Surgical extraction of impacted mandibular third molar is one of the most commonly performed day care procedure in Oral and Maxillofacial Surgery either for therapeutic or prophylactic purpose. It is often associated with complications like pain, swelling, trismus, dry socket, bleeding and infection, which are typically temporary in nature. However, the most concerning complication is temporary or permanent damage to the Inferior Alveolar Nerve (IAN) resulting in paresthesia, hypoesthesia or dysesthesia of the lower lip, teeth, gingiva and skin over the chin, which significantly affects the quality of life of the patient [1].
Ahmed C et al., reports that the common risk factors for the IAN damage includes advanced age and difficult impaction but the most important one is the proximity of the root to the IAN canal [2]. The incidence of IAN injury following mandibular third molar extraction is 0.41% to 8.1% for temporary altered sensation and 0.014% to 3.6% for permanent nerve damage [3]. But the incidence increases up to 20% to 36% in high risk cases as defined by radiographic signs described by various authors [4,5] which includes alteration in the root structure (darkening, narrowing, root deflection, bifid apex or overlapping over the nerve canal) or alteration in the inferior alveolar canal features (obliteration of radio opaque line, deflection or narrowing of the inferior alveolar canal). In these cases the nerve injury may occur either due to the instrumentation or due to crushing and tearing of the nerve by the root during tooth elevation [4].
Various approaches have been proposed to decrease damage to the IAN in high risk cases, which comprises coronectomy and leaving the roots behind, staged surgical removal of the third molar [6], modified coronectomy and grafting [7], orthodontic aided extrusion [8] and pericoronal ostectomy [9]. Staged tooth removal was proposed to minimize the late post-operative risk of infection of retained roots, but requires two surgical interventions and the amount of root migration is unpredictable. Modified coronectomy with grafting was advocated for restoring the periodontal health of the second molar. Orthodontic aided extrusion of the third molar is technique sensitive, time consuming, expensive and unpredictable procedure. Applied coronectomy to prevent IAN damage was first proposed by Ecuyer and Debien [10] in 1984. In spite of numerous studies supporting the effectiveness of coronectomy, the procedure remains controversial due to the possibilities of infection and other odontogenic pathology arising from the roots left behind [11]. The aim of present study was to evaluate the outcome after coronectomy of mandibular third molars in terms of complications encountered during or after the procedure, temporary or permanent IAN injury, infection rate and other associated morbidity.
Materials and Methods
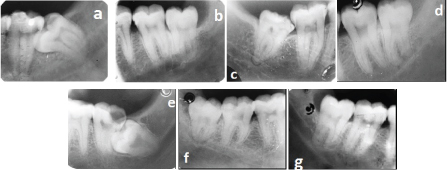
This prospective clinical study was conducted in the Department of Oral and Maxillofacial Surgery, Ragas Dental College and Hospital, Chennai, India, from June 2012 to Jan 2016. The study group consisted of 20 impacted mandibular third molar teeth in total of 18 patients. Individuals visiting our department for impacted mandibular third molar teeth removal were carefully examined. Patients with high risk of injury to IAN [Table/Fig-1a-g] based on Rood’s Criteria [5] in an IOPA, between the age group of 18 to 40 years with the ability to understand and cooperate were included in the study. Patients with local pathology like dental caries or periodontal pathology, nerve canal and roots separated cases, preexisting IAN paresthesia or patients with compromised systemic conditions that will predispose to local infection like uncontrolled diabetes mellitus, HIV infected individuals, chemotherapy, bisphosphonate therapy or previous radiotherapy of head and neck were excluded from the study. Patients, who opted for coronectomy, were described about the procedure and the risk of post-operative complications like pain, root migration, need for second surgery, infection and failure of coronectomy. The possibility of IAN damage and all possible treatment options available to reduce the nerve injury were explained to the patient and informed consent was obtained from the patient prior to the procedure. The Institutional Review Board approved the study. Computed Tomography (CT) scan was not taken in our cases as ethical committee restricts its usage.
Rood’s criteria. a. Darkening of the root. b. Deflection of the root. c. Narrowing of the root. d. Dark and bifid apex of the root. e. Interruption of white line of canal. f. Diversion of the canal. g. Narrowing of the canal.
