The word esthetics derived from the Greek word ‘Perception’, has become an inseparable part of modern dentistry or cosmetic dentistry. The most common defect tainting the beauty of the mouth and thus, the face, is discoloured teeth. This can be caused by various natural or iatrogenic causes or can be habit related. Several methods are available for treating discolored teeth such as - laminates, veneers, jacket crowns, microabrasion, macroabrasion and bleaching [1].
Even with so many newer contemporaries, bleaching still continues to hold its century old place as being simple, common, least invasive, economical, most effective and patient friendly treatment modality for removing or diminishing stains [1].
Hydrogen peroxide and carbamide peroxide are the two commonly used bleaching agents. Hydrogen peroxide dissociates into molecular oxygen and water and this molecular oxygen oxidises the stains and thus bleaches it. Peroxide due to its low molecular weight and protein denaturation ability can enter the pulp through enamel and dentin and cause reactions of pulp ranging from mild transient pulpal inflammation to suppression of the pulpal enzymes, engorgement of pulpal blood vessels and irreversible pulpal changes [2].
The application of bleaching agent can lead to changes in the properties of the restorative material and could affect its adhesion to the tooth. As there is always some degree of microleakage between tooth and restoration it brings forward a possibility that the bleaching agent can penetrate into the pulp and damage it [3].
This study is a part of a previously conducted study where the penetration of 10% carbamide peroxide commonly used “at home” bleach, into the pulp chamber was evaluated [2]. In this study, penetration of 30% hydrogen peroxide commonly used “in office” bleach, into the pulp chamber was evaluated, keeping the methodology used, the type of restorative materials used and the test control agent similar to the previously conducted study [2].
The study was done to evaluate the penetration of 30% hydrogen peroxide into pulp chamber through intact tooth surface and tooth surface that was restored with a hybrid composite resin and Resin Modified Glass Ionomer Cement (RMGIC).
Materials and Methods
This in-vitro study was conducted between June 2014 to November 2014 in the Department of Conservative Dentistry, Kalinga Institute of Dental Sciences, Bhubaneswar and the teeth for the study were collected from the Department of Oral and Maxillofacial Surgery. A total of 60 intact human maxillary central incisors of patients of the age group between 40 to 60 years undergoing extraction for periodontal reasons were selected for the study.
The inclusion criteria were as follows
Teeth with no surface defects, cracks or fracture lines.
Intact teeth extracted for periodontal reasons.
Adult patient of the age group 40 - 60 years.
The exclusion criteria were as follows
Teeth with surface defects, cracks or fracture lines.
Teeth with previous restorations or root canal treatment.
The teeth collected was cleaned with an ultrasonic scaler to remove any debris or calculus and was stored in distilled water till the study was conducted. Distilled water was chosen as the preservative medium so as not to create any bias when the teeth would be subjected to the treatment agents for evaluation of pulpal penetration.
The specimens were divided into six groups comprising of 10 teeth each. In the first two groups (Group 1and 2), the teeth were left intact with no cavity preparation done on them. In the next four groups, standard Class V cavity preparation, 2mm deep, 3mm in length and 1mm coronal to the CEJ was done. Out of these four groups, two groups (Group 3 and 4), were restored with a hybrid composite resin (Filtek Z350) and the other two groups (Group 5 and 6), were restored with a RMGIC (Fuji II LC), 24 hours post polymerization, final finishing and polishing was done with Sof-lex discs (3M ESPE) and teeth were placed in distilled water for 24 hours. These teeth then underwent thermocycling between 5oC and 55oC for 500 cycles to simulate the oral envrionment [2].
The roots were then sliced 3mm apical to the Cemento-Enamel-Junction. A #4 round bur was used to widen the access to the pulp through the cut root, following which pulpal tissue, if present, was removed with a spoon excavator and then the pulp cavity was washed with distilled water [2].
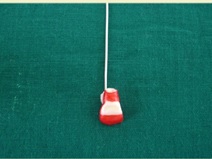
Two layers of nail varnish were used to isolate the teeth to prevent any cross diffusion, leaving a standardized buccal area exposed to the bleaching agent in intact teeth. In case of restored teeth 2mm beyond the restoration margins was isolated. A 21 gauge stainless steel wire was attached to the cut coronal end of the root of each tooth by composite resin [Table/Fig-1]. The wire helped in suspending the teeth in the glass test tube [2]. Group 1, 3 and 5 acted as control in the experiment [2].
Sectioned tooth sample with restoration, nail varnish coat and orthodontic wire attachment.
After drying the pulp chamber 100μl of 2M acetate buffer was placed into it to absorb and stabilize the diffused peroxide. Each tooth was then immersed for 30 minutes in the concerned test solution that was present in the glass test tube in such a way, that the clinical crown was completely immersed in that solution. The test tubes were placed in a water bath whose temperature was maintained at 37oC during this 30 minutes exposure [2].
