Tropical Acute Febrile Illness (TAFI) is defined as all acute febrile syndromes with oral temperature over 37.5oc within the last 24 hours and less than two weeks, in tropical and sub tropical developing countries with non specific symptoms that include all the symptoms that will not help us to localize to a particular system and are the usual complaints of a person with acute febrile illness like fever, generalized body pain, loose stools, vomiting, swelling of legs, generalized swelling of the body, decreased urine output, breathlessness, cough, chest pain, altered sensorium, headache and others and non specific signs that include all the signs that will not help us to localize to a particular system like fever, tachycardia, myalgia, conjunctival congestion, rashes, joint pains and others [1–7]. TAFI with Acute Kidney Injury (AKI) was a major cause of mortality [4,6]. Malaria was over diagnosed [8]. Emerging and re-emerging diseases, population growth, urbanization, migration, international travel, pandemics, global warming complicate matters [7,9,10]. AKI management requires latest guidelines [11]. The present situation demands a better syndromic approach, early treatment and prevention of complications [7].
Materials and Methods
A total of 600 hospitalized TAFI patients were prospectively studied at a tertiary care centre affiliated to a private medical college in coastal Karnataka between September 2012 and September 2014 for the aetiology of TAFI; the development and staging of AKI based on Kidney Disease: Improving Global Outcomes (KDIGO) guidelines; the initiation of RRT and in-hospital mortality.
Patients aged more than 18 years with TAFI were included in the study. Patients aged less than 18 years with nosocomial and chronic infections, fever with single system involvement, non infectious aetiologies and of unknown origin, chronic kidney disease, acute kidney injury secondary to non infectious aetiologies, and lastly, immunocompromised and immunosuppressed individuals and pregnant females were excluded from the study.
Informed consent, history, examination, a set of routine blood and urine investigations, peripheral blood smears for malaria, chest radiograph, abdominal ultrasonogram for all patients and blood cultures (BacT/ALERT and VITEK, bioMérieux, North Carolina, USA) for enteric fever, leptospiral IgM ELISA (PAN Bio Ltd, Brisbane, Australia), dengue IgM (PAN Bio Ltd, Brisbane, Australia), Weil Felix for rickettsiae (PROGEN, TULIP diagnostics Ltd, Goa, India) and arterial blood gas analysis for appropriate patients. The values provided by manufacturers were used for test interpretation.
KDIGO guidelines were used for AKI diagnosis and classification. Management was based on standard guidelines. Indicated patients were initiated on Renal Replacement Therapy (RRT) in form of Intermittent Venovenous RRT (IVVRRT) and Sustained Low-Efficiency Daily RRT initiation (SLEDD). Catheters and catheter sites were selected as per the KDIGO guidelines. RRT initiation and in-hospital mortality were the primary outcomes.
Statistical Analysis
Data analysis was done using SPSS version 17.0 with statistical significance calculated using chi-square and Fisher’s exact t-test for which p-value < 0.05 was considered significant. Sample size was calculated based on study by Basu G et al., for a power of 90% and the sample size was set at 600 [3].
Results
Renal Replacement Therapy (RRT) Initiation
RRT initiation was observed in 33 (10.2%) of AKI patients. Among patients with AKI stage 1, 2 and 3, RRT was initiated in 3 (9.1%), 1 (3.0%) and 29 (87.9%) [Table/Fig-1]. Of the patients with AKI, 291 (89.8%) were treated conservatively and 33 patients (10.2%) were initiated on RRT. A total of 31 AKI patients (93.9%) were dialyzed once a day while two patients (6.1%) received RRT initiation twice in the same day. Among the total of 33 patients who were haemodialysed, 26 patients (78.8%) have received RRT for a maximum of three times while only seven patients (21.2%) received RRT for more than three times. Of AKI stage 1, 2 and 3, 9.1%, 3.0% and 87.9% underwent RRT respectively. The total number of times haemodialysed correlated significantly with the AKI stage and the in-hospital mortality of the patient. RRT has statistically altered all three parameters namely –creatinine, urea and urine output when the baseline values were compared with the discharge value. Out of all the 33 dialyzed patients, 27 (81.8%) improved and 6 (18.2%) died. On statistical analysis RRT was a positive predictor of in-hospital mortality.
