Smile Reconstruction for the Preschoolers Using GRASCE Appliance – Two Case Reports
A.K. Shanmugaavel1, Deepa Gurunathan2, Lavanya Sundararajan3
1 Senior Lecturer, Department of Pediatric and Preventive Dentistry, Saveetha Dental College and Hospitals, Chennai, Tamilnadu, India.
2 Reader, Department of Pediatric and Preventive Dentistry, Saveetha Dental College and Hospitals, Chennai, Tamilnadu, India.
3 Postgraduate Student, Department of Pediatric and Preventive Dentistry, Saveetha Dental College and Hospitals, Chennai, Tamilnadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. A.K. Shanmugaavel, Senior Lecturer, Department of Pediatric and Preventive Dentistry, Saveetha Dental College and Hospitals, Chennai, Tamilnadu-600095, India.
E-mail: dentistshan@gmail.com
Preschoolers with early childhood caries or extensive dental trauma may suffer from abnormal social interaction with their peers. Dentists face great challenges in the aesthetic rehabilitation of these young children. As the parental desire towards aesthetics is gaining more importance there is need for an anterior aesthetic appliance which may be used to replace these lost teeth. These case reports highlight a specific design which can be used successfully in day to day clinical practice.
Aesthetics, Children, Deciduous root stumps, Primary teeth, Rehabilitation
Case 1
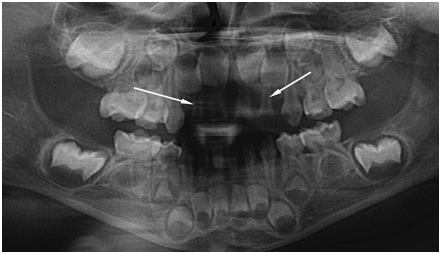
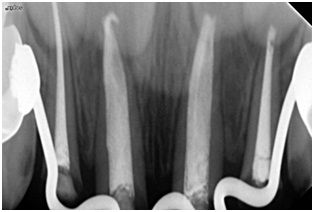
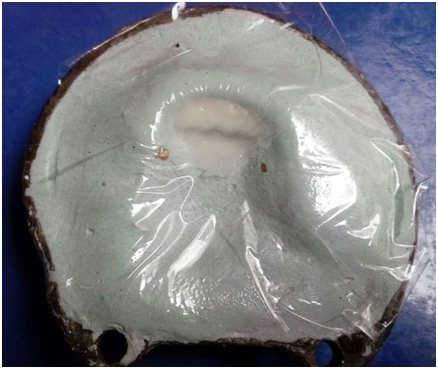
A three and half year old healthy female child reported with a chief complaint of pain in the upper front teeth region. The medical history was non-contributory. The child had dull, had continuous pain for past one week. Extra oral examination revealed a bilateral symmetrical facial appearance. On intra oral clinical examination there was severe tooth loss with root stumps of teeth 51, 52, 61 and 62 [Table/Fig-1]. The decay pattern was Class I in teeth 55, 65, 75 and 85, Class II in teeth 54 and 64 and Class V in teeth 53 and 63. Radiographic evaluation of teeth 52, 51, 61 and 62, showed a favorable root length and bone height [Table/Fig-2]. A diagnosis of severe early childhood caries was made. Caries status of the child was controlled by restoring 55, 65, 54, 64, 75, 85, 53 and 63 with composite restoration. After obtaining the consent from the parents, as there was favorable root length and bone height, pulpectomy was performed in teeth 52, 51, 61 and 62 [Table/Fig-3] followed by composite restoration and Stainless Steel (SS) crown preparation in 54 and 64 in accordance with the UK national guidelines [1]. Care was taken to seat the prefabricated stainless steel crown (3M ESPSE, United States) with downward pressure. Elastomeric impressions were made and the SS crowns were transferred on to the impression, stabilized in position [Table/Fig-4], followed by the fabrication and insertion of the “Groper’s Appliance with Stainless Steel Crown and Customized Teeth (GRASCE)” as shown in [Table/Fig-5].
Pre-operative intraoral frontal view.

Pre-operative orthopantamograph.
Post-operative radiovisiography showing pulpectomy, favorable root length and bone height.
Elastomeric impression with the prefabricated stainless steel crown.

Post-operative intraoral frontal view.

Steps in Fabrication of “GRASCE” Appliance
One study model and a working model were prepared.
A multiple U bend was made with wire of 0.9mm in diameter [Table/Fig-6]. This design extended from the palatal surface of the pre-fabricated stainless steel crown which was placed on the first primary molar to the palatal surface of the opposing first primary molar.
Once the wire component was stabilized, the wire was soldered [Table/Fig-7] to the crown followed by a customized teeth wax up [Table/Fig-8,9] for the upper incisors. A buccal extension was avoided to give better aesthetics and as well as to prevent hindrance to growth of maxillary arch.
The prepared waxed up model was then subjected to reverse flasking, dewaxing, packing and curing [Table/Fig-10,11 and 12] with tooth colored heat polymerizing resin.
The untrimmed appliance was then trimmed with acrylic burs, and final finishing and polishing were done with pumice [Table/Fig-13,14 and 15].
Model with the wire framework.

