw, plate breakage /pull-out, malunion, nonunion or avascular necrosis of humeral head. At final follow-up patients were evaluated by Constant score and radiographs were taken to assess for union or any complication mentioned above. Callus formation, presence of bridging osseous trabeculae and cortical continuity were considered as evidence of radiological union. Humeral head-shaft angle is the angle between humeral shaft axis and head. Head axis was taken as perpendicular to a line between the nearest lateral and medial points of the anatomic neck through the apex of the head. Head-shaft angle was further categorized as major varus (115 degrees), minor varus (115–124 degrees), normal (125–145 degrees), minor valgus (146–155 degrees), and major valgus (155 degrees) and compared between the immediate postoperative and last follow-up radiographs.
Statistical Analysis
Statistical analysis was performed using Graphpad software version 6.0 by statistical consultant with level of significance being 0.05. Chi-square test and Fisher-exact test was used to compare the results between two groups.
Results
The mean age of the patients in the present study was 46 years with minimum age patient of 22 year and maximum of 68 year. The male:female ratio was 1.36:1 with male predominance. Right upper extremity was involved more commonly with the ratio being 1.16:1 which was due to right handedness of the majority of the population. The predominant mode of injury was due to fall (53.8%) followed by road traffic accident (46.2%). The time interval between the injury and operation was approximately 7 days. The majority of fractures in the present study were Neer’s type 3 part (46.1%), followed by 4 part (34.7%) [Table/Fig-1]. Minimum number of patients was those with 2 part fracture (19.2%).
Of the 26 patients, all fractures united radiologically and clinically. No patient was lost to follow-up. Mean time to union was 12.3 weeks (9 –15 weeks) and mean constant score at final follow-up was 72.5. At the final follow-up 8 patients had good score, 10 patients had moderate score, 6 patients had excellent outcome and 2 patients had poor outcome according to constant score. Age-wise average constant score distribution is shown in [Table/Fig-2]. We compared the results in 2 part, 3 part and 4 part fracture types as per Constant score and time to union. Average Constant score in 2 part fracture was 80.8, in 3 part was 71.3, and in 4 part was 69.3 [Table/Fig-3]. There was no significant difference in outcomes between patients with 3-part and 4-part fractures (p-value=0.6). Constant score decreased as the degree of comminution increased. Radiographs of a patient of two part proximal humerus fracture showing good fracture union is shown in [Table/Fig-4]. Although proximal humerus fracture has maximum age incidence in elderly osteoporotic bone but in present study maximum number of cases were in age group 50-60 years and least in 60-70 years. During the follow-up, 4 complications (15.4%) were encountered, 2 cases of varus malunion (minor varus), 1 case of wound infection and 1 case of screw cut-out. Two cases required reoperation, one patient had wound infection at 5th postoperative day for which debridement was done and the other had screw cut out at 8 weeks post surgery for which screw removal was done. These fractures healed uneventfully after debridement and screw removal. Other two cases healed in varus malunion but were asymptomatic.
Distribution of cases as per neer classification and approaches used.
| Age (Yrs) | Total No. of Patients (n) | Constant Shoulder Score |
|---|
| 20-30 | 4 | 84 |
| 30-40 | 5 | 67.2 |
| 40-50 | 3 | 74 |
| 50-60 | 10 | 72.2 |
| 60-70 | 4 | 67 |
Evaluation on basis of neer type and constant shoulder score.
| Neer Type | Deltoid SplittingGroup | DeltopectoralGroup | Avg Constant ShoulderScore of Neer Type |
|---|
| 2 Part | 79 | 82 | 80.8 |
| 3 Part | 70.6 | 74 | 71.3 |
| 4 Part | 67.5 | 70.8 | 69.3 |
| Total | 70.9 | 74 | 72.5 |
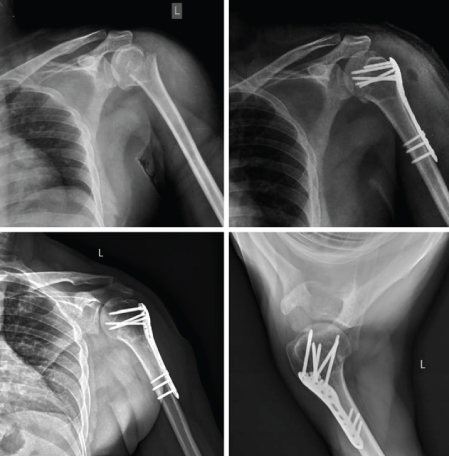
Preoperative, immediate postoperative, follow-up anteroposterior and lateral radiograph at 1 year of 2 part proximal humerus fracture of 24-year-male showing good union.
