Cone Beam Computed Tomography- An Effective Tool in Detecting Caries Under Fixed Dental Prostheses
Priyanka Ramesh Vedpathak1, Shailesh Madhukar Gondivkar2, Ajay Ramesh Bhoosreddy3, Karan Rajendra Shah4, Gaurav Ravishankar Verma5, Gayatri Praveen Mehrotra6, Ashwini Chandrakant Nerkar7
1 Postgraduate Student, Department of Oral Medicine and Radiology, MGV’s KBH Dental College and Hospital, Nashik, Maharashtra, India.
2 Assistant Professor, Department of Oral Medicine & Radiology, Government Dental College and Hospital, Nagpur, Maharashtra, India.
3 Professor and Head, Department of Oral Medicine and Radiology, MGV’s KBH Dental College and Hospital, Nashik, Maharashtra, India.
4 Lecturer, Department of Oral Medicine and Radiology, MGV’s KBH Dental College and Hospital, Nashik, Maharashtra, India.
5 Postgraduate Student, Department of Oral Medicine and Radiology, MGV’s KBH Dental College and Hospital, Nashik, Maharashtra, India.
6 Postgraduate Student, Department of Oral Medicine and Radiology, MGV’s KBH Dental College and Hospital, Nashik, Maharashtra, India.
7 Postgraduate Student, Department of Oral Medicine and Radiology, MGV’s KBH Dental College and Hospital, Nashik, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priyanka Ramesh Vedpathak, Vidyanagar (East), Barshi Road, Beed-431122, Maharashtra, India.
E-mail: priyanka.vedpathak09@gmail.com
Introduction
Caries under restorations is the most common reason for re-treatment and replacement in restorative failures. To avoid failures of fixed dental prostheses, it is important to diagnose caries under it earlier. Without image degradation and metal artifacts, Cone Beam Computed Tomography (CBCT) can be the solution to detect caries without removing fixed dental prostheses.
Aim
The aim of this study was to determine the efficacy of CBCT in detecting caries under fixed dental prostheses.
Materials and Methods
Each specimen was scanned with CBCT for evaluation of secondary caries under fixed prostheses. Exposure parameters were 60 kVp and 3mA. Field of View (FOV) used was 8cm X 8cm. According to International Caries Detection and Assessment System (ICDAS) criteria, six Grade 6 carious extracted teeth were selected. All teeth were prepared with four different specimens - full metal, metal-ceramic, full ceramic and metal-acrylic crowns for each tooth. Each specimen was scanned by CBCT. T-test was performed for mean gray value differences between caries and noncaries regions of each material. Gray values were recorded and evaluated for different parameters using two-way analysis of variance.
Results
Significant differences were found with respect to material (full metal, metal-ceramic, full ceramic and metal-acrylic) and situation (caries/noncaries) (p<0.001). There were no significant differences with respect to location (anterior or posterior). Mean gray values of caries and noncaries regions were found to be different for each material.
Conclusion
CBCT can be used as a post-treatment diagnostic technique for detecting caries under fixed prostheses without removing it.
Dentin, Diagnosis, Mean gray value
Introduction
Secondary caries under restorations is the most common reason for re-treatment and replacement in restorative failures [1]. To prevent severe destruction of hard tissue and also to enhance the prognosis for a successful treatment outcome, it is important to diagnose secondary caries earlier [2–4]. For patients with esthetic and functional loss, the treatment of choice is metal crowns and partial Fixed Dental Prostheses (FDP) [5]. The survival rate of FDP is usually of about 10 years and caries is the reason for their failure [6–9]. Even though there are evolution of the materials and techniques used to fabricate fixed restorations, the need to remove them still arises and the most common reason for this is secondary caries [10]. To diagnose secondary caries adjacent to restorations, various radiographic techniques are used such as peri-apical, bitewing, occlusal and panoramic imaging together with clinical examination in order to avoid their failures [11]. Since these radiographic techniques provide only two-dimensional (2D) information, there is a need for three-dimensional (3D) radiographic techniques. For example, if there is any carious lesion located buccally or lingually beneath the restoration, then it would be difficult to detect such conditions using routine 2D radiographic techniques [12]. Another problem with these radiographic techniques is the superimposition of anatomic structures as well as X-rays are notable to penetrate high-atomic-number metals [13,14]. As radiopacity of materials is related to their levels of absorption and scattering of X-rays it has a significant effect on the accuracy of conventional radiographic techniques [15,16]. Most of the metals are radiopaque in conventional X-rays and in most of the radiographic images because of their high electron density making it difficult to diagnose caries at the crown level of abutment teeth with light and dark streaks [17]. These metal artifacts increase in the presence of greater numbers of metal objects and/or units [18]. An artifact is any distortion or error in the image that is unrelated to the subject being studied. Any metallic object if present in scanned area can produce artifact due to distortion of metallic structure [19]. The scanned high density object absorbs more low-energy photons than high-energy photons, which is called beam hardening. Cupping, hypodense halo and streaks are the most commonly occurring artifacts which are produced because of beam hardening.
