Now-a-days day care surgeries are becoming popular. Anaesthesia for these surgeries is also very important. For short procedures like endoscopic procedures, incision and drainage, debridement, laparoscopic ligation, we need a short acting agent which is defined in its work and besides being a good sedative and anxiolytic, is also having strong analgesic property. Ketamine, which is a dissociative anaesthetic, is having all the properties which we needed i.e. an intravenous anesthetic with distinct analgesic activity and relatively rapid onset of action with immediate recovery. It has bronchodilatory property which is very useful during intraoperative period. The precise molecular mechanism of ketamine has been extensively studied during the last decade and the current understanding is that inhibition of sensory perception is mediated by the blockade of N-methyl D-aspartate receptor blockade [1]. The main drawback of use of Ketamine for these short procedures is postoperative delirium, excitement and hallucinations which is called the emergent reactions of Ketamine. Cardiostimulatory responses after Ketamine induction are also possible. Although, Ketamine is widely used, but these properties have limited its use as general anaesthetic. However, the emergent reactions like unpleasant dreams or hallucination can be overcome by use of benzodiazepines as premedication [2,3]. Dexmedetomidine due to its anxiolytic, sedative, analgesic, anaesthetic sparing and neuroprotective effect, has now become commonly used drug in anaesthesia practice. It maintains sympathoadrenal stability and perioperative haemodynamics. These properties suggest that it can be suitable adjuvant to Ketamine anaesthesia [4–7].
The aim of our study was to compare the effect of Dexemedtomidine or Midazolam as premedication for surgery under Ketamine anaesthesia. This study was proposed to compare the effects of dexmedetomidine and midazolam when used as premedicating agent with ketamine. We assessed Postoperatve delirium, intraoperative haemodynamic stability and Postoperative pain.
Materials and Methods
A prospective, randomized and double-blind study was conducted after approval from institutional ethical committee and written informed consent, on from patients of ASA (American Society of Anaesthesiology) class I and class II, aged between 18 to 40 years and of both sexes undergoing various short surgical procedures in the hospital from October 2014 to September 2015 at Department of Anaesthesia in Rama Medical College, Mandhana, Kanpur, Uttar Pradesh, India. Patients who were included in the study were randomly divided into three groups using computer generated table of random numbers. Detailed pre anaesthetic check-up of every patient was done. Delirium scoring was done pre operatively with help of Memorial Delerium Assessment Scale.
The patients were inserted intravenous cannula into a peripheral vein and i.v. drip started. Patients were pre medicated with inj. Ranitidine (0.25mg/kg), inj. Metoclopramide (0.15mg/kg) and inj. Glycopyrrolate (0.01mg/kg). Patients were pre oxygenated with help of Hudson mask with oxygen flow of 6 L/min.
According to the group alloted, the study solution was prepared in a separate OT so that the assessor and the patient both were unaware to the constituent of the study solution. Assessors were also blinded to the computer generated randomization.
Group K: Patients were pre medicated with normal saline 10 ml as placebo, given slowly over 10 minutes, anaesthesia induced with inj. Ketamine 2mg/kg.
Group M: Patients were pre medicated with inj. Midazolam 0.05mg/kg diluted to 10ml with normal saline, given slowly over 10 minutes, anaesthesia induced with inj. Ketamine 2mg/kg.
Group D: Patients were pre medicated with inj. Dexmedetomidine 0.5μg/kg diluted to 10ml with normal saline, given slowly over 10 minutes, anaesthesia induced with inj. Ketamine 2mg/kg.
Group K patients were considered as Control Group. Although, Ketamine known to cause delirium, but we avoid any sedative premedication in this group because surgical procedure in present study are of short duration (10-15min) and simultaneously if patient experiencing delirium score approaching to 15, we gave inj. Midazolam 0.05mg/kg and excluded them from the study.
Anaesthesia was induced only after the surgeon was ready and painting and draping of incision site has been done. Oxygenation continued with help of Hudson mask at oxygen flow of 6 L/min. During the whole procedure, continuous monitoring was done for Pulse Rate (PR), Non Invasive Blood Pressure (NIBP) and ECG with help of multipara monitor. Postoperative Pulse Rate and Mean Blood Pressure values are taken after shifting of the patient to postoperative room. Postoperative delirium scoring was done after 30 min of giving inj. Ketamine and postoperative pain scoring was done after 60 min of giving inj. Ketamine. In this study we have used an objective scale for measuring delirium pre operatively and Postoperatively. We used Memorial Delirium Assessment Scale (MDAS) for scoring of delirium [8]. For scoring of postoperative pain we have used VAS numeric pain distress scale [9]. Surgical procedures which took more than 15 min in completion or in which other sedative agents have to be used were excluded from the study to prevent any confounding effect of other agents on delirium caused by ketamine.
Statistical Analysis
All statistical analyses were performed using MedCalc version 12-© 1993-2013 statistical software. Demographic data were compared using Student’s unpaired t-test. The monitored and calculated data were analysed using one-way Analysis Of Variance (ANOVA). For all paired comparisons, test applied was Tukey-Kramer test.