Twenty six patients were treated by PHILOS plate with 13 patients was operated by deltopectoral and 13 patients by deltoid splitting approach. Mean Constant score in deltosplitting approach was 70.9 and 74 in deltopectoral group (p-value= 0.54) [Table/Fig-3]. No significant difference existed in Constant score in 2 approaches. The average time to union in Deltoid splitting approach was 12.1 weeks (9 – 15 weeks) and in Deltopectoral approach was 12.6 weeks (9 – 15 weeks). However, when compare the composite score in reference with age group (<50 and >50), the difference between the group was significant (p=.032) between two groups on basis of Nonparametric Mann Whitney Score. Clinical examination at follow-up revealed no evidence of axillary nerve palsy such as atrophy or loss of weakness in either group. One early-onset wound infection in deltopectoral group, none occurred in the deltoid-splitting group (p=0.29) was treated successfully by debridement and antibiotic therapy. One screw cut-out occurred in the deltopectoral group, which required a surgery to remove the screw. There were two cases with varus malunion (8%) [Table/Fig-5], 1(3.8%) in the deltoid-splitting group and 1(3.8%) in the deltopectoral group. However, no significant difference existed between groups in terms of complications (p>0.05) and all fractures were united.
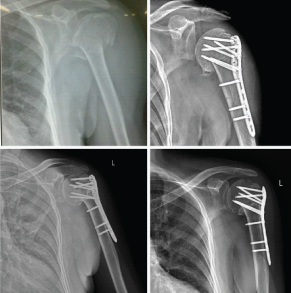
Preoperative, immediate postoperative, follow-up anteroposterior radiograph at 6 months and 18 months of 3 part proximal humerus fracture in 50- year-male showing varus malunion.
Discussion
The present study aimed at evaluating clinical outcome after PHILOS plate fixation and to evaluate the potential complications during the follow-up period. The early results of PHILOS plate fixation have been reported in the study. This study also supports the hypothesis that surgical approach for plate fixation has no crucial influence on outcome.
Patients with proximal humerus fractures have been on the rise in the past few decades due to increase in the proportion of population with osteoporosis as the age advances. It has been shown in various studies that osteoporosis adversely affects the anchorage of internal fixation and leads to increased failure rates [33,34]. Patients who have 3 part or 4 part proximal humerus fractures, are more prone for poor clinical results and high failure rates especially when the fixation has been performed with conventional non-locking plates [17,35].
Various fixation methods have been used in the past for treatment of proximal humeral fractures which showed variable outcomes. In a study by Sadowski et al., fixation with PlantTan plates resulted in 100% complications especially in elderly osteoporotic bones, with penetration of the proximal screw being the most common complication [36]. Various studies have reported outcomes similar to non-operative group in patients treated with Tension band wiring [18,19]. Similarly, AO-T plates and cloverleaf plates were shown to give poor results in osteoporotic bones [16,17]. Complications like screw loosening, subacromian impingement and avascular necrosis of upto 40% has been reported with these plates [16,17]. Polarus nail was later introduced for treatment of these fractures [21,37] but a high complication rate was seen (proximal screw loosening, revision surgery and lateral metaphyseal comminution predisposing to implant failure) [38].
