Adrenal Schwannoma: A Rare Incidentaloma
Sumit Kumar1, Vilvapathy S. Karthikeyan2, Chikkamoga S. Manohar3, K. Sreelakshmi4, Maregowda Shivalingaiah5
1 Senior Resident, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
2 Senior Resident, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
3 Assistant Professor, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
4 Assistant Professor, Department of Pathology, Victoria Hosptial, Bangalore, Karnataka, India.
5 Professor, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vilvapathy S. Karthikeyan, 35, Second Cross, Thirumal Nagar, Pondicherry-605013, Karnataka, India.
E-mail: sengkarthik@yahoo.co.in
Adrenal schwannomas are very rare tumours that are difficult to diagnose preoperatively. A 42-year-old male presented with epigastric pain and indigestion. He had history of repeated operations for recurrent facial swelling on both sides of face diagnosed as Angiolymphoid Hyperplasia with Eosinophilia (ALHE). Physical examination revealed right facial swelling. Laboratory tests showed no evidence of hormonal hypersecretion. CECT abdomen showed a well-defined heterogenously enhancing right adrenal mass (5x4cm). Patient underwent right adrenalectomy. Histopathology revealed adrenal schwannoma, confirmed by immunohistochemistry (IHC) showing diffuse expression of S-100. Fine-needle aspiration biopsy of facial lesion confirmed ALHE recurrence. Less than 35 cases have been reported. Diagnosis of adrenal schwannoma on imaging studies is very difficult and surgical resection when performed for non-functioning adrenal masses >4cm clinches the diagnosis. Adrenal schwannoma is highly uncommon and was incidentally associated with recurrent ALHE.
Adrenalectomy, Angiolymphoid Hyperplasia with Eosinophilia (ALHE), Nodular swellings
Case Report
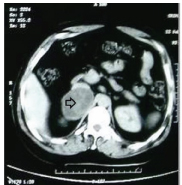
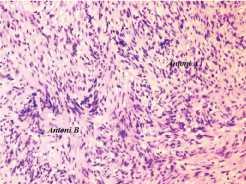
A 42-year-old male presented with epigastric pain and indigestion since 2 months. His medical history revealed that he had undergone multiple operations for recurrent facial swellings and histopathology had revealed Angio-Lymphoid Hyperplasia with Eosinophilia (ALHE). Physical examination revealed multiple preauricular and postauricular nodular swellings [Table/Fig-1]. There were no similar swellings elsewhere. Complete blood count, renal and liver function tests were unremarkable. Ultrasound abdomen showed a well-defined mixed echogenic right suprarenal mass (6.4x4.5 cm). CECT abdomen detected a well- defined heterogenously enhancing right adrenal mass measuring 5x4 cm [Table/Fig-2]. Hormonal evaluation in the form of fasting plasma cortisol, plasma aldosterone concentration, plasma renin concentration and 24 hour urine for metanephrines was negative, ruling out adrenal hormonal hypersecretion. Fine-needle aspiration biopsy of facial lesion confirmed recurrence of ALHE. With this background, an adrenal incidentaloma was diagnosed and patient underwent right open adrenalectomyas it was non-functioning and measured 5cm on CECT abdomen. On gross pathological examination, a globular cystic mass 8x7x3.5 cm weighing 100 grams with smooth capsule was found [Table/Fig-3]. Cut-section showed variegated appearance with predominantly solid areas with cystic and haemorrhagic components [Table/Fig-4]. Histopathologic examination revealed spindle shaped cells arranged in hypercellular and hypocellular areas. Cells in hypercellular areas had pallisading arranagement with Verocay body formation [Table/Fig-5]. On immunohistochemistry, spindle cells were strongly and diffusely S-100 positive, confirming adrenal schwannoma [Table/Fig-6]. Postoperative follow-up at 18 months remains uneventful with no recurrence on ultrasound abdomen.
Clinical photograph showing multiple preauricular and postauricular nodular swellings. (arrow)

CECT abdomen showing a well-defined heterogeneously enhancing right adrenal mass (arrow) measuring 5x4cm.
Gross appearance of adrenal schwannoma showing globular cystic mass measuring 8x7x3.5cm.
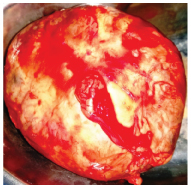
Cut-section of adrenal schwannoma - variegated appearance where solid areas are predominantly yellowish with cystic and haemorrhagic areas.

Photomicrograph: Spindle shaped cells arranged in hyper and hypocellular areas. Cells in hypercellular areas show pallisading arranagement with Verocay body formation. H&E, 100X.
Immunohistochemistry: Spindle cells are strongly and diffusely S100 positive. 40X.