CBCT is a promising radiographic technique which enables clinicians to evaluate the region of interest in three planes, axial, coronal and sagittal. Advantage of CBCT over medical CT is reduced radiation dose and reduced cost [20]. CBCT uses a cone shaped X-ray beam centered on a 2D sensor to scan a 180°-360° rotation around the patient’s head to acquire a full 3D volume of data. As per the need of today’s practitioners’, various materials are used for fixed prostheses such as porcelain-fused-to-metal, full metal and full ceramic which differ according to the properties of the biomaterials as well as the processing of the products [21,22]. In this study, CBCT was used to detect caries under FDP of full metal, metal ceramic, full ceramic and metal acrylic. Because of the difficulties in detection of caries under fixed restorations due to the compression of structures in intraoral radiography and metal artifacts in CBCT, the aim of this study was to determine the efficacy of CBCT in detecting caries under fixed dental prostheses.
Materials and Methods
This in-vitro study was conducted at the Department of Oral Medicine and Radiology, MGV’s KBH Dental College and Hospital, Nashik, India from October 2015 to December 2015. According to International Caries Detection and Assessment System (ICDAS) criteria [Table/Fig-1] [23], inclusion criteria of the study was six extracted carious permanent teeth (Tooth no. 11, 12, 23, 16, 26, 47) with Grade 6 caries that extended to dentin and the pulp cavity and cavity walls all along the cervical, middle and occlusal third of the crown. All the selected teeth were without any restoration and got extracted because of extensive caries and mobility. Extracted teeth were then cleaned and kept in distilled water for 24 hours at 37°C. During teeth preparation, the caries cavity was filled with wax to a level in line with the preparation outline making it a full crown structure [Table/Fig-2]. Impression was taken with a silicon impression material and sent to a technician to fabricate a crown of full metal, metal ceramic, full ceramic and metal acrylic materials. From the caries cavity, the wax was removed by using hot water. A total of five crown specimens were obtained: One full metal (16), One metal ceramic (12), One full ceramic (11), One metal acrylic (47) and Two prepared teeth, One anterior (23) and One posterior (26) without any restorations as the control group [Table/Fig-3]. We inserted the cast with all crown specimens into water in order to imitate oral soft tissues. Each specimen was then scanned with CBCT for evaluation of the secondary caries under fixed prostheses. Orthophos XG model of Sirona CBCT machine was used for this study. 3D Exposure parameters were 60 kVp and 3mA. Field of View (FOV) used was 8cm X 8cm with 1mm slice thickness and exposure time of 14 seconds. Tube potential and tube current were automatically determined from scout views by the CBCT machine. The CBCT images of the specimens were reconstructed with Galileos Software [Table/Fig-4]. Two specialized oral and maxillofacial radiologists separately evaluated the cross-sectional images on axial, coronal and tangential slices. The ability of CBCT imaging to display differences in attenuation is related to the ability of the detector to reveal subtle contrast differences. This parameter is called the bit depth of the system and determines the number of shades of gray available to display the attenuation [19]. All gray values of caries and dentin were recorded from axial, coronal and tangential slices. The mean of these three gray values of caries and dentin was then calculated respectively for each image and considered as Mean Gray Value (MGV) at that site. All the obtained data was collected, tabulated and entered in MS excel and analyzed by using SPSS version 20.0.0 software. Pearson’s correlation was used to assess inter-examiner reliability. Two-way ANOVA was used for statistical analysis. Independent sample t test was done for individual evaluation of caries and dentin differences.