Locking plates provide better stability than conventional plates that were used in the past [39–41]. Many authors have demonstrated that they give better functional outcome and also avoid complications [1,9,11,42–44]. Because of this the use of locking plates has become the standard protocol for open reduction and internal fixation of proximal humerus fractures particularly in the elderly patients with poor bone quality [9,11,44]. Besides this, the functional outcome also depends upon the stability provided by the implant. In the locking plate system, all the forces are transmitted from the bone via the Locking head screws to the blade and vice versa. Hence, the fixed angle plates enable a gain in the torsional stiffness and stability and may therefore promote a superior outcome and less chance of complications like cut-out of the screws and plates, non-union, avascular necrosis, and fractures distal to the plate [45].
In this study, mean constant score at the final follow-up was 72.5. The average time to union was 12.3 weeks (9–15 weeks). The average time to union in Deltoid splitting approach was 12.1 weeks (9-15 weeks) and in Deltopectoral approach was 12.6 weeks (9 – 15 weeks). Average time to union in 2 part fractures was 11.2 weeks, in 3 part it was 12.5 weeks and in 4 part 12.6 weeks. Complications (screw cut out, varus malunion, infection) occurred in total 4 cases (15.4%).
In a study conducted by the Frankhauser et al., proximal humerus fractures were treated with Locking Proximal Humerus Plate (LPHP) [11]. They observed no non-union and reported a low incidence of re-operations (n=2), the Mean Constant – Murley score was 74.6 after 12 months. Bjorkenheim et al., in their study reviewed 72 patients treated with Locking Compression plate [9]. At final follow-up, 36 patients reported excellent outcome. A total of 31 patients reported moderate outcome and 5 patients had poor results. Koukakis et al., reviewed 20 patients in their study and showed favourable results with surgical treatment of proximal humerus fractures using a Locking Compression Plate [44]. After a mean follow-up of 16 months, the mean constant score was 76.1 the results did not differ significantly with age but in our study younger patients had better outcome. Hente et al., studied 31 patients with displaced 3-part and 4-part fractures of the proximal humerus treated with Locking Compression Plate [46]. After a mean follow-up period of 18.5 months, the mean constant score was 76.
Present series had complication rate similar to the study conducted by Martinez et al., which after a follow-up of 58 patients had no case of wound infection, avascular necrosis, or loss of fixation, only 2 patients (3.44%) had axillary nerve palsy which recovered spontaneously in 3 months and 5 patients complained of impingement symptoms (8.62%) [47]. Similarly, in a prospective study by Roderer et al., implant related complications (plate impingement, screw perforation, loosening of screw) were seen in 9 cases (17%) [48]. Study conducted by Nourozi et al., had similar outcome with 15% complication rate in a study conducted in 37 patients with 1 case of AVN, 2 case of wound infection and 3 case of malunion [49]. According to Charalambous et al., out of 25 cases, 5 required revision because of implant failure or non-union [50]. Out of 25 implants, 4 had screw protrusion into the gleno-humeral joint, 4 had screw loosening and backing out, and 1 plate broke without further trauma [50]. PHILOS is an effective system for stabilizing these fractures but the potential complications should also be taken care of. In another study, Rose et al., reported 0 infections, 4 nonunions, and 0 cases of AVN in 16 patients at 12-month follow-up [51].
Two major approaches have been described for the surgical management of proximal humerus fractures. The Delto-pectoral approach is the procedure of choice [52,53]. However, several surgeons agree that this approach may not be the best option when performing an angular stable plate fixation of a proximal humerus fracture [53–57]. However, it involves substantial soft-tissue dissections, including partial release of the deltoid muscle, retraction of the deltoid muscle and the humeral manipulation to access the lateral aspect of humerus. As a result it becomes difficult to gain the correct drill angle using a standard Delto-Pectoral approach. Therefore this approach is not the best when performing an angular stable plate fixation of a proximal humeral fracture [58,59]. Recently the Deltoid Splitting approach has become more popular. It is a minimally invasive approach used for the osteosynthesis of proximal humeral fractures in a sliding-in technique. Plating through a minimally invasive anterolateral acromial approach allows the direct access to the appropriate plating zone, a bare spot between the humeral head-penetrating vessels from the anterior and posterior circumflex artery. Further this approach prevents deltoid release and also avoids exposure of anterior blood supply and thus will prevent devitalisation of fracture fragments [60].
