Moulding Faces at an Early Age-A Case Series
Sunil Sunny1, Rinu Thomas2, Neethu Mathew3, Anvar Kizhakke Parambath4, Amla Madhusudanan5
1 Head of Department and Principal, Department of Orthodontics, Annoor Dental College, Muvattupuzha, Kerala, India.
2 Senior Lecturer, Department of Orthodontics, Annoor Dental College, Muvattupuzha, Kerala, India.
3 Postgraduate Student, Department of Orthodontics, Annoor Dental College, Muvattupuzha, Kerala, India.
4 Postgraduate Student, Department of Orthodontics, Annoor Dental College, Muvattupuzha, Kerala, India.
5 Postgraduate Student, Department of Orthodontics, Annoor Dental College, Muvattupuzha, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rinu Thomas, C/o K.P John, Kannothu House, Kuttapuzha P.O., Thiruvalla-689103, Kerala, India.
E-mail: rinuthomas.t@gmail.com
Certain malocclusions have to be treated at an early age to avoid surgeries for the correction in the future. Introduction of functional appliances has reduced the elimination and correction of skeletal as well as dental discrepancies. Proper case selection taking into consideration skeletal and dental age with the use of various diagnostic aids helps us to identify and treat the malocclusions before it is too late. In this case series, we report three patients with skeletal jaw malrelationship treated with functional and orthopaedic appliances.
Case selection, Functional appliances, Skeletal and dental mal-relationship, Skeletal and dental age
Case Series
In the present case series, cases of three adolescent patients with skeletal and dental malrelationships treated with functional and orthopaedic appliances have been presented.
Case 1
A 12-year-old boy came to the Department of Orthodontics, with the complaint of forwardly placed lower jaw. Extraoral examination showed the patient was a vertical grower with a leptoproscopic face form and a concave profile, intraoral examination revealed that the patient Angle’s Class III malocclusion with reverse over jet on a Class III skeletal jaw base and ectopically erupting upper canines.
Lateral cephalogram, Orthopantomogram, study models and Extraoral and intraoral photographs were made as a part of investigation. Pre-treatment cephalometric analysis indicated maxillary retrognathism and mandibular prognathism with vertical growth pattern. We planned for a treatment with rapid maxillary expansion appliance with reverse pull headgear.
Treatment progress: After three months of treatment, 5mm wide midline diastema was seen after Rapid Maxillary Expansion (RME) and edge to edge bite was achieved. The RME was sealed followed by fixed mechanotherapy [Table/Fig-1,2,3 and 4].
Comparison of pre-treatment and post-treatment cephalometric readings.
| Readings | Normal values | Pre treatment | Post treatment |
|---|
| SNA | 82° | 83° | 83° |
| SNB | 80° | 85° | 81° |
| MPA | 32° | 33° | 33° |
| Gonial angle | 128±7° | 140° | 140° |
| IMPA | 90±3° | 86° | 85° |
| Interincisal angle | 131° | 129° | 132° |
| LAFH | 65.64mm | 63mm | 68mm |
| Co-Gn | 118.95mm | 115mm | 121mm |
Pre-treatment photographs (extraoral and intraoral), lateral cephalogram and orthopantomogram and study models.
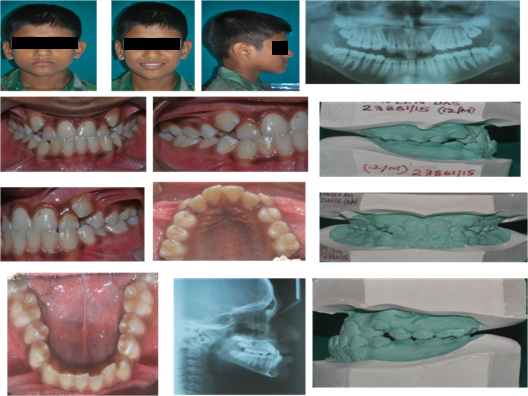
Appliance–Rapid maxillary expander with reverse pull headgear.