International Caries Detection and Assessment System (ICDAS).
| Code | Description | Pictorial Presentation |
|---|
| 0 | Sound tooth surfaces |  |
| 1 | First visual change in enamel |  |
| 2 | Distinct visual change in enamel |  |
| 3 | Initial breakdown in enamel due to caries with no visible dentin |  |
| 4 | Surface with underlying dark shadow from dentin |  |
| 5 | Distinct cavity with visible dentin |  |
| 6 | Extensive distinct cavity with visible dentin |  |
The caries cavity was filled with wax making it a full crown structure.

A cast with crowns of full metal, metal ceramic, full ceramic and metal acrylic materials.

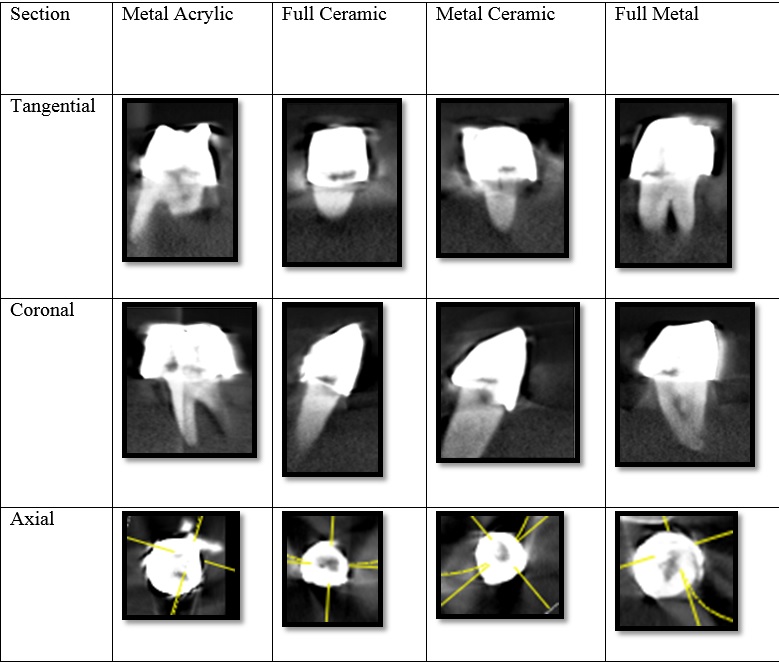
Cross sectional images of tangential, coronal and axial slices.
Results
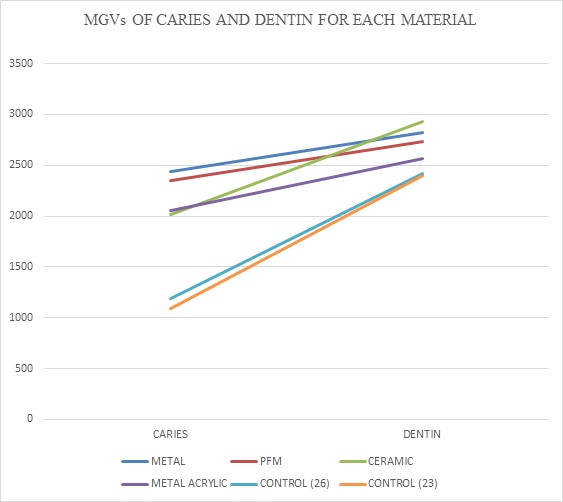
MGVs of caries versus healthy dentin of control group i.e. 23 and 26 were 1089 ± 129.8 versus 2397.5 ± 118.13 of caries and 1193 ± 131.91 versus 2415.7 ± 120.27 of dentin respectively. MGVs of caries of full metal, metal ceramic, full ceramic and metal acrylic are 2440 ± 207.25, 2352.7 ± 249.04, 2012 ± 216.64 and 2055 ± 84.113 respectively. MGVs of healthy dentin of full metal, metal ceramic, full ceramic and metal acrylic are 2820.3 ± 125.94, 2731 ± 174.07, 2933.7 ± 93.388 and 2568.7 ± 169.19 respectively. Means and standard deviations of MGVs are listed in [Table/Fig-5].