The current study showed no difference in outcome in fracture proximal humerus treated with locking plate in deltoid splitting and deltopectoral group in terms of Constant score and complications. Constant score of 74 in deltopectoral and 70.9 in deltosplitting group are comparable in both the groups and with other studies also. Previously, possibility of axillary nerve during plate fixation through deltoid splitting approach is been seen as a limitation of this approach [55,61–64] but in the current study no axillary nerve palsy was noted. Laflamme et al., Hepp et al., [65,66], Gardener et al., also found no lesions to the axillary nerve [55,57].
Limitation
There are two major limitations to this study. First, the number of patients was less and the mean time to follow-up was short. We suggest a large sample size and longer follow-up period will further validate the results obtained here in.
Conclusion
PHILOS plate fixation gives good functional outcomes in proximal humerus fractures with early mobilisation. Our study has shown no significant differences between the two approaches. Also there was no high predisposition to axillary nerve injury seen with deltoid splitting approach.
[1]. Helmy N, Hintermann B, New trends in the treatment of proximal humerus fracturesClin Orthop 2006 442:100-08. [Google Scholar]
[2]. Kristiansen B, Bartod G, Bredesen J, Epidemiology of proximal humerus fracturesActa Orthop Scand 1987 58(1):75-77. [Google Scholar]
[3]. Kannus P, Palvanen M, Niemi S, Osteoporotic fractures of the proximal humerus in elderly Finnish persons: sharp increase in 1970-1998 and alarming projections for the new millenniumActa Orthop Scand 2000 71:465-70. [Google Scholar]
[4]. Lind T, Kroner K, Jensen J, The epidemiology of fractures of proximal humerusArch Orthop Trauma Surg 1989 108:285-87. [Google Scholar]
[5]. Nguyen TV, Center JR, Sambrook PN, Symptomatic fracture incidence in elderly men and women: the Dubbo Osteoporosis Epidemiology StudyAm J Epidemiol 2001 153:587-595. [Google Scholar]
[6]. Lannoti JP, Ramsey ML, Williams GR, Warner JP, Non prosthetic management of proximal humerus fracturesJBJS (Am) 2003 85:1578-93. [Google Scholar]
[7]. Resch H, Povacz P, Frohlich R, Wambacher M, Percutaneous fixation of three- and four-part fractures of the proximal humerusJ Bone Joint Surg Br 1997 79(2):295-300. [Google Scholar]
[8]. Lungershausen W, Bach O, Lorenz CO, Locking plate osteosynthesis for fractures of the proximal humerus [in German]Zentralbl Chir 2003 128(1):28-33. [Google Scholar]
[9]. Björkenheim JM, Pajarinen J, Savolainen V, Internal fixation of proximal humeral fractures with a locking compression plate: a retrospective evaluation of 72 patients followed for a minimum of 1 yearActa Orthop Scand 2004 75(6):741-45. [Google Scholar]
[10]. Mittlmeier TW, Stedtfeld HW, Ewert A, Beck M, Frosch B, Gradl G, Stabilization of proximal humeral fractures with an angular and sliding stable antegrade locking nail (Targon PH)J Bone Joint Surg Am 2003 85(suppl 4):136-46. [Google Scholar]
[11]. Fankhauser F, Boldin C, Schippinger G, Haunschmid C, Szyszkowitz R, A new locking plate for unstable fractures of the proximalhumerusClin Orthop Relat Res 2005 430:176-81. [Google Scholar]
[12]. Wanner GA, Wanner-Schmid E, Romero J, Internal fixation of displaced proximal humeral fractures with two one-third tubular platesJ Trauma 2003 54(3):536-44. [Google Scholar]
[13]. Schmal H, Klemt C, Sudkamp NP, Evaluation of shoulder arthroplasty in treatment of four-fragment fractures of the proximal humerusUnfallchirurg 2004 107(7):575-82. [Google Scholar]
