Replication of Palatal Rugae and Incorporation in Complete Denture
Sushil Kar1, Arvind Tripathi2, Riti Madhok3
1 Professor, Department of Prosthodontics, Saraswati Dental College, Lucknow, Uttar Pradesh, India.
2 Professor and Head, Department of Prosthodontics, Saraswati Dental College, Lucknow, Uttar Pradesh, India.
3 Junior Resident, Department of Prosthodontics, Saraswati Dental College, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sushil Kar, Saraswati Dental College, 233, Tiwari Ganj, Faizabad Road, Lucknow-227105, Uttar Pradesh, India.
E-mail: drsushil_kar@yahoo.co.in
Anatomic landmark, Maxilla, Speech
In complete denture prosthodontics, phonetics is one of the most important factors to be taken into consideration. Often complete denture wearers complain of improper pronunciation of certain words which is attributed to the rugae form and palatal contour [1].
The prominent ridges present on either side of the mid palatine raphe across the anterior portion of the palate constitute the rugae palatine, commonly referred to rugae. For audible phonation, the tongue must make accurate approximation with the palate. An overly thick or thin denture prosthesis in the region of anterior palate hampers appropriate formation of palato-lingual sounds [2]. Thus, the replication of soft tissue contours favours the formation and pronunciation of Sibilants as clearly as a normal dentate individual.
Precise reproduction of this particular soft tissue landmark in the complete denture not only enhances phonetics but also aids in mastication, deglutition and better taste perception [3]. This article enumerates the various steps taken for accurate replication of the existing palatal rugae in the complete denture prosthesis.
Technique
Make maxillary and mandibular primary impressions using impression compound and obtain primary casts. Fabricate 2mm short special trays with autopolymerizing resin (DPI RR cold cure, India). Following border moulding, take final impressions with light body impression material (Xantopren M Mucosa; Heraeus Kulzer, Hanau, Germany) [Table/Fig-1].
Observe and outline the palatal rugae area in the patient’s mouth using an indelible pencil [Table/Fig-2]. Transfer the outlined area onto the intaglio surface of the maxillary final impression by reseating the impression in the patient’s mouth [Table/Fig-3].
Prepare a thin, clear acrylic stent over the transferred rugae outline on the final impression using sprinkle on method. Ensure accurate reproduction of the palatal rugae elevations. Once set, remove the acrylic stent from the impression and trim carefully.
Pour final impression with Type III dental stone (Dentstone; Pankaj Industries, Mumbai, India) to obtain maxillary cast [Table/Fig-4]. Record tentative jaw relation and verify trial denture following teeth arrangement.
Remove part of trial denture base from the demarcated palatal rugae area [Table/Fig-5] and replace it with the acrylic stent prepared earlier [Table/Fig-6].
Wax up, process, finish and polish according to conventional procedure [Table/Fig-7].

Rugae area demarcated with indelible pencil.

Marked area transferred into the impression.
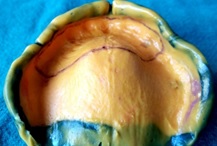
Poured cast with the delineated rugae area.

Demarcated area removed from the denture base.

Thin shell of duplicated rugae waxed into the denture base.

Processed denture with replicated rugae.

A thin tin foil was adapted on the palatal area to facilitate easy removal of the acrylic stent without damaging the cast. The important part here is the adaptation of a thin foil on the cast before packing and flasking during the curing procedure.
A trained speech therapist was recruited to observe the improvement in speech. Sounds such as th, t, d, s, g, j, l, n, r, w, x, z were used to observe the improvement of speech.
Discussion
Palatal rugae plays a very important role in phonetics. The absence of rugae impedes proper articulation due to the lack of tactile sense. The patient’s own rugae can be transferred to the palatal surface of the denture in a number of ways. This can be attained by using plastic palate forms, corrugated metal palate and free hand wax carving of anatomic palate [4]. Another procedure to replicate rugae involves the use of interdental floss, which duplicates the width and thickness of rugae [5].
The technique of rugae transfer followed by replication in the present technique allows for an efficacious formation of palato-lingual words, which in turn, enhances the patients’ adaptability to the prosthesis. Another advantage is the lack of requirement of an elaborate armamentarium for the duplication process.
However, during curing of the denture, there could be incorporation of voids or other processing errors on the intaglio surface. This could lead to uncomfortable fit and abrasion of the mucosa. Therefore, this method is technique sensitive and requires careful processing. Conventional complete dentures do not provide palatal rugae duplication and therefore leads to altered speech, especially the linguopalatal sounds. This technique improves speech and patient comfort drastically. Further to this study, the rugae duplication will be done by metal inserts and the efficacy of acrylic rugae and metal rugae will then be evaluated.
[1]. Rothman R, Phonetic considerations in denture prosthesisJ Prosthet Dent 1961 11(1):214-23. [Google Scholar]
[2]. Allen LR, Improved phonetics in denture constructionJ Prosthet Dent 1958 8:753-63. [Google Scholar]
[3]. Palmer JM, Structural changes for speech improvement in complete upper denture fabricationJ Prosthet Dent 1979 41(5):507-10. [Google Scholar]
[4]. Rogers OW, Electroformed metal plates for complete denturesJ Prosthet Dent 1970 23(2):207-17. [Google Scholar]
[5]. Vijayaraghavan V, Chandani P, A simple method for palatal rugae carving in complete denturesJ Indian Prosthodont Soc 2013 13(2):137-38. [Google Scholar]