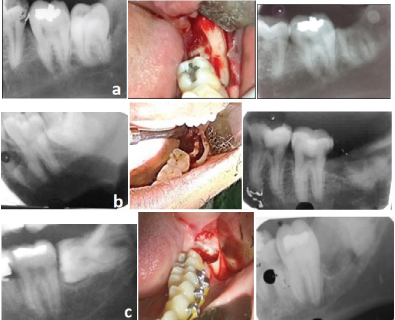
Surgical procedure: Patients were evaluated by standard clinical and radiographic examination. Then the tooth status (eruption status, pattern and depth of impaction, root shape and radiographic signs), Pederson Difficulty Index and Winter’s Classification [12] of impacted mandibular third molar was recorded [Table/Fig-2]. Lignocaine (2%) with 1:80,000 adrenaline was administered to block the IAN nerve and long buccal nerve. Standard Ward’s incision was made with anterior releasing incision mesial to the third molar and distal releasing incision along the anterior border of ramus. Triangular buccal flap was elevated and retracted. The lingual flap was carefully reflected and protected with Howart’s periosteal elevator. Conservative buccal trough was made with 702 surgical bur allowing access to the cemento enamel junction of the tooth. Care was exercised to maintain as much crestal bone height as possible by minimizing the width of the buccal trough. The crown was sectioned transversely at an angle of 45 degree at the level of the cemento enamel junction into crown and root. The crown was carefully fractured while stabilizing the root fragments with an instrument to avoid inadvertent mobilization of the root. Following removal of the crown, a round bur was used to reduce the remaining root fragments so that the remaining roots are at least 2mm-3mm below the crest of the lingual and buccal plates in all places [Table/Fig-3a-c]. During the procedure, if the roots got luxated or inadvertently removed, it was considered a failed coronectomy. Patients were prescribed Amoxycillin 500mg, Metronidazole 400mg and Paracetamol 500mg each three times a day for three days following the procedure.
| S. No. | Pederson Difficulty Index [12] | Eruption Status | Nerve Relationship Radiographic Signs | Winter’s Classification[12] |
|---|
| Partially Erupted | Non Erupted |
|---|
| 1 | 5 | Yes | | Darkening of root | Mesioangular |
| 2 | 8 | | Yes | Deflection of root | Vertical |
| 3 | 8 | Yes | | Darkening of root | Vertical |
| 4 | 6 | Yes | | Dark and bifid apex | Mesioangular |
| 5 | 8 | | Yes | | Vertical |
| 6 | 5 | Yes | | Interruption of white line | Mesioangular |
| 7 | 8 | | Yes | Interruption of white line | Horizontal |
| 8 | 7 | Yes | | Diversion of the canal | Mesioangular |
| 9 | 8 | | Yes | Narrowing of the canal | Vertical |
| 10 | 5 | Yes | | Interruption of white line | Mesioangular |
| 11 | 5 | Yes | | Deflection of root | Mesioangular |
| 12 | 8 | Yes | | Dark and bifid apex | Vertical |
| 13 | 8 | Yes | | Interruption of white line | Horizontal |
| 14 | 5 | Yes | | Darkening of root | Mesioangular |
| 15 | 8 | | Yes | Defelction of the canal | Horizontal |
| 16 | 7 | Yes | | Interruption of white line | Horizontal |
| 17 | 8 | Yes | | Diversion of canal | Horizontal |
| 18 | 5 | Yes | | Deflection of root | Mesioangular |
| 19 | 5 | Yes | | Narrowing of canal | Mesioangular |
| 20 | 5 | Yes | | Interruption of white line | Mesioangular |
Coronectomy photographs.
a. Vertical impaction
b. Mesio angular impaction
c. Horizontal impaction
After the procedure, the patients were evaluated at six months interval for a period of two years for IAN deficit, lingual nerve deficit, pain, dry socket, infection or other complications if anything were noted. If the roots required extraction due to infection or exposure at a later date, it was recorded as complications of coronectomy. IAN deficit was recorded with standardized neurosensory test which included a light touch test, two point discrimination and pain threshold test and were compared with preoperative neurosensory baseline. The distance between the root apex and IAN canal, as well as the distance between the sectioned third molar crown and the second molar were measured on a standardized intra oral radiograph to assess the root migration. To secure an identical position of the film, a bite index and a film holder was used.
Pain assessed with a Visual Analog Scale (VAS) of 1 to 10. Preoperative facial measurements were taken by marking the mandibular angle as base point and the soft tissue pogonion, corner of lip commissure, ala base of nose, lateral canthus of eye and tragus of ear as reference points. The sum of all the measurements were taken to assess the facial swelling and recorded in millimetre preoperatively and one week post-operatively. For statistical analysis, all the data were incrementally entered during the course of study in Microsoft Office Excel Worksheet and ‘paired t-test’ was used to analyze the data.