Post-treatment photographs (extraoral and intraoral), lateral cepahalogram, orthopantomogram and study models.
Case 2
A 14-year-old girl presented with the chief complaint of forwardly placed upper front teeth. Extra-oral examination showed that the patient was a vertical grower with convex face form.
On intra-oral examination, the patient had Angle’s Class II malocclusion with proclined maxillary and mandibular teeth on skeletal Class II jaw bases.
Necessary pre-treatment records were made. Pre-treatment cephalometric analysis indicated prognathic maxilla and retrognathic mandible with vertical maxillary excess and vertical growth pattern. Treatment planning included activator appliance and high pull headgear for holding the maxilla and forward position of mandible.
Treatment progress: After 11 months of treatment, we attained a Class I molar and Class I canine relation, forward position of mandible and retroclination of upper incisors. Following non extraction line of fixed treatment. Patient had a short lip so planned for cheiloplasty, reduction augmentation genioplasty for deficient chin and gingivectomy to increase the crown height [Table/Fig-5,6,7 and 8].
Comparison of pre-treatment and post-treatment cephalometric readings.
| Readings | Normal values | Pre treatment | Post treatment |
|---|
| SNA | 82° | 82° | 82° |
| SNB | 80° | 77° | 77° |
| MPA | 32° | 32° | 33° |
| Gonial angle | 128±7° | 127° | 128° |
| IMPA | 90±3° | 93° | 97° |
| Interincisal angle | 131° | 114° | 119° |
| LAFH | 65.64mm | 73.5mm | 76.5mm |
| Co-Gn | 118.95mm | 113mm | 117mm |
Pre-treatment photographs (extraoral and intraoral), lateral cepahalogram, orthopantomogram and study models.

Appliance–Activator with high pull headgear.

Post-treatment photographs (extraoral and intraoral), lateral cepahalogram, orthopantomogram and study models.

Case 3
A 12-year-old boy reported with the chief complaint of forwardly placed upper front teeth.
Extra orally the patient was an average grower with convex profile and leptoproscopic face form. Intra-oral examination revealed Angle’s Class II malocclusion with proclined maxillary and mandibular teeth and mandibular anterior crowding on skeletal Class II jaw bases.
Necessary pre-treatment records were made. Pre-treatment cephalometric analysis indicated retrognathic maxilla and mandible with average growth pattern, so we planned for treatment with Frankel Regulator II Appliance.
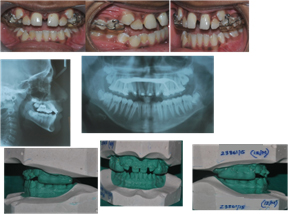
Treatment progress: After 12 months of treatment, we attained Class I molar and Class I canine relation and positional defect and abnormal muscle activity with lip trap has been corrected. We planned for non extraction line of treatment with Interproximal reduction and reduction augmentation genioplasty for chin later [Table/Fig-9,10,11 and 12].
Comparison of pre-treatment and post treatment cephalometric readings.
| Readings | Normal values | Pre treatment | Post treatment |
|---|
| SNA | 82° | 79° | 79° |
| SNB | 80° | 74° | 77° |
| MPA | 32° | 30° | 32° |
| Gonial angle | 128±7° | 121° | 123° |
| IMPA | 90±3° | 93° | 109° |
| Interincisal angle | 131° | 121° | 102° |
| LAFH | 64.33 | 62° | 71° |
| Co-Gn | 114.44 | 108 | 115 |
Pre-treatment photographs (extraoral and intraoral), lateral cepahalogram. orthopantomogram and study models.

Appliance –Frankel Regulator II.

Post-treatment photographs (extraoral and intraoral), lateral cepahalogram and orthopantomogram and study models.