Discussion
Adrenal Schwannoma (AS) is a rare incidentaloma found in the adrenal medulla and only less than 35 cases have been reported till date [1–4]. It is difficult to diagnose AS preoperatively by imaging alone and surgical resection is the primary management. Schwannomas are encapsulated, usually benign slow-growing nerve sheath tumours, containing schwann cells in the stroma with minimal collagen [1]. These usually occur in head, neck, flexor surfaces of upper and lower extremities. Retroperitoneum accounts for 1-3% of schwannomas [2]. Visceral schwannomas especially in adrenal gland occur rarely and are discovered serendipitously. AS is usually discovered as a non-secreting adrenal mass in asymptomatic patients. Some patients may present with minor clinical symptoms like abdominal pain, back pain or haematuria. Adrenal incidentaloma include cortical lesions like adenoma and carcinoma and medullary lesions like pheochromocytoma, neuroblastoma and ganglioneuroma [3].
Mohiuddin et al., reviewed 33 reported cases [3]. The cases demonstrated a broad age range, from 14 to 89 years, with a median age of 49 years with a slight female predominance (F:M=1.2:1). In this series, majority of the adrenal schwannomas were identified incidentally and only 13 out of 30 patients had abdominal pain, flank pain or discomfort before specific diagnosis. Though most of the cases had no clinical or biochemical evidence of endocrine hormonal activity, one case showed elevated urinary catecholamines.
Patients with adrenal tumours require a complete endourologic assessment including measurement of serum electrolytes, serum catecholamines, 24-hour urine studies for catecholamines, metanephrines, vanillylmandellic acid and 17-ketosteroids. CT scan also aids in diagnosis. Schwannomas appear as well-circumscribed, homogenous, round or oval mass, with slight enhancement on CT scan [5]. Cystic degeneration or calcification, if present, is suggestive of long-standing schwannomas, but pheochromocytomas and malignancies should be kept in mind in a large tumour [3]. Preoperative diagnosis is not definitive and histopathologic examination is required in most cases to confirm the diagnosis [6]. Functioning adrenal lesions and nonfunctioning adrenal lesions greater than 6cm should be excised, those less than 4 cm with imaging characteristics that appear benign should generally not be resected, and those between 4cm and 6cm can be either closely observed or resected [3].
On gross examination, AS appear firm, round, well-circumscribed tan-yellow to grayish-white tumours. Though mostly solid with homogenous consistency, some larger ones present with cystic areas, calcification or haemorrhage. On histopathologic examination, AS may be conventional or cellular [3]. Conventionally, schwannomas present as alternating compact areas termed Antoni A and loosely textured paucicellular areas described as Antoni B. Nuclear-free zones seen between nuclear palisading are known as Vercoay bodies [1]. Immunohistochemistry of adrenal schwannomas with S-100 protein showing strong and diffuse staining confirms diagnosis. AS shows positivity for vimentin. They also reveal pericellular reactivity for type 4 collagen [7]. They stain negative for CD117, desmin, CD34, HMB45, synaptophysin, cytokeratin and smooth muscle actin on immunohistochemistry [3].
Follow-up is done with USG or CT scan over regular intervals. Prognosis in most cases after resection has been found to be favorable. ALHE is an uncommon benign vascular neoplasm presenting with small, dull red papules or nodules usually 2–3 cm in diameter. It is mainly found on the head and neck, mostly in the vicinity of the ear. It can also involve trunk, extremities, genitalia, lips and oral mucosa. It was first described in 1969 by Wells and Whimster [8]. ALHE can arise either due to a benign neoplastic proliferation of vascular tissue or a reactive hyperplasia of vascular tissue due to trauma, infections, renin or hyperestrogenic states (pregnancy or oral contraceptives) [8,9].
There is involvement of dermis and/or the subcutaneous tissue. ALHE on histopathology shows benign proliferation of dilated small to medium-sized blood vessels mixed with a nodular, perivascular, inflammatory infiltrate composed of predominantly polytypic B lymphocytes, eosinophils, histiocytes, plasma cells, neutrophils and mast cells [8]. Surgical excision is treatment of choice, but local recurrences do occur in 33-50% after standard surgical excision [4].
Conclusion
Preoperative diagnosis of adrenal schwannoma is difficult. Surgical excision provides ultimate tissue diagnosis because of non-availability of reliable and definite non-histological diagnostic modalities for this rare tumour. Diagnosis can be confirmed by histological and immunohistological evaluation. Till now no relation has been found between these adrenal schwannoma and recurrent Angiolymphoid Hyperplasia and Eosinophilia (ALHE), but this case raises an interesting possibility of their association.
[1]. Woodruff JM KH, Louis DN, Scheithauer BW, Schwannoma 2000 Lyon FranceIARC Press [Google Scholar]
[2]. Târcoveanu E, Dimofte G, Bradea C, Moldovanu R, Vasilescu A, Anton R, Adrenal schwannomaJSLS 2009 13(1):116-19. [Google Scholar]
[3]. Mohiuddin Y, Gilliland MGF, Adrenal schwannoma: a rare type of adrenal incidentalomaArch Pathol Lab Med 2013 137(7):1009-14. [Google Scholar]
[4]. Jeshtadi A, Govada N, Somalwar SB, Nagulapally S, Schwannoma of the adrenal glandJ Med Allied Sci 2014 4:77-80. [Google Scholar]
[5]. Suzuki K, Nakanishi A, Kurosaki Y, Nogaki J, Takaba E, Adrenal schwannoma: CT and MRI findingsRadiat Med 2007 25(6):299-302. [Google Scholar]
[6]. Weiss SW GJ, Enzinger and Weiss’s Soft Tissue Tumours 2001 St Louis, MOMosby [Google Scholar]
[7]. Fine SW, McClain SA, Li M, Immunohistochemical staining for calretinin is useful for differentiating schwannomas from neurofibromasAm J Clin Pathol 2004 122(4):552-59. [Google Scholar]
[8]. Kaur T, Sandhu K, Gupta S, Kanwar AJ, Kumar B, Treatment of angiolymphoid hyperplasia with eosinophilia with the carbon dioxide laserJ Dermatolog Treat 2004 15(5):328-30. [Google Scholar]
[9]. Miller CJ, Ioffreda MD, Ammirati CT, Mohs micrographic surgery for angiolymphoid hyperplasia with eosinophiliaDermatol Surg 2004 30(8):1169-73. [Google Scholar]