Cast Partial Denture with Cekapreci-Sagix Extra Coronal Attachment and Obturator for Rehabilitation of Patient with Maxillary Defect
Deepak Macchindra Vikhe1, Veena Raghottam Saraf2, Gangadhar Siddappa Angadi3, Aruna Jawaharlal Bhandari4, Geetanjali Deepak Vikhe5
1 Senior Lecturer, Department of Prosthodontics, Rural Dental College and Hospital, Pravara Medical Trust, Loni, Maharashtra, India.
2 Reader, Department of Prosthodontics, Rural Dental College and Hospital, Pravara Medical Trust, Loni, Maharashtra, India.
3 Professor and Head, Department of Prosthodontics, Rural Dental College and Hospital, Pravara Medical Trust, Loni, Maharashtra, India.
4 Professor, Department of Prosthodontics, Rural Dental College and Hospital, Pravara Medical Trust, Loni, Maharashtra, India.
5 Dental Surgeon, Department of Prosthodontics, Rural Dental College and Hospital, Pravara Medical Trust, Loni, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepak Machindra Vikhe, Senior Lecturer, Department of Prosthodontics, Rural Dental College and Hospital, Pravara Medical Trust, Loni-413736, Maharashtra, India.
E-mail: drdeepak_mvikhe@yahoo.com
Oroantral opening, Retention, Semi-precision attachments
A 43-year-old male patient reported with a chief complaint of difficulty in speaking and chewing food, flow of nasal secretions in right side of oral cavity and facial deformity since four years. The patient had a history of cyst and fungal infection in molar region of maxilla on right side followed by surgical correction of the lesion, four years ago.
Extra-oral examination revealed asymmetry of the face of the patient due to removal of teeth and some part of residual alveolar ridge on the defect side. Intra-oral examination revealed, partially edentulous maxillary arch with few teeth remaining on the left side, the second premolar was rotated mesially. There was an oro-antral opening seen on right side due to unilateral resection during surgical correction. Some part of the hard palate and adjacent mucosa was intact. The lower arch was completely dentulous [Table/Fig-1a,1b]. The patient was informed about different treatment options like conventional removable partial denture with obturator, flexible partial denture with obturator, cast partial denture with attachments, implant supported prosthesis etc., depending on the intra-oral condition. After interaction with patient, a suitable treatment plan was selected depending upon patient’s economic status.

Intra-oral occlusal view of the maxillary arch.

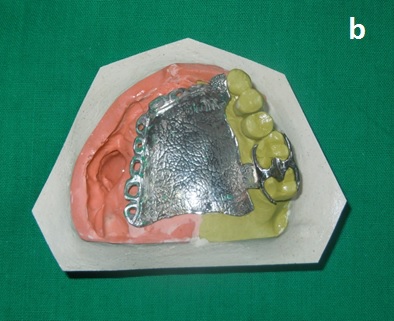
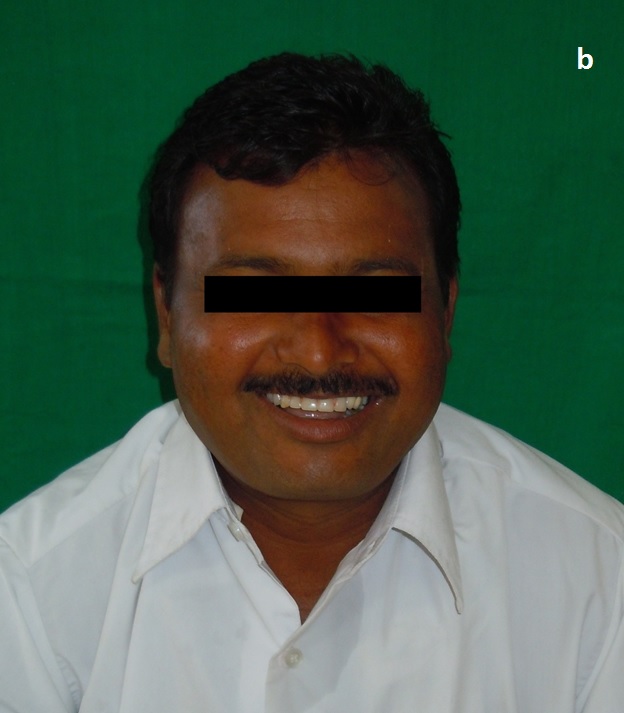
Considering number of abutments, available hard palate, oro-antral fistula and after proper examination and investigations the prosthesis was planned which consisted of cast partial denture with cekapreci-sagix extra coronal attachment and obturator. After proper preprosthetic procedures, the diagnostic impressions were made with irreversible hydrocolloid impression material (DPI) and casts were fabricated. Tooth preparation was done in relation to 25 for correction of rotation. Tooth preparation was also done for teeth 23 and 24 to incorporate the castable plastic male part of cekapreci-sagix extra coronal attachment with the paralleling mandrel into the wax-up of copings for crowns of 23,24 [Table/Fig-2]. Final Porcelain Fused to Metal (PFM) crowns were fabricated on master cast with casted male part of cekapreci-sagix extra coronal attachment. Trail of these crowns was done intra-orally for proper fitting and parallelism of the male part of cekapreci-sagix attachment [Table/Fig-3]. Pick up impression was made with these PFM crowns with casted male part. Final cast were obtained with PFM crowns, attached with male and female processing clip [Table/Fig-4]. The cast was surveyed and planned for cast metal frame work to support the obturator. Proper designing of frame work was done and mouth preparation for cast partial frame work was done, followed by impression. Cast was poured and final casted framework of cast partial denture was obtained and trail done intra orally [Table/Fig-5a,5b]. Final and pick up impression was made with this cast metal frame work [Table/Fig-6]. Cast was poured using altered cast technique [Table/Fig-7a,7b] for proper extension. PFM crowns were cemented on prepared teeth intra-orally with permanent luting cement (GC Fuji GIC Type 1 Luting Cement). Wax rim was fabricated on this frame work, face bow record was made [Table/Fig-8] and transferred on the articulator (whip-mix articulator and face bow), followed by jaw relation recording and mounting of cast. Teeth arrangement and try-in of prosthesis was done for proper occlusion and esthetics [Table/Fig-9a,9b]. After proper verification of trial denture, final acrylization was done and final prosthesis was retrieved incorporated with final female retentive clip of cekapreci-sagix attachment [Table/Fig-10]. As patient was having some stains on lower natural dentition, artificial stains was used on acrylic teeth of prosthesis to camouflage intra-orally [Table/Fig-11a,11b]. The final prosthesis was evaluated for proper extension, fit, phonetics, esthetics, occlusion and function. Pre-operative and post-operative view of patient extra-orally [Table/Fig-12a,12b].
Castable plastic male part of cekapreci-sagix attachment with wax patterns.