Soldered wire framework to the prefabricated stainless steel crown.


Customized teeth wax up frontal view.

Reverse flasking of the model.


Packing of the tooth colored resin material.


Finished and polished Appliance.

Insertion of the Appliance
The appliance was inserted and cemented using glass ionomer (Fuji I, Japan) cement after checking for any occlusal disturbances. The child was recalled and reviewed at 7days, 14days, 1 month and every 3 months interval till one year. His speech was as normal as before. There were no clinical signs of failure of appliance such as irritation to the gingiva, difficulty in mastication, fracture or abrasion of the acrylic component, fracture of the solder, dislodgment of the crown and discoloration of the teeth. The Pre-operative and Post-operative pictures are illustrated in [Table/Fig-1,5] respectively. The parents were also very satisfied with the appliance and they reported that the child’s eating pattern and psychological behavior has improved. As this is a newer treatment option of retaining the roots of deciduous tooth with crown structure damaged till the Cemento-Enamel Junction (CEJ) and placement of the appliance, a long follow up is planned and the patient is still on follow up at regular intervals.
Case 2
An apparently healthy two and a half year old male child reported complaining of decayed front teeth in the maxilla. The medical history was non-contributory. The past dental history revealed that the child was bottle fed up to 2 yrs of age. On extra oral examination, there was a diffuse swelling confined to the upper lip in correlation with the decayed maxillary incisors. Intra oral examination revealed severely affected maxillary anterior teeth with only root stumps visible. Dental caries involving the mesial and distal portion of 54 and 64 were evaluated [Table/Fig-16]. Radiographic presentation showed pathologic root resorption in relation to teeth 51, 61 and internal resorption in tooth 62 [Table/Fig-17]. A diagnosis of severe early childhood caries with irreversible pulpitis in teeth 52, 51, 61 and 62 were made based on clinical and radiographic presentation. As the child was too young immediate intervention was not initiated. On review after antibiotic regimen for three days, the upper lip became normal and child was asymptomatic. The treatment plan was explained to the parents and after obtaining the informed written consent extraction of teeth 52, 51, 61 and 62 was done under local anesthesia. The extraction of 52 was done in order to favor eruption of both the lateral incisors at the same time. An active physical restraint was used to control the child’s behavior during extraction. One month interval was given for healing of the sockets [Table/Fig-18]. Pulpectomy and SS crown preparation was done in teeth 54 and 64 followed by the fabrication and insertion of the GRASCE appliance [Table/Fig-19]. On recall visit at 2 weeks [Table/Fig-20], 1 month, 4 months and 7months [Table/Fig-21,22] the child had adapted to the appliance well. The intraoral Pre-operative and post-operative pictures are illustrated in [Table/Fig-18,19] respectively. We also observed that the behavior of the child improved from Frankl’s negative (-) behavior to Frankl’s definitely positive (++) behavior in the dental operatory. As the child was managed with a newer appliance a long term follow-up was planned. The parents were satisfied and on a regular follow-up till date the child shows a more positive attitude towards maintenance of oral hygiene.
Pre-operative intraoral occlusal view.

Pre-operative phosphorplate radiography.

Pre-operative frontal view after the extraction of anterior teeth.

Immediate Post-operative frontal view.

Post-operative occlusal view after 2 weeks.

Extraoral Post-operative view after 4 months.

Extraoral Post-operative view after 7 months.