Results
A total of 18 patients (13 male and 5 female aged between 18 and 40 years) who needed removal of 20 lower third molars (five horizontal impaction, five vertical impaction, ten mesioangular impaction), whose root apices were involved with the inferior alveolar canal were included in the study. The mean age of the patient was 27.6 years. The mean Pederson Difficult Index was 6.6 + 1.4. Coronectomy was successfully performed on 18 third molars and two patients had failed coronectomy and the mobilized roots were removed. Both failed coronectomy cases were female patients with conical root morphology. In all cases healing of the surgical site was uneventful. All patients completed a minimum of two years follow up.
The mean pre-operative facial measurement was 470.7 + 29.9mm and the post-operative swelling at one week was 484.1 + 26mm [Table/Fig-4]. One patient had pain on the soft tissue around the coronectomy site with discomfort in mouth opening for a period of two months which was attributed to enamel lipping left behind intra operatively and it subsided spontaneously. One patient had profuse bleeding intra-operatively in failed coronectomy case, which may be due to the possible manipulation of the inferior alveolar canal. The bleeding was controlled by pressure application and placement of oxidized cellulose. One patient had post-operative numbness in the lateral border of tongue which resolved after a month. Of the 18 asymptomatic teeth, radiographic assessment showed coronectomy was adequate in 15 cases, but a shard of enamel (enamel lipping) had been retained on root fragment in three patients [Table/Fig-5].
Post operative variables.
| S.No. | Pain(1st week) | Swelling | Inferior Alveolar Nerve/Lower Lip Paresthesia | Complications (Infection/ Second Surgical Intervention/ Others) |
|---|
| Pre-operative | (1st week) | 1st week | 6 months |
|---|
| 1 | 0 | 443 | 465 | No | No | Nil |
| 2 | 0 | 429 | 430 | No | No | Nil |
| 3 | 1 | 487 | 495 | No | No | Failed coronectomy |
| 4 | 0 | 483 | 480 | No | No | Nil |
| 5 | 1 | 460 | 460 | No | No | Nil |
| 6 | 0 | 490 | 490 | No | No | Temporary numbness on lateral border of tongue |
| 7 | 0 | 453 | 460 | No | No | Nil |
| 8 | 0 | 464 | 493 | No | No | Failed coronectomy, post operative bleeding |
| 9 | 0 | 415 | 440 | No | No | Nil |
| 10 | 0 | 510 | 535 | No | No | Nil |
| 11 | 0 | 445 | 450 | No | No | Nil |
| 12 | 0 | 514 | 520 | No | No | Nil |
| 13 | 0 | 499 | 490 | No | No | Nil |
| 14 | 0 | 490 | 490 | No | No | Nil |
| 15 | 3 | 493 | 495 | No | No | Post operative pain |
| 16 | 0 | 505 | 496 | No | No | Nil |
| 17 | 0 | 480 | 497 | No | No | Nil |
| 18 | 0 | 483 | 498 | No | No | Nil |
| 19 | 0 | 420 | 499 | No | No | Nil |
| 20 | 0 | 450 | 500 | No | No | Nil |

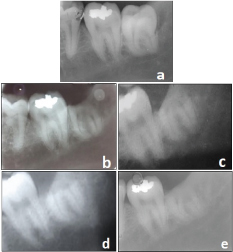
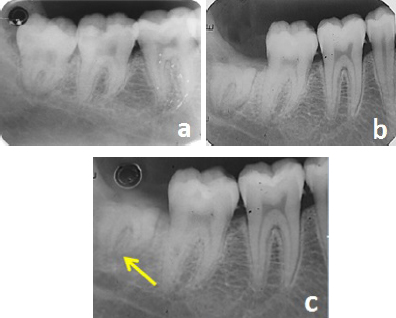
Bone formation [Table/Fig-6] around the retained roots were observed in 14 of our cases and root migration [Table/Fig-7] of approximate 1mm-2mm away from the nerve was observed in five of our cases at two year follow-up. None of our patients required second surgery and none developed permanent nerve injury either to IAN or lingual nerve.
Formation after coronectomy.
a. Pre-operative, b. Immediate post-operative, c. Six months post-operative
d. One year post-operative, e. Two year post-operative.
Root migration after coronectomy.
a. Pre-operative b. Immediately after coronectomy c. Six months after coronectomy.