After 30 minutes, the acetate buffer solution was transferred to a glass test tube. Then, the pulp chamber was rinsed twice with 100μl of distilled water which was then transferred to the same test tube. A 100μl of 0.5 mgml-1 leucocrystal violet and 50μl of 1 mgml-1 enzyme horseradish peroxidase were placed into each test tube and the solution was diluted using distilled water to 3ml [2]. This methodolgy is adopted from the methodology similar to the previously conducted study and as described by Mottola et al., [2,4].
The optical density of the resultant blue colour in the tubes was measured by a U-V spectrophotometer at a wavelength of 596 nm. A standard curve of known amount of hydrogen peroxide was used to convert the optical density values into microgram equivalents of hydrogen peroxide [2].
Statistical Analysis
Descriptive data were presented as Mean, Standard Deviation and Range values and used for analysis; One Way ANOVA was used for multiple group comparisons and Student’s t-test for pairwise comparisons. A p-value of 0.05 or less was considered for statistical significance.
Results
Group 1, in which intact teeth were immersed in distilled water showed no pulpal peroxide level. Group 2, in which intact teeth were immersed in 30% hydrogen peroxide, showed pulpal peroxide level in the range between 21.90μg to 23.16μg with a mean of 22.53μg and a standard deviation of ± 0.55.
Group 3, in which teeth restored with a hybrid composite resin were immersed in distilled water showed no pulpal peroxide level. Group 4, in which teeth restored with a hybrid composite resin were immersed in 30% hydrogen peroxide, showed pulpal peroxide level in the range between 26.56 μg to 28.46 μg with a mean of 27.51 μg and a standard deviation of ± 0.85.
Group 5, in which teeth restored with RMGIC were immersed in distilled water showed no pulpal peroxide level. Group 6, in which teeth restored with a RMGIC were immersed in 30% hydrogen peroxide, showed pulpal peroxide level in the range between 32.22μg to 34.25μg with a mean of 33.25μg and a standard deviation of ± 0.66.
Descriptive information on the penetration of peroxide into the pulp chamber in the groups and related information in terms of mean and standard deviation have been presented in [Table/Fig-2]. ANOVA and Student t-test comparison between groups is presented in [Table/Fig-3].
Descriptive information on penetration of peroxide into the pulp chamber.
| Bleaching Agents | Intact Teeth | Restored |
|---|
| Group No. | Range (μg) | Mean ± SD (μg) | Composite | RMGIC |
|---|
| Group No. | Range (μg) | Mean ± SD (μg) | Group No | Range (μg) | Mean ± SD (μg) |
|---|
| DW | 1 | - | 0.0 | 3 | - | 0.0 | 5 | - | 0.0 |
| 30% H2O2 | 2 | 21.90 – 23.16 | 22.53 ± 0.55 | 4 | 26.56 – 28.46 | 27.51 ± 0.85 | 6 | 32.22 – 34.25 | 33.25 ± 0.66 |
• DW : Distilled water
• 30% H2O2 : 30% Hydrogen peroxide
Inter group comparison (Group 2,4 and 6) of penetration of pulp chamber with 30% H2O2 using ANOVA and intragroup comparison using Student t-test.
| No. | Groups | Penetration (μg) | Difference between Groups |
|---|
| Mean | SD | ANOVA | Groups Compared | Mean Difference (μg) | p-value* | Student t-test |
|---|
| 2. | Intact teeth | 22.53 | 0.55 | F=594.8p <0.001,(HS) | 2 – 4 | 4.98 | p<0.001 | 46.27 |
| 4. | Composite restored | 27.51 | 0.85 | 2 – 6 | 10.72 | p<0.001 | 132.67 |
| 6. | RMGIC restored | 33.25 | 0.66 | 4 – 6 | 6.74 | p<0.001 | 45.60 |
*Significant
The groups in which 30% hydrogen peroxide was applied (Group 2,4 and 6) One way ANOVA was done and a statistically significant difference was seen in the penetration of peroxide into the pulp chamber of intact teeth and teeth restored with hybrid composite resin and RMGIC (p<0.001, F= 594.8). Group 6 (RMGIC) showed the highest penetration and Group 2 (intact teeth) showed the least amount of penetration. Intragroup comparison between Group 2 (intact teeth) and Group 4 (composite resin) gave a statistically significant result (p<0.001, t = 46.27). Similar statistically significant result was obtained on comparison of Group 2 (intact teeth) with Group 6 (RMGIC) (p<0.001, t = 132.67) and Group 4 (composite resin) with Group 6 (RMGIC) (p<0.001, t = 45.60).
Discussion
This study was conducted to evaluate the penetration of 30% hydrogen peroxide into the pulp through intact teeth and teeth restored with composite resin and RMGIC as literature search did not show any study conducted on 30% hydrogen peroxide and its penetration in restored teeth using both composite resin and RMGIC. The methodology used in this study is as described by Mottola et al., and is considered to be most sensitive in detecting the presence of peroxide in the pulp [4]. In this method, hydrogen peroxide using horseradish peroxidase as a catalyst causes oxidation reaction to occur in the acetate buffer solution having leucocrystal violet. This reaction produces a colour validating the presence of peroxide in the pulp [2,4].