Discussion
Knowledge of normal human growth is essential in recognition of abnormal growth. In general the goal of orthodontic treatment is to improve the patient’s life by enhancing dental and jaw function and dentofacial aesthetics. Chronological age is frequently not enough for evaluating the somatic maturity and developmental stage of the subject, hence the biologic age is evaluated by the skeletal, dental, morphologic age as well as by the onset of puberty [1,2]. The composite of growth changes occurring in the cranial base, maxilla and mandible are necessary to achieve a facial balance. Bjork’s implant studies showed that growth in the suture continues until puberty. It was reported that measurement of the distance of separation between the lateral implants on the frontal cephalogram over time, showed that sutural growth was the most significant factor in the development of the width of the maxilla. Growth in length, on the other hand occurs by sutural growth towards the palatine bone and by apposition at the tuberosities. To formulate the problem list it is important to identify both the patient’s perceptions and the doctor’s observations. This is followed by solutions of these specific problems into a specific treatment strategy that would provide maximum advantage for the patient [3,4]. In our case of RME with reverse pull headgear we have achieved reduction in SNB angle and upper and lower proclination and increase In lower anterior face height and mandibular length which was also observed in animal studies by A.B.M Rabie who demonstrated that anterior positioning of mandible stimulate significant mandibular growth primarily by remodelling process at the condyle. In case of activator with high pull headgear, there was increase in inter-incisal angle with increase in anterior face height and mandibular length and holding of vertically growing maxilla. These functional appliances correct Class II malocclusions by encouraging dentoalveolar change [5,6]. Clinical studies have demonstrated that extra oral force is effective at restricting maxillary horizontal growth [7] as showed in our case. In addition to the orthopaedic effects of headgear, dento-alveolar changes have been reported in a study by Poulton showing majority of correction to the dento-alveolar change. In the case of Frankel regulator, we have achieved reduction in inter-incisal angle and with increase in SNB, lower anterior face height and mandibular length due to downward rotation of mandible. This observation is supported by studies on humans using functional regulator. In a comparative study, Owen concluded that the frankel seems to effect less maxillary retraction than the extra oral force of a headgear [8–10].
Conclusion
Nature does not intend for the orthodontist to achieve perfection rather challenges the orthodontist trying to achieve perfection. Thus, the orthodontist’s task in diagnosis and treatment planning is to ascertain an individual’s available limits of soft tissue to create adaptive dental and skeletal changes. This increased attention to soft tissue and emphasizes on perfection in combination and will better serve the patients in a rational way.
[1]. Samir Bishara, Textbook of Orthodontics 2001 1st edition:33 [Google Scholar]
[2]. Thomas Rakosi, Irmtrud Jonas, Thomas M. Graber, Orthodontic diagnosis colour atlas of dental medicine:102 [Google Scholar]
[3]. Bjork A, Skeiler V, Growth of maxilla in the dimensions as revealed radiographically by the implant methodBr J Orthodontics 1977 4(2):53-64. [Google Scholar]
[4]. William R. Proffit, Henry W. Fields Jr, David M. Sarvar, Contemporary orthodontics4th edition:163 [Google Scholar]
[5]. Rabie A.B.M, Wang L, Tsai M, Replicating mesenchymal cells in the condyle and glenoid fossa during mandibular forward positioningAm J Orthod Dentofacial Orthop 2003 123(1):49-57. [Google Scholar]
[6]. Freunthaller P, Cephalometric observation in class II division 1 malocclusion treated with activatorAngle Orthodontist 1967 37(1):18-25. [Google Scholar]
[7]. Klein PL, An evaluation of cervical traction on the maxilla and upper first permanent molarAngle Orthodontist 1957 27(1):61-68. [Google Scholar]
[8]. Poulton DR, A three year survey of class II malocclusion with and without headgear therapyAngle orthodontist 1964 34(3):181-93. [Google Scholar]
[9]. Righellis EG, Treatment effects of frankel, activator and extraoral traction applianceAngle Orthodontist 1983 53(2):107-21. [Google Scholar]
[10]. Owen AH, Maxillary incisolabial responses in class II division 1 treatment with frankel and edgewiseAngle Orthodontist 1986 56(1):67-87. [Google Scholar]