In-hospital Mortality
The in-hospital mortality was 18 (3%) among TAFI patients, of which 17 (94.4%) had AKI, of which 15 (88.2%) were of AKI stage 3 and, of which 9 (60%) patients died before the initiation of RRT, and of which all 9 (100%) had leptospirosis [Table/Fig-1]. AKI was a statistically significant predictor of death. Among the AKI stages, stage 3 has the greatest statistical significance with respect to in-hospital mortality. The most common cause of AKI stage 1, 2, 3, RRT initiation and in-hospital mortality was leptospirosis 17.8% (27), 54.5% (55), 94.4% (67), 88% (29) and 88.8% (16), respectively.
AKI, AKI stages, RRT initiation and In-hospital mortality in TAFI.
| AKI | AKI stages | RRT initiation | In-hospital mortality |
|---|
| n (%) | n (%) | n (%) | n (%) |
|---|
| 324 (54) | Stage 1 – 152 (25.5)Stage 2 – 101 (16.5)Stage 3 – 71 (11.8) | AKI – 33 (5.5)Stage 1 – 3 (0.5)Stage 2 – 1 (0.17)Stage 3 – 29 (4.83) | TAFI – 18 (3)AKI – 17 (2.9)Stage 1 – 1 (0.17)Stage 2 – 1 (0.17)Stage 3 – 15 (2.5) |
TAFI - Tropical acute febrile illness, AKI - Acute kidney injury, RRT - renal replacement therapy.
Spectrum of Tropical Acute Febrile Illness
The spectrum of TAFI, in decreasing order, was vivax malaria (203, 33.8%), leptospirosis (151, 25.2%), dengue fever (85, 14.2%), falciparum malaria (49, 8.2%), mixed malaria (37, 6.2%), enteric fever (7, 1.2%), scrub typhus (5, 0.8%), undifferentiated (63, 10.5%), and the most common aetiology was malaria (289, 48.17%) including vivax (203 out of 289, 70.2%), falciparum (49, 17.0%) and mixed (37, 12.8%) malaria [Table/Fig-2].
The spectrum of aetiologies among TAFI, AKI, AKI stages, RRT initiation and In-hospital mortality
| Malaria | Leptospirosis | Dengue fever | Enteric fever | Scrub typhus | Undifferentiated | Total |
|---|
| Vivax malaria | Falciparum malaria | Mixed malaria |
|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
|---|
| TAFI | 203(33.8) | 49 (8.1) | 37 (6.2) | 151(25.2) | 85(14.2) | 7 (1.2) | 5(0.8) | 63(10.5) | 600 |
| AKI | 62(19.1) | 24(7.3) | 15(4.6) | 149(45.8) | 59(18.2) | 3 (0.9) | 2(0.7) | 10(3.1) | 324 |
| AKI Stage 1 | 40(26.3) | 8(5.2) | 10(6.6) | 27(17.8) | 52(34.2) | 3(2) | 2(1.3) | 10(6.6) | 152 |
| AKI Stage 2 | 22(21.8) | 15(14.9) | 5(4.9) | 55(54.5) | 4(3.9) | 0 | 0 | 0 | 101 |
| AKI Stage 3 | 1(1.4) | 0 | 0 | 67(94.4) | 3(4.2) | 0 | 0 | 0 | 71 |
| RRT Initiation | 1(3) | 1(3) | 1(3) | 29(88) | 1(3) | 0 | 0 | 0 | 33 |
| In-hospital Mortality | 0 | 0 | 0 | 16(88.8) | 1(5.6) | 0 | 0 | 1(5.6) | 18 |
TAFI - Tropical acute febrile illness, AKI - Acute kidney injury, RRT - renal replacement therapy.
Proportion and Spectrum of Acute Kidney Injury
The proportion of AKI was 324 out of 600 patients, 54% based on KDIGO guidelines [Table/Fig-1]. The spectrum of AKI, in decreasing order, was leptospirosis (149, 45.8%), vivax malaria (62, 19.1%), dengue fever (59, 18.2%), falciparum malaria (24, 7.3%), mixed malaria (15, 4.6%), undiagnosed (10, 3.1%), enteric fever (3, 1.2%), scrub typhus (2,0.7%) [Table/Fig-2]. The most common cause of AKI (149 out of 324, 45.8%), AKI stage 2 (55 out of 101, 54.5%), stage 3 (67,out of 71, 94.4%), RRT initiation (29 out of 33, 88%) and in-hospital mortality (16 out of 18, 88.8%) was leptospirosis; and AKI stage 1 (52, 34.2%) was dengue fever. Together leptospirosis, dengue fever and vivax malaria accounted for more than four-fifth of AKI among the patients. Also malaria (falciparum, vivax and mixed) contributed to one-third of total number of patients with AKI. Thus, even though malaria patients were more in number, AKI was mostly due to leptospirosis.