The general public today opt for bleaching to have dazzling white teeth that would make them look more younger, healthier and attractive [5]. The basic process of bleaching involves oxidation of the inter-prismatic organic matrix of the enamel and dentin when hydrogen peroxide breaks down to form molecular oxygen and water [5]. Bowles and Ugwuneri and later Cooper et al., have shown that hydrogen peroxide easily passes through the enamel, dentin and into the pulp [6,7]. This free movement is due to the relatively low molecular weight of the peroxide molecules (30g/mol) and may account for transient pulpal sensitivity that is occasionally experienced by some patients [8].
There are varied results pertaining to the effect of hydrogen peroxide on pulp. Bowles and Thompson and Bowles and Burns demonstrated inhibition of pulpal enzymes by peroxide [9,10]. Hoffman and Meneghini showed toxicity of peroxide to cultured human fibroblasts [11]. Hanks and Wataha showed that hydrogen peroxide could diffuse to the pulp and reach a level that is capable of causing harmful biological effects in 15 minutes on fibroblasts [12]. Studies have shown that hydrogen peroxide concentrations as low as 5% can dramatically inhibit pulpal enzyme activity [6,13,14]. Hydrogen peroxide (35%) caused obliteration of odontoblasts, haemorrhage, resorption and inflammatory infiltration in the pulp but these changes in the pulp demonstrated evidence of reversibility after 60 days [15]. Cohen and Chase did not observe any histological proof of pulpal damage after subjecting teeth to 35% hydrogen peroxide in vivo [16]. Robertson and Melfi, Matis et al. and Leonard et al., observed mild sporadic and reversible reactions for in office bleaching techniques [17–19]. The possible mechanism by which pulp protects itself is production of peroxidase and catalase that causes enzymatic breakdown of peroxide and the production of haeme-oxygenase 1 which is a defensive enzyme in oxidative stress [14]. Positive pulpal pressure and osmotic pressure may also hinder the entry of peroxide into the pulp [14].
The most common direct restorative materials to be employed for the anterior teeth include composite resins and glass ionomer cements. A major problem in restorative dentistry despite its advancements is the lack of proper union between the restorative material and the tooth surface thus leading to microleakage [20].
Restorative materials, when placed in the oral environment, are constantly being subjected to challenges of a thermal nature, such challenges if significant, can have unfavorable effects on the margin of restorations thus causing microleakage [21]. In vitro thermocycling simulates these conditions of the oral cavity in the teeth subjected to it and causes aging of the restoration due to the high and low temperature that they are subjected to, which produces different thermal expansion coefficient between tooth and restoration interface [22].
When a bleaching process is applied to a restored tooth the properties of the restorative material may be affected by the bleaching agent. Bleaching alters the bonding characteristics of the restorative materials. Both pre and post operative bleaching is said to decrease the bonding of restorative materials to the tooth and increase the microleakage, this is attributed to the presence of residual peroxide which possibly inhibits the polymerization of the bonding agent resulting in marginal gaps [23]. Studies have suggested that the amount of penetration of peroxide into the pulp is more in restored teeth than in intact teeth [13]. The penetration is largely due to the microleakage properties of restorative materials, as none of the restorative materials are able to completely prevent microleakage. The amount of penetration also depends on the type, depth and size of the restoration, insulating base material and bonding agent used, the application time and concentration of the bleaching agent used [3,13,21]. The higher the concentration of peroxide in the agent more is the penetration into the pulp [14]. This finding is similar to the results of the study conducted. Among the two restorative materials used in the study, the results showed that there was greater penetration of peroxide into the pulp through teeth restored with RMGIC than in teeth restored with a hybrid composite resin which could be due to greater microleakage [3]. The greater microleakage of RMGIC could be due to its dual cure property in which the resin component causes it to shrink during light polymerization and further shrinkage is continued due to its chemical reactions [20,21]. The volumetric changes is markedly more in resin modified glass ionomer [24] and its wetting ability to the tooth structure is less due to less water and carboxylic acid content, thus, exhibiting greater microleakage [21].
Resin composites due to advanced adhesive technology show less microleakage [3]. and when exposed to thermal changes in the mouth, resin composites expand on heating and contract on cooling, whereas resin modified glass ionomers contract on heating (due to loss of water) and undergo further contraction on cooling due to thermal contraction [21]. These facts validate the reason for greater microleakage and more penetration of peroxide into the pulp in teeth restored with RMGIC.
Limitation
This is an experimental study and does not represent the actual in-vivo condition.
Other concentrations of hydrogen peroxide could be assessed.
Other restorative materials could have been used and its penetration could have been assessed.
Conclusion
It can be concluded from this study that there is penetration of hydrogen peroxide from the bleaching agent into the pulp chamber of teeth. The penetration of hydrogen peroxide into the pulp chamber of teeth is more in restored teeth than in intact teeth and in restored teeth, resin modified glass ionomer cements show greater peroxide penetration into the pulp than hybrid composite resins.
Further in-vivo research is required to validate the results of this in vitro study and determine the penetration of peroxide into the pulp and establish the concentration of peroxide that causes irreversible damage to the pulp.
• DW : Distilled water
• 30% H2O2 : 30% Hydrogen peroxide
*Significant