Discussion
The majority of nerve injuries in the oral surgery involve branches of the trigeminal nerve. The nerve injuries can be produced by pathological conditions, traumatic injury, surgical access, orthognathic surgery, dental implantology surgery or occasionally following local anesthetic administration. In all the aetiology of nerve injuries, the extraction of third molar was the cause of nerve damage in 52.1% of oral surgical cases [13]. Fieldman has reported the incidence nerve injury following third molar impaction surgery as “silent epidemic of iatrogenic trigeminal nerve injury” [14].
Mandibular third molars are frequently removed prophylactically to prevent the potential pathological complications associated with the tooth. However, since the newly published recommendations of British National Institute of Clinical Excellence (NICE), regular prophylactic extraction of impacted third molars has reduced in United Kingdom. The guideline given by NICE specifically opposes prophylactic removal of mandibular third molars and listed specific clinical indications for the surgery [14,15]. Initially, this guideline was also followed in USA with conservative approaches to third molar management, but now it has been accepted that prophylactic removal is a standard procedure and is no longer a controversial treatment option as presented in the Third Molar Multidisciplinary Conference in American Association of Oral and Maxillofacial Surgeons (AAOMS) ParCare 2012 [16,17].
The first dictum of Medicine and Surgery is – ‘Primum Non Curaram’ means – First Do No Harm. Neurosensory damage is the commonest cause of litigation following impacted third molar surgery [18]. Lydiatt claims that the patients often forget the information given to them prior to the procedure and only 30% to 50% of the information given to them was recalled after seven days of the surgery and stresses the significance of informed consent [19]. Pogrel MA has reported that only 20% of cases had good improvement, 30% had moderate improvement and the remaining 50% had no improvement in sensation following micro neurosurgery [20]. Therefore, prevention is better than cure to prevent patient dissatisfaction following the procedure. Conservative and minimally invasive procedure that is required for the management of disease is always the preferred treatment [17].
Most pathological conditions arising from the third molar are related to the crown and peri-follicular structures. The follicle acts as deep periodontal pocket which is the frequent site for infection. It gives rise to pericoronitis, periodontal problems, decayed tooth and follicle related odontogenic cysts and tumours. Thus, the crown along with the follicular tissue should be removed to relieve from any further infections [21]. Coronectomy or Prejudiced Odontectomy (American Dental Association-D7251) is a technique by means of which the crown is sectioned and the roots that are closer to the IAN canal on diagnostic radiographic imaging are left in situ [4]. Retention of root for coronectomy is based on the idea that broken fragments of vital teeth generally heal without complications [22,23]. This procedure attracted special attention in the last decade, because of the reported benefits and success rate of this technique, in contrast to the contemporary belief that the roots left behind will be the source of problem [6,24,25].
The radiological appearance of the tooth root and the IAN were compared to whether or not the nerve was visible in the socket at the time of operation, produced predictor signs for possible damage to the nerve which, if present, the incidence of labial nerve impairment was recorded as 35.64% [4]. A comparative study showed radiological signs to actual incidence of damage to the IAN and found that three radiological signs (darkening of the root, interruption of lamina dura, and diversion of the canal) posed statistically significant as predictors of trauma to the IAN and stated when one of those signs if present, the nerve was affected in 30% cases [5]. Along with these signs, other factors includes the severe angulation of the root apices at the canal, hypercementosis of the root or root apex and any forceful manipulation with the bur or other instruments near the nerve would cause damage eventually [21].
Dental Computerized Tomography (CT) would be very helpful and would probably be the best choice for evaluating the relationship of the IAN and impacted tooth. But it is also more expensive, higher radiation exposure and not easily accessible to many patients. Khan et al., compared the panoramic signs (root darkening, channel narrowing, radiolucency between root and channel, cortical channel interruption, channel diversion) with CT findings and found 30% to 50% correlation [26]. In our study, we preferred to assess lower third molars with Intra-Oral Peri-Apical (IOPA) radiograph, viewed it with the help of magnifying glass when necessary and then made decision for a coronectomy.