AKI was present in almost all patients with leptospirosis [Table/Fig-3]. 70% of dengue patients had AKI. Almost half of falciparum malaria patients had AKI. Two-fifth of scrub typhus patients also has AKI. More than one-third of mixed malaria patients have AKI. About one-third of enteric fever patients also have AKI. AKI was seen in about one-third of vivax malaria patients. Also one third of patients with undiagnosed TAFI developed AKI.
AKI, AKI stages, RRT initiation and In-hospital mortality with respect to the number of patients with each aetiology
| | AKI | AKI Stage1 | AKI Stage2 | AKI Stage3 | RRT Initiation | In-hospital Mortality | Total |
|---|
| | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n |
|---|
| Malaria | Vivax | 62 (30.5) | 40 (19.7) | 22 (10.8) | 0 | 1 (0.5) | 0 | 203 |
| Falciparum | 24 (49) | 8 (16.4) | 10 (30.6) | 1 (2) | 1 (2) | 0 | 49 |
| Mixed | 15 (40.5) | 10 (27) | 5 (13.5) | 0 | 1 (2.7) | 0 | 37 |
| Leptospirosis | 149 (98.7) | 27 (17.9) | 55 (36.4) | 67 (44.4) | 29 (19.3) | 16 (10.6) | 151 |
| Dengue fever | 59 (69.4) | 52 (61.2) | 4 (4.7) | 3 (3.5) | 1 (1.2) | 1 (1.2) | 85 |
| Enteric fever | 3 (42.9) | 3 (42.9) | 0 | 0 | 0 | 0 | 7 |
| Scrub typhus | 2 (40) | 2 (40) | 0 | 0 | 0 | 0 | 5 |
| Undifferentiated | 10 (15.9) | 10 (15.9) | 0 | 0 | 0 | 1 (1.6) | 63 |
AKI - Acute kidney injury, RRT - renal replacement therapy.
Staging of Acute Kidney Injury
KDIGO AKI stage 1, 2 and 3 was seen in 152 (46.9%), 101 (31.2%) and 71(21.9%) of AKI patients, respectively [Table/Fig-1]. The increase in AKI staging is associated with increased in-hospital mortality (KDIGO, Stage 1 – 1 (0.17%), Stage 2 – 1 (0.17%), Stage 3–15 (2.5%)). AKI stage 3 significantly correlated with the in-hospital mortality in the patients.