Results
There was no statistically significant difference among the groups in terms of age, weight, height and sex [Table/Fig-1].
| Group K | Group M | Group D |
|---|
| Age (yrs) | 29.1 ± 6.8297 | 30.56 ± 7.0987 | 30.96 ± 6.6824 |
| Weight (Kg) | 60.06 ± 9.2473 | 60.63 ± 10.3907 | 61.56 ± 10.0823 |
| Height (cm) | 158.95 ± 8.7652 | 158.38 ± 7.4938 | 160.40 ± 8.3517 |
| Gender M/F | 11/19 | 11/19 | 10/20 |
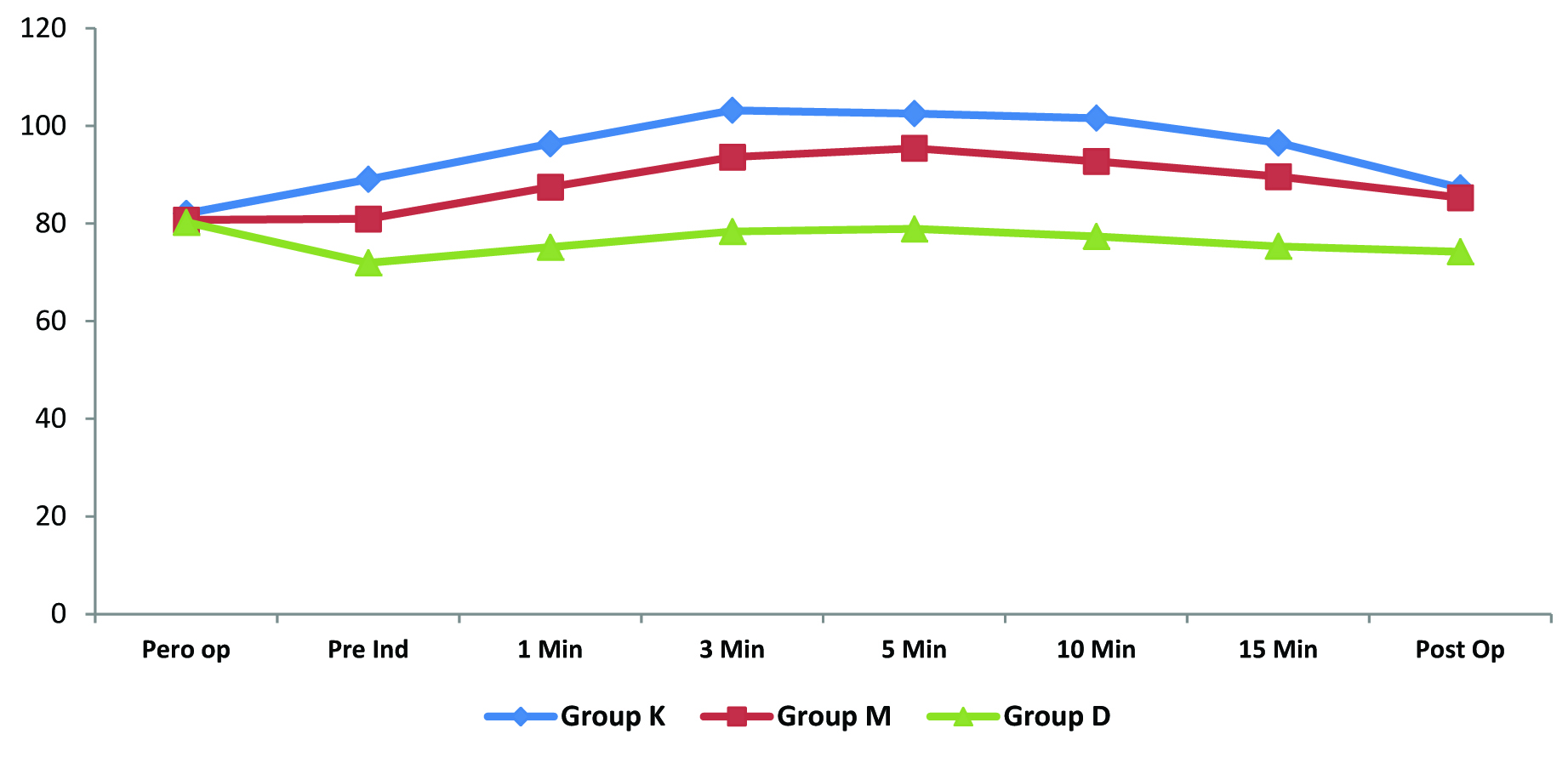
Data shows that in comparison to control group, midazolam and Dexmedetomidine both produced more haemodynamically stable patients. But group D (Dexmedetomidine) patients were even more haemodynamically stable in comparison to group M patients. Pulse rate findings among three groups shows that Dexmedetomidine reduced pulse rate significantly (p-value<0.001) [Table/Fig-2]. We have compared Pulse Rate values in all three groups in graphical form [Table/Fig-3].