Discussion
Historical evidence states that space maintainers are not required for the loss of upper anterior teeth after eruption of the canine [2]. However, Kapur et al., reported that aesthetic rehabilitation of the primary dentition had a psychological impact on the recovery of the child’s self esteem [3]. Hence pulpectomy should be considered as the first line of treatment option for teeth with favorable root length and alveolar bone height. The advantage of pulpectomy over extraction includes normal eruption pattern, continued alveolar bone growth and less traumatic psychological experience to the child in the dental operatory.
Aesthetic restoration of primary anterior teeth is still a challenge to the pediatric dentist. The different treatment options available for restoring esthetics in primary teeth include intracoronal restorations which utilize resin composites, glass ionomer cements, resin-modified ionomers, or polyacid-modified resins [4]. Full coronal restoration for primary incisors include restorations that are directly bonded onto the tooth, such as a resin material and crowns that are luted onto the tooth that are either a preveneered stainless steel or zirconia crown [4]. In case of severe loss of coronal tooth structure as seen in severe early childhood caries or early loss of primary teeth GROPER’s appliance was used to restore the aesthetics. Pulpectomy followed by intracoronal biological post and omega loop retainers were the treatment option as suggested by Grewal et al., for the primary tooth with more than half to three fourth of crown tooth structure [5]. While Waggoner et al., has advised for same day extraction and appliance placement with excellent outcome [4]. This case report presents a newer treatment option of retaining the deciduous tooth with crown structure damaged till the CEJ and placement of the appliance. This would facilitate the eruption of the succedenous teeth in a normal manner and maintain the alveolar bone height. The original GROPER’s appliance introduced by Jasmin and Groper in 1984 consists of acrylic teeth attached to metal clefts which were soldered onto the palatal wire [6]. Due to the strenuous laboratory procedures the appliance was modified incorporating preformed acrylic teeth and buccal acrylic flange [7,8]. The limitations of this appliance includes larger tooth size, gingival inflammation associated with the buccal acrylic flange, occlusal disturbances and secondary caries due to cement loss in the primary molars. To overcome these limitations the appliance is modified and named as GRASCE appliance.
The appliance design is similar to GROPER’s appliance with a round wire of diameter 0.036 to 0.040 inch attached to a prefabricated SS crown in the primary first molars. First primary molars are preferred as abutments than primary second molar due to the shorter wire span and less potential interference with the erupting first permanent molars [9]. The stainless steel crowns were preferred over orthodontic bands as they serve as more secure abutments [9] as well as the maintenance of SS crowns is much simpler to children and their parents in comparison to placement of bands on molar teeth. In addition SS crowns help in prevention of further decay even in the absence of missed appointments for fluoride application.
As per the knowledge of authors only prefabricated acrylic moulds are available (3M ESPE Polycarbonate Crowns) and not the entire tooth structure. Hence, customized acrylic tooth in accordance with the facial morphology of the child was prepared. The advantage of customized acrylic teeth is that it gives an aesthetic appearance as it is individualized to shape and size of each child. The gum fit in this design makes the teeth to rest directly over the alveolar ridge without any acrylic flange extending over the vestibule. This helps to prevent the gingival inflammation and irritation. The acrylic component on the palatal side serves as a major connector stabilizing the wire component to the customized teeth. The thickness of the acrylic ranges from 1mm to 2mm making it more convenient for the child during mastication and speech. In addition, these appliances do not hinder the intercanine growth in width as stated by Scures in 1967 that the intercanine growth in width between 2 to 4 years was less than 0.5mm and it was clinically insignificant [10].
The limitations of this appliance include removal as a whole unit when the first upper permanent central incisor makes its appearance in the oral cavity. However, this may not affect the self esteem of the children as these children fit into the group of school going children who are in the mixed dentition stage with normal exfoliating incisors.
Conclusion
Replacement of the missing incisors with GRASCE appliance provides a reasonable treatment option for preschool children with severe early childhood caries or early dental trauma. The simple technique in fabrication of the appliance allows it to be used in daily clinical practice with greater success both to the child in establishing a positive attitude and the dentist in aesthetic replacement of the missing teeth.
[1]. Kindelan SA, Day P, Nichol R, Willmott N, Fayle SA, British Society of Paediatric DentistryUK National Clinical Guidelines in Paediatric Dentistry: stainless steel preformed crowns for primary molarsInt J Paediatr Dent 2008 18(Suppl 1):20-28. [Google Scholar]
[2]. Christensen JR, Fields HW, Space maintenance in the primary dentitionIn Pediatric Dentistry: Infancy Through Adolescence. Pinkham JR ed 1994 2nd edPhiladelphiaW.B. Saunders Company:358-63. [Google Scholar]
[3]. Kapur A, Chawla HS, Goyal A, Gaube K, An esthetic point of view in very young childrenJ Clin Pediatr Dent 2005 30(2):99-103. [Google Scholar]
[4]. Waggoner WF, Restoring primary anterior teeth: updated for 2014Pediatr Dent 2015 37(2):163-70. [Google Scholar]
[5]. Grewal N, Seth R, Comparative in vivo evaluation of restoring severely mutilated primary anterior teeth with biological post and crown preparation and reinforced composite restorationJ Indian Soc Pedod Prev Dent 2008 26:141-48. [Google Scholar]
[6]. Jasmin JR, Groper JN, Fabrication of a more durable fixed anterior esthetic applianceJ Dent Child 1984 51(2):124-27. [Google Scholar]
[7]. Khare V, Nayak PA, Khandelwal V, Nayak UA, Fixed functional space maintainer: novel aesthetic approach for missing maxillary primary anterior teethBMJ Case Rep 2013 :1-4.doi:10.1136/bcr-2013-009585 [Google Scholar]
[8]. Chalakkal P, Devi RS, Srinivas G. V, Venkataramana P, Dentulous appliance for upper anterior edentulous spanJ Clin Diagn Res 2013 7(12):3086-87. [Google Scholar]
[9]. Waggoner WF, Kupietzky A, Anterior esthetic fixed appliances for the preschooler: considerations and a technique for placementPediatr Dent 2001 23(2):147-50. [Google Scholar]
[10]. Scures CC, Report of the increase in bicanine diameter in 2 to 4 -year-old childrenJ Dent Child 1967 34:332-35. [Google Scholar]