Baseline Characteristics
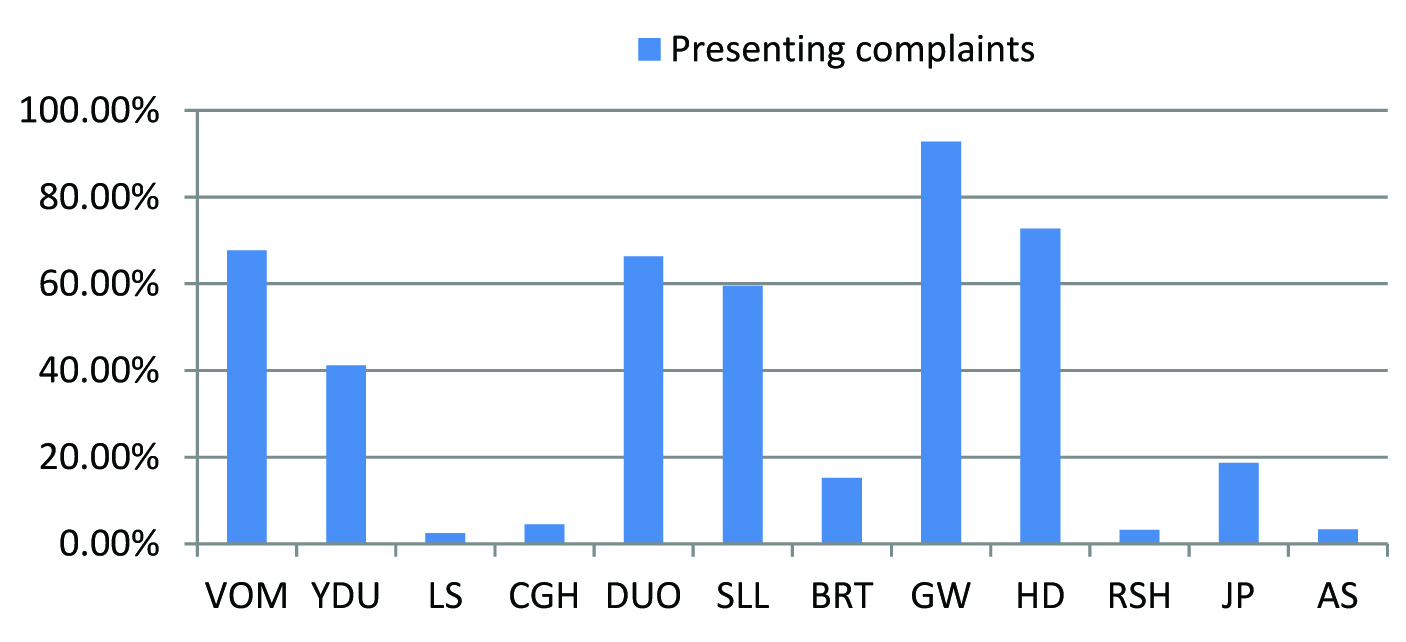
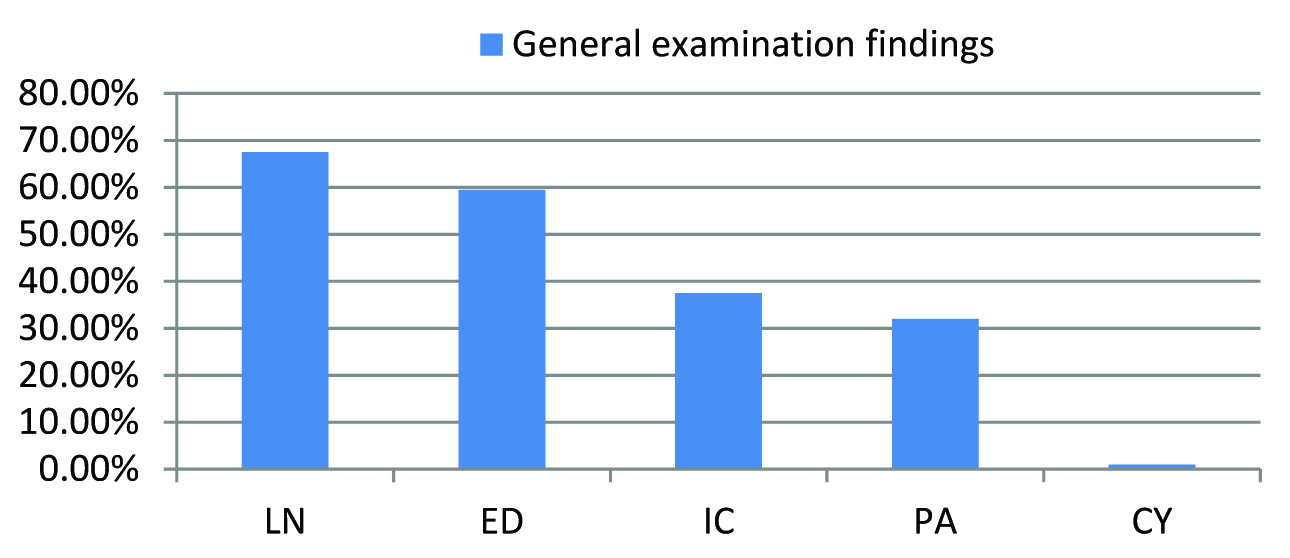
Almost three-fourth of the patients was less than 50 years of age. The mean age was 40.34 years with a standard deviation of 15.42 years. Age positively correlated with AKI staging. More than three fourth of all patients were males. More than two-thirds was manual laborers while about one-thirds was farmers. About three-fourth of the patients gave a history of alcoholism and more than half were smokers. The correlation of both alcoholism and smoking with in-hospital mortality was statistically significant. [Table/Fig-4] shows distribution of presenting complaints among tropical acute febrile illness patients. About three-fourth (72%) of the patients had fever of 4-6 days duration at the time of admission, while 17% had fever of 1-3 days duration and only 11% had more than 7 days of fever. Fever duration was significantly related to AKI staging. Cough was significantly related to AKI. Generalized weakness was significantly related to AKI staging. Vomiting, yellowish discoloration of urine, decreased urine output, swelling of lower limbs, breathlessness, headache and joint pain were significantly related to AKI and its staging. Altered sensorium was significantly related to AKI, its staging and in-hospital mortality. [Table/Fig-5] shows distribution of general examination findings among acute febrile illness patients.