Mean gray values of the material tested for caries and dentin.
| MATERIAL | CARIES | DENTIN |
|---|
| Full Metal | 2440 ± 207.25 | 2820.3 ± 125.94* |
| Metal Ceramic | 2352.7 ± 249.04 | 2731 ± 174.07* |
| Full Ceramic | 2012 ± 216.64 | 2933.7 ± 93.388* |
| Metal Acrylic | 2055 ± 84.113 | 2568.7 ± 169.19* |
| Control (23) | 1089 ± 129.8 | 2397.5 ± 118.13* |
| Control (26) | 1193 ± 131.91 | 2415.7 ± 120.27* |
Independent sample t test
*Statistically significant difference at p < 0.05
Two-way analysis of variance showed significant differences with respect to material (full metal, metal ceramic, full ceramic, metal acrylic) (p < 0.001); and situation (caries or noncaries) (p < 0.007), whereas no significant difference was found with respect to location (anterior/posterior) [Table/Fig-6]. MGVs for caries and healthy dentin regions were found to differ significantly between four different materials (p < 0.001) [Table/Fig-7].
Two-way analysis of variance for different parameters.
| PARAMETERS | SUM OF SQUARES | df | MEAN SQUARE | F | p-value |
|---|
| Anterior/ Posterior | 9004.8 | 2 | 4502.4 | 3.814 | 0.1901 |
| Metal/PFM/ Ceramic/ Metal Acrylic | 409158 | 3 | 136386 | 25.299 | 0.0012 |
| Caries/Dentin | 35467 | 2 | 17734 | 3.174 | 0.0079 |
a) Metal - full metal, b) PFM - porcelain fused to metal (metal ceramic), c) Ceramic - full ceramic
Mean gray values of caries and dentin for each material.
a) Metal - full metal, b) PFM - porcelain fused to metal (metal ceramic), c) Ceramic - full ceramic
Discussion
There are very few scientific researches on the detection of different types of caries at different levels beneath different types of FDP using CBCT. In this study, we assessed teeth with full metal, metal ceramic, full ceramic, metal acrylic and compared with teeth without restorations at different levels and for different types of caries. In a previous study, researchers evaluated the caries under a single crown of lithium disilicate ceramic crown, zirconia ceramic crown, and metal ceramic crown using CBCT and determined significant differences between the caries and dentin images [5]. In the present study, we increased the numbers of specimens i.e., we used four different specimens of full metal, metal ceramic, full ceramic and metal acrylic in order to increase the sensitivity of the data. Even with the increased numbers and different types of specimens, the results were found to be similar to the findings of Bilgin et al., [5]. Murat et al., [11] made standardized artificial carious lesions instead of using natural carious teeth. They prepared specimens to imitate caries cavitation at the cervical third under various types of restorations of composite resin, amalgam, complete metal crown, and thermoplastic polymer. They assessed the performance of intraoral film and digital radiography and two different CBCT systems for the visibility of artificial buccal recurrent caries lesions under various restorative materials. They found that CBCT outperformed intraoral radiography in detection of artificial buccal recurrent caries under restorations. In the present study, extracted teeth with ICDAS Grade 6 caries that extended to dentin, including the pulp cavity and cavity walls all along the cervical, middle, and occlusal third of the crown were used and we evaluated caries detection under the four different crown systems using CBCT. Nummikoski et al., observed that the radiopacity of restorative materials, which depends on the atomic number, has a primary effect on the ability to detect caries in the cervical zone [16]. The present study showed that, with advanced digital radiographic techniques, the middle portion of the tooth under a fixed restoration could be diagnosed in addition to the cervical zone. As the number of metal restorations in the oral cavity increases, metal artifacts and image degradation (as light streaks) increases [11,18]. However, although metal restorations hinder the visualization of caries under fixed restorations, the present study showed that caries under all four types of restorations can be detected and characterized. Many authors described that radiopacity of the restorative materials aids in detection of caries in cervical zone. This radiopacity is associated with atomic number of the material. However, the high atomic number leads to degrade the image [11,16,18]. Thus it has been suggested that by reducing field size or modifying the patient position would help to avoid the scanning region susceptible to beam hardening [24–27]. In this study, we used small FOV i.e., 8cm X 8cm which in turn avoided the chances of metal artifacts. Our study also indicates that with the help of CBCT with smaller FOV, it would be possible to detect even middle and cervical portion of tooth beneath fixed dental prosthesis.