[14]. Gallo RA, Zeiders GJ, Altman GT, Two-incision technique for treatment of complex proximal humerus fracturesJ Orthop Trauma 2005 19:734-40. [Google Scholar]
[15]. Plecko M, Kraus A, Internal fixation of proximal humerus fractures using the locking proximal humerus plateOper Orthop Traumatol 2005 17:25-50. [Google Scholar]
[16]. Rees J, Hicks J, Ribbans W, Assessment and management of three-and four-part proximal humeral fracturesClin Orthop Relat Res 1998 353:18-29. [Google Scholar]
[17]. Kristiansen B, Christensen SW, Plate fixation of proximal humeral fracturesActa Orthop Scand 1986 57(4):320-23. [Google Scholar]
[18]. Ilchmann T, Ochsner PE, Wingstrand H, Jonsson K, Non-operative treatment versus tension-band osteosynthesis in three- and four-part proximal humeral fractures. A retrospective study of 34 fractures from two different trauma centersInt Orthop 1998 22(5):316-20. [Google Scholar]
[19]. Zyto K, Ahrengart L, Sperber A, Törnkvist H, Treatment of displaced proximal humeral fractures in elderly patientsJ Bone Joint Surg Br 1997 79(3):412-17. [Google Scholar]
[20]. Drosdowech DS, Faber KJ, Athwal GS, Open reduction and internal fixation of proximal humerus fracturesOrthop Clin North Am 2008 39(4):429-39. [Google Scholar]
[21]. Rajasekhar C, Ray PS, Bhamra MS, Fixation of proximal humeral fractures with the Polarus nailJ Shoulder Elbow Surg 2001 10(1):7-10. [Google Scholar]
[22]. Young AA, Hughes JS, Locked intramedullary nailing for treatment of displaced proximal humerus fracturesOrthop Clin North Am 2008 39(4):417-28. [Google Scholar]
[23]. Strohm PC, Helwig P, Konrad G, Südkamp NP, Locking plates in proximal humerus fracturesActa Chir Orthop Traumatol Cech 2007 74(6):410-15. [Google Scholar]
[24]. Moonot P, Ashwood N, Hamlet M, Early results for treatment of three- and four-part fractures of the proximal humerus using the PHILOS plate systemJ Bone Joint Surg Br 2007 89(9):1206-09. [Google Scholar]
[25]. Thanasas C, Kontakis G, Angoules A, Limb D, Giannoudis P, Treatment of proximal humerus fractures with locking plates: a systematic review [published online ahead of print September 12, 2009]J Shoulder Elbow Surg 2009 18(6):837-44. [Google Scholar]
[26]. Konrad G, Bayer J, Hepp P, Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Surgical techniqueJ Bone Joint Surg Am 2010 92(suppl 1 pt 1):85-95. [Google Scholar]
[27]. Micic ID, Kim KC, Shin DJ, Analysis of early failure of the locking compression plate in osteoporotic proximal humerus fractures [published online ahead of print October 3,2009]J Orthop Sci 2009 14(5):596-601. [Google Scholar]
[28]. Hirschmann MT, Quarz V, Audigé L, Internal fixation of unstable proximal humerus fractures with an anatomically preshaped interlocking plate: a clinical and radiologic evaluationJ Trauma 2007 63(6):1314-23. [Google Scholar]
[29]. Gardner MJ, Weil Y, Barker JU, Kelly BT, Helfet DL, Lorich DG, The importance of medial support in locked plating of proximal humerus fracturesJ Orthop Trauma 2007 21(3):185-91. [Google Scholar]
[30]. Brunner F, Sommer C, Bahrs C, Open reduction and internal fi xation of proximal humerus fractures using a proximal humeral locked plate: a prospective multicenter analysisJ Orthop Trauma 2009 23(3):163-72. [Google Scholar]
[31]. Neer CS 2nd, Displaced proximal humeral fractures. I. Classification and evaluationJ Bone Joint Surg Am 1970 52:1077-89. [Google Scholar]