Distribution of presenting complaints among tropical acute febrile illness patients. VOM vomiting, YDU yellowish discoloration of urine, LS loose stools, CGH cough, DUO decreased urine output, SLL swelling of lower limbs, BRT breathlessness, GW generalised weakness, HD headache, RSH rash, JP joint pains, AS altered sensorium.
Distribution of general examination findings among acute febrile illness patients. LN lymphadenopathy, ED edema, IC icterus, PA pallor, CY cyanosis.
Discussion
In this study we show that the spectrum of TAFI was different from that of studies in Karnataka by Mohan TSR et al., Kashinkunti MD et al., other parts of south India by Basu G et al., Chrispal A et al., other parts of India by Joshi R et al., Singh R et al., Southeast Asia by Leelarasamee A et al., Kasper MR et al., other tropical countries by Crump JA et al., reviews and meta-analyses by Susilawati et al., Prasad et al., and Joshi R et al., [3–5,7,12–17]. This was probably due to the unique topography and demography of coastal Karnataka. This study will help health care workers for syndromic approach to diagnosis. This will also help in management of fever in tropical travelers returning from this region as well as the study of local and global trends of TAFI.
The most common cause of TAFI was vivax malaria and broadly, malaria, as opposed to leptospirosis, scrub typhus, dengue fever in other studies. Kasper MR et al., - influenza, Crump JA et al., - bacterial bloodstream infections and broadly, bacterial zoonoses [3,5,7,12–16]. The endemicity of malaria in the districts of coastal Karnataka may be one of the probable reasons for malaria being the most common aetiology of TAFI.
The proportion of vivax, falciparum and mixed malaria was also different from studies by Bhandary N., Basu G et al., Saravu K et al., and Kasper et al., [3,7,18,19]. The proportion of dengue fever and leptospirosis may be explained by the epidemiological and demographical profile of the patients, i.e. manual laborers exposed to day biting aedes mosquitoes and farmers exposed to contaminated water, respectively.
In this study the proportion of AKI was more than most of the studies, like those by Bhandary N, Kashinkunti MD et al., by Basu G et al., [3,13,18]. This may be due to the AKI criteria used in the studies. RIFLE criteria had been shown to categorize greater number of patients with AKI than the WHO 2006 criteria by Thanachartwet V et al., [20]. Thus the presence of 54% AKI in TAFI patients in this study may be due to the greater sensitivity of the KDIGO criteria. Patients with AKI had to be treated aggressively as it was a significant positive predictor of impending death similar to study by Saravu K et al., and Waikar SS et al., [19,21].
The spectrum of AKI was different as compared to study by Basu G et al., [3]. The most common cause of AKI, its stages 2 and 3, RRT initiation and in-hospital mortality was leptospirosis; and AKI stage 1 was dengue fever as opposed to studies by Basu G et al., - scrub typhus and Daher EDF et al.,– HIV/AIDS [22]. The greatest proportion of AKI was seen in leptospirosis as compared to studies by Basu G et al.,– falciparum malaria [3]. This may be due to the greater nephrotoxicity of the local leptospiral serovars or greater susceptibility of the study population to AKI and more severe AKI. The proportion of malaria patients with AKI, severe AKI, RRT initiation and in-hospital mortality differed from studies by Bhandary N., Basu G et al., Saravu K et al., Kute VB et al., and Gupta BK et al., [3,18,19,23,24].
The decreasing number of AKI patients with increase in AKI staging had been observed in other studies by Bhandary N., Basu G et al., and Saravu K et al., [3,18,19]. The proportion of AKI stage 1 patients may represent the usually asymptomatic and undiagnosed cases of AKI who can be better detected using a more sensitive criteria like that of KDIGO. In this study, among the AKI stages, stage 3 was associated with the highest in-hospital mortality.