PFM crowns with male part.

Female pink processing clip in place.


Cast partial frame work trail intra-orally.

Final and pick up impression.


Frame work on altered cast.

Teeth arrangement on articulator.


Final prosthesis with yellow female retentive clip.

Artifical stains applied on acrylic teeth.

Final prosthesis insertion.

Extraoral pre-operative view.

Extraoral postoperative view.
Discussion
The less retentive prosthesis/obturator is the main problem in acquired maxillary defect patients. The factors which affect the retention of obturator are size of the defect, remaining teeth, remaining bony structure and the ability and time taken by the patient to adapt to the prosthesis [1]. There are various causes for maxillofacial defects such as congenital and acquired. The example of congenital defects is cleft palate and acquired defects are trauma or carcinoma of alveolar bone of maxillary arch including maxillary sinus [2]. Communication can be created between oral cavity and maxillary sinus or nasopharynx by these maxillary defects [3]. The patient’s acceptance and adaptability plays an important role in success of obturator or prosthesis due to less retention. The various ways of increasing retention in prosthesis is by using clasps, soft-liners, different impression techniques etc. These conventional methods have many limitations. These cekapreci-sagix extra-coronal attachments are economical, non-invasive for the patients and on the same time lead to great improvement in retention [1].
The ceka attachment is a prefabricated, resilient attachment [4]. There are two treatment procedures for correction of the maxillary defects, such as surgical procedure or by prosthetic rehabilitation. The surgical treatment demands on more surgical procedure for the patient and it may lead to failure of graft material. The prosthodontic rehabilitation is easy and technically reversible [5]. Cekapreci-sagix attachments are sagittal ball attachments with female retention clip for different prosthetic applications. Male part gets attached with crowns; female parts/clips are placed on tissue side of the denture. To conclude it can be said that, cekapreci-sagix extra coronal attachment helps to maintain balance between esthetic appeal and functional stability in cast partial dentures for the patient.
[1]. Alqutaibi AY, Enhancing retention of maxillary obturators using dental implantsInternational Journal of Contemporary Dental and Medical Reviews 2015 010915:1-5. [Google Scholar]
[2]. Abadi BJ, Byron RJ Jr, Maxillary obturator a clinical case reportEurope PMC 2008 56(7):709-13. [Google Scholar]
[3]. Karthikeyan S, Balu K, Devaki V, Ajay R, A simple method of enhancing retention in interim hollow bulb obturator in a case of an acquired palatal defectJ Pharm Bioallied Sci 2015 7(Suppl 2):S782-85. [Google Scholar]
[4]. Schweikert EO, A prosthetic solution with cantilevered ceka-attachmentsQuintessence Int Dent Dig 1981 12(2):165-72. [Google Scholar]
[5]. Meenakshi A, Shah D, The obturator prostheses for maxillectomySRM J Res Dent Sci 2012 3:193-97. [Google Scholar]