[32]. Constant CR, Cork: MCH Thesis 1986 University CollegeAge related recovery of shoulder function after injury [Google Scholar]
[33]. Barrios C, Brostrom LA, Stark A, Walheim G, Healing complications after internal fixation of trochanteric hip fractures: the prognostic value of osteoporosisJ Orthop Trauma 1993 7(5):438-42. [Google Scholar]
[34]. Giannoudis PV, Schneider E, Principles of fixation of osteoporotic fracturesJ Bone Joint Surg Br 2006 88(10):1272-78. [Google Scholar]
[35]. Paavolainen P, Bjorkenheim JM, Slatis P, Paukku P, Operative treatment of severe proximal humeral fracturesActa Orthop Scand 1983 54(3):374-79. [Google Scholar]
[36]. Sadowski C, Riand N, Stern R, Hoffmeyer P, Fixation of fractures of the proximal humerus with the PlantTan Humerus Fixator Plate: early experience with a new implantJ Shoulder Elbow Surg 2003 12:148-51. [Google Scholar]
[37]. Adedapo AO, Ikpeme JO, The results of internal fixation of three- and four-part proximal humeral fractures with the Polarus nailInjury 2001 32:115-21. [Google Scholar]
[38]. Agel J, Jones CB, Sanzone AG, Camuso M, Henley MB, Treatment of proximal humeral fractures with Polarus nail fixationJ Shoulder Elbow Surg 2004 13:191-95. [Google Scholar]
[39]. Weinstein DM, Bratton DR, Ciccone WJ II, Elias JJ, Locking plates improve torsional resistance in the stabilization of three-part proximal humeral fracturesJ Shoulder Elbow Surg 2006 15(2):239-43. [Google Scholar]
[40]. Walsh S, Reindl R, Harvey E, Berry G, Beckman L, Steffen T, Biomechanical comparison of a unique locking plate versus a standard plate for internal fixation of proximal humerus fractures in a cadaveric modelClin Biomech 2006 21(10):1027-31. [Google Scholar]
[41]. Siffri PC, Peindl RD, Coley ER, Norton J, Connor PM, Kellam JF, Biomechanical analysis of blade plate versus locking plate fixation for a proximal humerus fracture: comparison using cadaveric and synthetic humeriJ Orthop Trauma 2006 20(8):547-54. [Google Scholar]
[42]. Kettler M, Biberthaler P, Braunstein V, Zeiler C, Kroetz M, Mutschler W, Treatment of proximal humeral fractures with the PHILOS angular stable plate. Presentation of 225 cases of dislocated fracturesUnfallchirurg 2006 109(12):1032-40. [Google Scholar]
[43]. Sudkamp N, Bayer J, Hepp P, Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Results of a prospective, multicenter, observational studyJ Bone Joint Surg Am 2009 91(6):1320-28. [Google Scholar]
[44]. Koukakis A, Apostolou CD, Taneja T, Korres DS, Amini A, Fixation of proximal humerus fractures using the PHILOS plate: early experienceClin Orthop Relat Res 2006 442:115-20. [Google Scholar]
[45]. Lill H, Hepp P, Korner J, Kassi JP, Verheyden AP, Josten C, Proximal humeral fractures: how stiff should an implant be? A comparative mechanical study with new implants in human specimensArch Orthop Trauma Surg 2003 123:74-81. [Google Scholar]
[46]. Hente R, Kampshoff J, Kinner B, Füchtmeier B, Nerlich M, Treatment of dislocated 3- and 4-part fractures of the proximal humerus with an angle-stabilizing fixation plate[Article in German] Unfallchirurg 2004 107:769-82. [Google Scholar]
[47]. Martinez AA, Cuenca J, Herrera A, Philos plate fixation for proximal humeral fracturesJ Orthop Surg 2009 17(1):10-4. [Google Scholar]
[48]. Roderer G, Erhardt J, Graf M, Kinzl L, Gebhard F, Clinical results for minimally invasive locked plating of proximal humerus fracturesJ Orthop Trauma 2010 24(7):400-06. [Google Scholar]