Also it was seen that with increase in AKI stage more number of patients were initiated on RRT. This had been observed in other studies by Basu G et al., and Thanachartwet V et al., [3,20].
It was also seen that about 10% of AKI patients required RRT. RRT initiation and greater number of times dialyzed had statistical significance as predictor of in-hospital mortality similar to studies by Palevsky PM et al., [25]. RRT statistically alters discharge creatinine, urea and urine output when compared to the baseline values, but may not alter in-hospital mortality.
Similarly it was seen that increase in stage of AKI had increased in-hospital mortality as observed in other studies by Basu G et al., and Thanachartwet V et al., [3,20].
Among the baseline characteristics, mean age 40.8 years were found to be similar to study by Basu G et al., of 39.7 years [3].
The positive predictors of AKI from this study [Table/Fig-6] may be compared to Saravu K et al., Basu G et al., and Prakash J et al., [3,19,26], while those of RRT initiation can be compared with Basu G et al., [3]. Finally, the positive predictors of in-hospital mortality may be compared to Basu G et al., Daher EDF et al., Ostermann M et al., Chertow GM et al., Gallagher M et al., and Aldawood A [3,22,27–30].
Positive predictors (p<0.001) of AKI, AKI stage, RRT initiation, In-hospital mortality. AKI - Acute kidney injury, RRT - renal replacement therapy
| AKI | AKI stage3 | RRT initiation | In-hospital mortality |
|---|
| leptospirosis, dengue, falciparum malaria, fever duration, decreased urine output, swelling of lower limbs, breathlessness, vomiting, yellowish discoloration of urine, altered sensorium, edema, pallor, icterus, | higher age, fever duration, decreased urine output, swelling of lower limbs, breathlessness, vomiting, yellowish discoloration of urine, altered sensorium, edema, pallor, icterus | AKI stage 3, leptospirosis, dengue, falciparum malaria, altered sensorium, alcoholism, smoking, baseline and repeat creatinine, creatinine>4mg/dl, absolute and percentage creatinine increase, baseline and repeat urea, urine output in the first and subsequent day, arterial blood gas | AKI stage 3, RRT initiation, leptospirosis, dengue, falciparum malaria, Dialysis total number of times haemodialysed, altered sensorium, alcoholism, smoking, baseline and repeat creatinine, creatinine>4mg/dl, absolute and percentage creatinine increase, baseline and repeat urea, urine output in the first and subsequent day, arterial blood gas |
All parameters were significant with p-value <0.01. The positive associations of in-hospital mortality were analysed using Pearson’s chi chi-square test, Mann Whiteney test and Fisher’s exact test as appropriate to the parameters
Merits
This is one of the few studies in this region that outlines the epidemiological spectrum of acute febrile syndromes. As the sample size has ninety percent power with ninety five percent confidence intervals, reliable conclusions may be drawn. Patients with the most severe stages of acute kidney injury were studied which has helped in providing information regarding its management and prognosis.
Limitation
TAFI and AKI patients may be missed due to asymptomatic disease, uncomplicated disease manageable at lower centre, non referral, treatment initiation before presentation, death before admission. Also the study population would have had more severe illness and hence acute kidney injury proportion may be an overestimation. As there was no serum creatinine values prior to admission possibility of acute on chronic renal failure cannot be excluded. A larger sample size may provide more significant results. Study on eGFR (estimated Glomerular Filtration Rate), clinical stage scoring, mechanical ventilation, inotropic support and comparison of KDIGO with other criteria were not in the scope of the present study.
Conclusion
The aetiology in about half of TAFI patients in coastal Karnataka was malaria. More than 50% develop AKI with greater than one-fifth of them progressing to AKI stage 3 and one-tenth requiring RRT. The most common cause of AKI, AKI stage 2, 3, RRT initiation and in-hospital mortality was leptospirosis. AKI was present in almost all patients with leptospirosis. Therefore leptospirosis is the most nephrotoxic acute febrile illness in the present study population. Dengue fever was the most common cause of AKI stage 1. Vivax malaria was the third most common cause of AKI. The factors like age, presenting complaints, examination findings, renal function and other parameters, aetiology and RRT initiation may be used to predict AKI and in-hospital mortality.
All parameters were significant with p-value <0.01. The positive associations of in-hospital mortality were analysed using Pearson’s chi chi-square test, Mann Whiteney test and Fisher’s exact test as appropriate to the parameters