Landi L et al., recommends coronectomy to be done, 2mm-3mm from the occlusal surface without involving the pulp after considering the pulpal anatomy of the impacted third molar tooth and the distance between the third molar crown and the second molar [6]. In case of accidental pulpal exposure pulpal dressing or pulpotomy was advised. In our study, we sectioned the crown at the cemento enamel junction level and the remaining enamel if anything is grinded off to the level 2-3 mm below the alveolar crest. It was described that enamel is inert and soft tissue cannot attach to its surface so the socket does not heal [27]. The enamel acts as foreign body, so chances of infection of the unhealed socket is more. Root fragment at least 3 mm inferior to the crest of bone seems appropriate and appears to encourage bone formation over the retained root fragment [28–30]. Our objective was to leave the root behind and aim for osseo-cementum formation over the retained root in contrast to migration and staged removal protocol of Landi L et al., [6]. We didn’t attempt to treat the exposed pulp as advocated by O’Riordan et al., [21], as coronectomy decompresses the pulp chamber, it will not be a significant contributing factor for post-operative pain. Histological evaluation of the retrieved lower third molar roots stated that symptoms after coronectomy do not result from the loss of pulp vitality or subsequent periradicular inflammation. It was refined that these pulpal tissues blend with overlying connective tissue when the mucosa heals successfully and the opening of the canal heals with osteo-cementum [27]. Interestingly, it was described that pulpal treatment of the retained root has resulted in high rate of infection and the subsequent need for removal [31].
Female patients with conical roots have higher risk for failure of coronectomy [32]. Incidence of nerve injury was greater in female patients, possibly because the bucco-lingual cortical bone is thinner, making the apical area of the mandibular third molar closer to the IAN. In our study, also both the failed coronectomy cases had fused and short roots which got luxated during sectioning the crown. None of our cases had infection or required second surgery post operatively. The radiolucent zone after third molar root migration may be mistaken for infection which should be carefully evaluated with the immediate post coronectomy radiograph [27]. None of our cases had IAN paresthesia which correlates with other studies.
Although some authors used preoperative prophylactic antibiotic therapy [33], we did not prescribe any preoperative antibiotics and did not encounter any infections in our study. We prescribed routine post-operative antibiotics after the procedure. Lingual flap protection was considered in our study as described in the literature [33], where it mentions that lingual retraction is essential to prevent inadvertent lingual bone plate perforation, thereby preventing permanent lingual nerve injury. Retraction of a lingual mucoperiosteal flap is frequently associated with an increased frequency of temporary lingual nerve damage and many authors contradict the lingual flap retraction procedure [34–37]. We had a case of temporary numbness of the lingual vestibule and lateral tongue which probably resulted from lingual flap maneuvering. None of our cases had IAN neurosensory complication including in the failed coronectomy patients.
Many authors are not advocating coronectomy procedure for the horizontally impacted third molar because of the difficulty in conceptualizing the third molar three dimensionally during sectioning and for the potential risk to IAN injury during sectioning the crown [38–40]. In contrary to this concept, the crown was sectioned bit by bit as advocated by Clare et al., [41]. Philips et al., claims that 26% to 35% of unerupted third molars retain eruption potential and change their position over time, depending on the angle of impaction and migrate towards occlusal plane [42]. Migration of root has been noted in every article published on this subject and appears to occur in between 14% to 81%, depending on the length of the follow-up [32,43]. A literature revealed that more than half of the roots migrated at a higher rate for 3 months post-operatively and then gradually stopped between 12 and 24 months [44]. We had a migration of root of about 1mm-3mm during a period of two years.
Many coronectomy studies reported incidence of 10%-12% of alveolar osteitis [3,32,45]. There was report where they mentioned that the occurrence of dry socket was considerably low in coronectomy in comparison to removal of third molars, because there is reduction in the amount of bone exposed and stabilizing effect with primary closure for all coronectomy cases, eventually resulted in no loss of clots [46]. Incidence of dry socket was not evident in our case series.
In this study, the coronectomy procedures were done by a single operator. Similar to training in impacted mandibular tooth removal, coronectomy also requires surgical training which is one of the frequent causes of failed coronectomy cases when multiple operators are involved. In this study we included all impacted third molar cases irrespective of the angulation of the third molar as we were evaluating the osseo-cementum formation over the root rather than root migration.
Limitation
The major drawback of this study is the smaller sample size. In spite of the reported advantages of the coronectomy, patients are very anxious about leaving the root behind in the bone and are not willing to take a chance for infection or a second surgical intervention. The study should be done with larger sample size with control group using computed tomography in high risk cases to extrapolate the results obtained from this study to a larger population. The periodontal health of second molar and the quality of bone distal to the second molar should also be evaluated in future studies to assess the requirement of growth factors or bone grafting during coronectomy procedure.
Conclusion
Coronectomy significantly reduces inferior alveolar nerve injury even in high risk cases, with reduced morbidity and other associated complications in contrast to conventional technique. However, potential complications of coronectomy like periodontal pockets on the distal surface of the second molar, root migration with possible need of a second procedure, dry sockets, local post-operative infections, post-operative pain, inadvertent root removal or root walk-out intra-operatively and inferior alveolar or lingual nerve damage should be discussed with the patient before recommending the procedure.