[49]. Norouzi M, Naderi MN, Komasi MH, Sharifzadeh SR, Shahrezaei M, Eajazi A, Clinical results of using the proximal humeral internal locking system plate for internal fixation of displaced proximal humeral fracturesAm J Orthop 2012 41(5):E64-E68. [Google Scholar]
[50]. Charalambous CP, Siddique I, Valluripalli K, Proximal humeral internal locking system (PHILOS) for the treatment of proximal humeral fracturesArch Orthop Trauma Surg 2007 127:205-10. [Google Scholar]
[51]. Rose PS, Adams CR, Torchia ME, Locking plate fixation for proximal humeral fractures: initial results with a new implantJ Shoulder Elbow Surg 2007 16(2):20-27. [Google Scholar]
[52]. Habermeyer P, Lehmann L, Rotatorenmanschette, Rotatorenintervall und langeBizepssehne. In: Habermeyer P, edSchulterchirurgie 2002 Munich, GermanyUrban & Fischer:333-374. [Google Scholar]
[53]. Rommens PM, Blum J, Runkel M, Retrograde nailing of humeral shaft fracturesClin Orthop Relat Res 1998 350:26-39. [Google Scholar]
[54]. Bathis H, Tingart M, Bouillon B, Tiling T, Surgical treatment of proximal humeral fractures. Is the T-plate still adequate osteosynthesis procedureZentralbl Chir 2001 126(3):211-16. [Google Scholar]
[55]. Gardner MJ, Griffith MH, Dines JS, Briggs SM, Weiland AJ, Lorich DG, The extended anterolateral acromial approach allows minimally invasive access to the proximal humerusClin Orthop Relat Res 2005 434:123-29. [Google Scholar]
[56]. Sturzenegger M, Fornaro E, Jakob RP, Results of surgical treatment of multifragmented fractures of the humeral headArch Orthop Trauma Surg 1982 100(4):249-59. [Google Scholar]
[57]. Gardner MJ, Boraiah S, Helfet DL, Lorich DG, The anterolateral acromial approach for fractures of the proximal humerusJ Orthop Trauma 2008 22(2):132-37. [Google Scholar]
[58]. Hawkins RJ, Kiefer GN, Internal fixation techniques for proximal humeral fracturesClin Orthop Relat Res 1987 223:77-85. [Google Scholar]
[59]. Martini M, The sub-deltoid approach to the metaphyseal region of the humerusJ Bone Joint Surg Am 1976 58(3):377-79. [Google Scholar]
[60]. Gardner MJ, Voos JE, Wanich T, Helfet DL, Lorich DG, Vascular implications of minimally invasive plating of proximal humerus fracturesJ Orthop Trauma 2006 20(9):602-07. [Google Scholar]
[61]. Apaydin N, Tubbs RS, Loukas M, Duparc F, Review of the surgical anatomy of the axillary nerve and the anatomic basis of its iatrogenic and traumatic injurySurg Radiol Anat 2010 32(3):193-201. [Google Scholar]
[62]. Kontakis GM, Steriopoulos K, Damilakis J, Michalodimitrakis E, The position of the axillary nerve in the deltoid muscle. A cadaveric studyActa Orthop Scand 1999 70(1):9-11. [Google Scholar]
[63]. Bono CM, Grossman MG, Hochwald N, Tornetta P III, Radial and axillary nerves. Anatomic considerations for humeral fixationClin Orthop Relat Res 2000 373:259-64. [Google Scholar]
[64]. Traxler H, Surd R, Laminger KA, Windisch A, Sora MC, Firbas W, The treatment of subcapitalhumerus fracture with dynamic helix wire and the risk of concommitant lesion of the axillary nerveClin Anat 2001 14(6):418-23. [Google Scholar]
[65]. Laflamme GY, Rouleau DM, Berry GK, Beaumont PH, Reindl R, Harvey EJ, Percutaneous humeral plating of fractures of the proximal humerus: results of a prospective multicenter clinical trialJ Orthop Trauma 2008 22(3):153-58. [Google Scholar]
[66]. Hepp P, Theopold J, Voigt C, Engel T, Josten C, Lill H, The surgical approach for locking plate osteosynthesis of displaced proximal humeral fractures influences the functional outcomeJ Shoulder Elbow Surg 2008 17(1):21-28. [Google Scholar]