Limitation
One of the limitations of this study was that only a single crown unit was evaluated for CBCT diagnosis. Future studies should be undertaken to evaluate CBCT for the detection of caries by using a greater number of metal units. Another limitation was that the specimens were not fixed using luting cement, which can also affect radiopacity. This should motivate other researchers to review previous CBCT scans in order to determine the possibility of detecting caries with FDPs under different conditions.
Conclusion
CBCT enables the detection of ICDAS Grade 6 caries under the crowns of all four materials investigated. Ceramic crowns allowed more effective detection of secondary caries as compared to other three materials. The radiopacity of the restorative material have a significant effect on accuracy with conventional but not with advanced three dimensional radiographic techniques. Efforts are needed to improve CBCT reconstruction algorithms, with a target on reducing artifacts induced by dense dental materials so that we can get an enhanced image quality at low radiation doses. CBCT scans taken for other reasons can be used as a post-treatment diagnostic technique for detecting caries under fixed dental prostheses. Since the routine 2D radiographic techniques cannot detect caries under fixed metallic dental prostheses, there is a need for CBCT (3D) radiographic techniques to detect such carious lesions. Moreover, it is a solution for diagnosing secondary caries without the removal of fixed prosthesis. Also chances of tooth fracture during fixed dental prosthesis removal can be avoided with less discomfort to patients. Further studies should be carried out to evaluate caries lower than ICDAS Grade 6 along with larger sample size and multiple unit prostheses.
Independent sample t test
*Statistically significant difference at p < 0.05
a) Metal - full metal, b) PFM - porcelain fused to metal (metal ceramic), c) Ceramic - full ceramic
[1]. Mamai-Homata E, Margaritis V, Koletsi-Kounari H, Oulis C, Polychronopoulou A, Topitsoglou V, Tooth loss and oral rehabilitation in Greek middle-aged adults and senior citizensInt J Prosthodont 2012 25:173-79. [Google Scholar]
[2]. Arnold WH, Sonkol T, Zoellner A, Gaengler P, Comparative study of in vitro caries-like lesions and natural caries lesions at crown marginsJr Prosthodont 2007 16(6):445-51. [Google Scholar]
[3]. Ando M, Gonzalez-Cabezas C, Isaacs RL, Eckert GJ, Stookey GK, Evaluation of several techniques for the detection of secondary caries adjacent to amalgam restorationsCaries Research 2004 38(4):350-56. [Google Scholar]
[4]. Okida RC, Mandarino F, Sundfeld RH, de Alexandre RS, Sundefeld ML, In vitro evaluation of secondary caries formation around restorationBulletin of Tokyo Dental College 2008 49(3):121-28. [Google Scholar]
[5]. Bilgin MS, Aglarci OS, Erdem A, Post-treatment diagnosis of caries under fixed restorations: A pilot studyJ Prosthet Dent 2014 112:1364-69. [Google Scholar]
[6]. Lemke HUVM, Inamuson K, Farman A, CARS ’98 Computer Assisted Radiology and Surgery 2007 AmsterdamElsevier:792-797. [Google Scholar]
[7]. Tan K, Pjetursson BE, Lang NP, Chan ES, A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 yearsClin Oral Implants Res 2004 15:654-66. [Google Scholar]
[8]. Creugers NH, Kayser AF, van’t Hof MA, A meta-analysis of durability data on conventional fixed bridgesCommunity Dent Oral Epidemiol 1994 22:448-52. [Google Scholar]
[9]. Scurria MS, Bader JD, Shugars DA, Meta-analysis of fixed partial denture survival: Prostheses and abutmentsJ Prosthet Dent 1998 79:459-64. [Google Scholar]
[10]. Sharma A, Rahul GR, Poduval ST, Shetty K, Removal of failed crown and bridgeJ Clin Exp Dent 2012 4:167-72. [Google Scholar]
[11]. Murat S, Kamburoglu K, Isayev A, Kursun S, Yuksel S, Visibility of artificial buccal recurrent caries under restorations using different radiographic techniquesOper Dent 2013 38:197-207. [Google Scholar]
[12]. Kandemir S, The radiographic investigation of the visibility of secondary caries adjacent to the gingiva in Class II amalgam restorationsQuintessence International 1997 28(6):387-92. [Google Scholar]
[13]. Farman AG, Farman TT, A comparison of 18 different X-ray detectors currently used in dentistryOral Surg Oral Med Oral Pathol Oral Radiology Endod 2005 99:485-89. [Google Scholar]
[14]. Kamburoglu K, Ilker Cebeci AR, Grondahl HG, Effectiveness of limited cone-beam computed tomography in the detection of horizontal root fractureDent Traumatol 2009 25:256-61. [Google Scholar]
[15]. Okuda Y, Noda M, Kono H, Miyamoto M, Sato H, Ban S, Radio-opacity of core materials for all-ceramic restorationsDent Mater J 2010 29:35-40. [Google Scholar]
[16]. Nummikoski PV, Martinez TS, Matteson SR, McDavid WD, Dove SB, Digital subtraction radiography in artificial recurrent caries detectionDentomaxillofac Radiol 1992 21:59-64. [Google Scholar]
[17]. Chandler HH, Bowen RL, Paffenbarger GC, Physical properties of a radiopaque denture base materialJ Biomed Mater Res 1971 5:335-57. [Google Scholar]
[18]. Tohnak S, Mehnert AJ, Mahoney M, Crozier S, Dental CT metal artifact reduction based on sequential substitutionDentomaxillofac Radiol 2011 40:184-90. [Google Scholar]
[19]. White SC, Pharoah MJ, Oral radiologyPrinciples and interpretation 2014 7th edSt. Louis MissouriMosby:187-91. [Google Scholar]
[20]. Schulze RK, Berndt D, d’Hoedt B, On cone-beam computed tomography artifacts induced by titanium implantsClin Oral Implants Res 2010 21:100-07. [Google Scholar]
[21]. Esmaeili F, Johari M, Haddadi P, Vatankhah M, Beam hardening artifacts: Comparison between two cone beam computed tomography scannersJ Dent Res Dent Clin Dent Prospects 2012 6:49-53. [Google Scholar]
[22]. Vasconcelos KF, Nicolielo LF, Nascimento MC, Haiter Neto F, Boscolo FN, Van Dessel J, Artifact expression associated with several cone-beam computed tomographic machines when imaging root filled teethInt Endod J 2015 48(10):994-1000. [Google Scholar]
[23]. Ismail AI, Sohn W, Tellez M, Willem JM, Betz J, Lepkowski J, Risk indicators for dental caries using the International Caries Detection and Assessment System (ICDAS)Community Dent Oral Epidemiol 2008 36:55-68. [Google Scholar]
[24]. Abramovitch K, Rice DD, Basic principles of cone beam computed tomographyDent Clin North Am 2014 58:463-84. [Google Scholar]
[25]. White SC, Cone beam imaging in dentistryHealth Physics 2008 95(5):628-37. [Google Scholar]
[26]. Wassell RW, Walls AW, Steele JG, Crowns and extra-coronal restorations: Materials selectionBr Dent J 2002 192(199-202):205-211. [Google Scholar]
[27]. Höland W, Schweiger M, Watzke R, Peschke A, Kappert H, Ceramics as biomaterials for dental restorationExpert Rev Med Devices 2008 5:729-45. [Google Scholar]