Haemodynamic variables: pulse rate.
| Time | Group K | Group M | Group D | p-value |
|---|
| Mean | SD | Mean | SD | Mean | SD |
|---|
| Pre operative | 82.06 | 9.607 | 80.73 | 9.259 | 80.26 | 5.214 | 0.785 |
| Pre induction | 89.06 | 8.766 | 80.93 | 6.312 | 71.93 | 6.329 | <0.001 |
| 1 min | 96.37 | 4.718 | 87.47 | 5.721 | 75.13 | 13.214 | <0.001 |
| 3 min | 103.2 | 9.124 | 93.6 | 4.428 | 78.36 | 8.271 | <0.001 |
| 5 min | 102.53 | 11.546 | 95.40 | 13.212 | 78.90 | 8.766 | <0.001 |
| 10 min | 101.6 | 9.217 | 92.73 | 6.231 | 77.36 | 8.124 | <0.001 |
| 15 min | 96.53 | 11.914 | 89.63 | 8.756 | 75.33 | 12.392 | <0.001 |
| Postoperative | 87.3 | 6.565 | 85.3 | 9.231 | 74.23 | 10.751 | <0.001 |
Comparison of pulse rate in three groups.
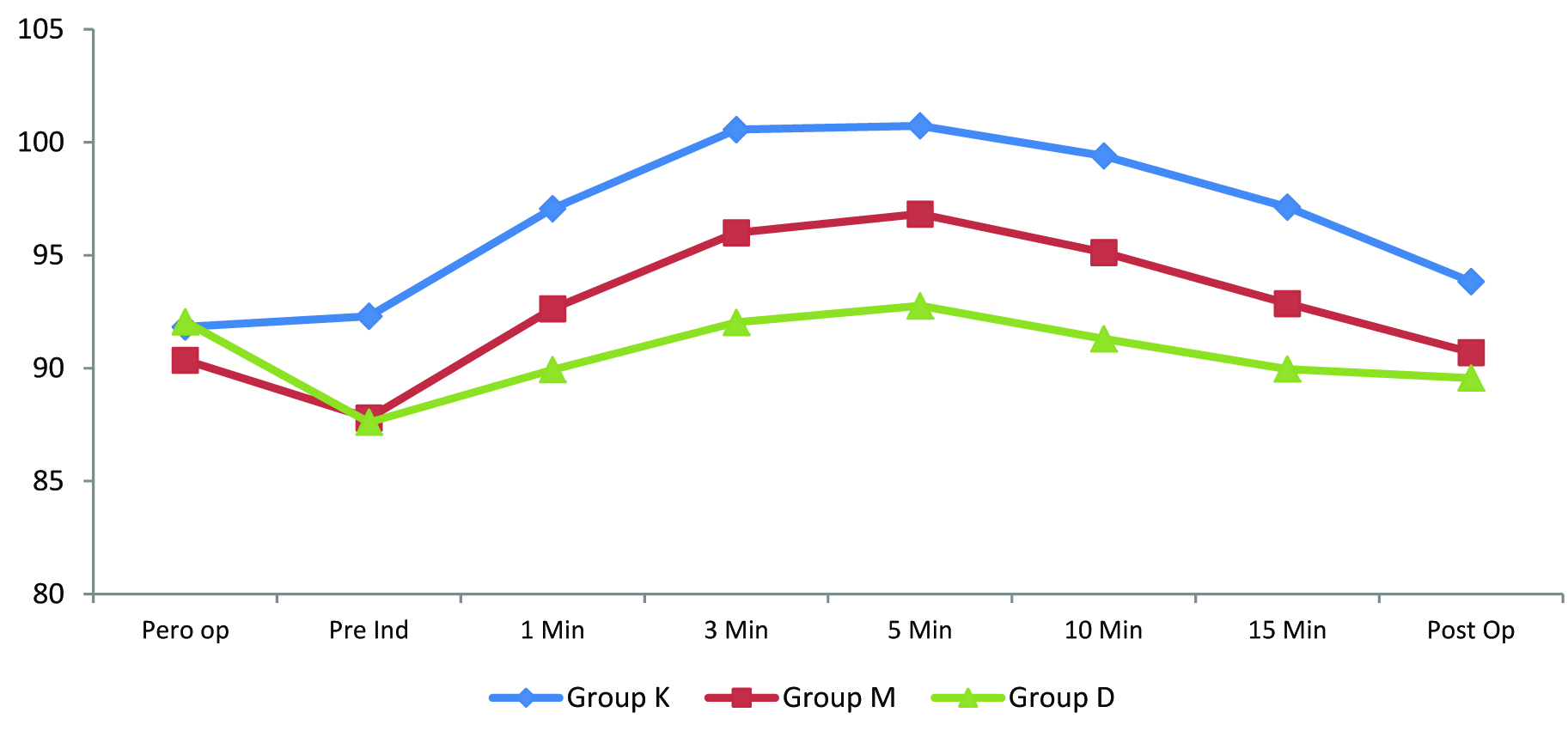
Dexmedetomidine reduced Mean Blood Pressure also to a highly significant level (p-value<0.001) in early intraoperative period. In group D and group M, there was fall in mean blood pressure in pre induction period. After giving inj ketamine, MBP again increased in group M and group D patients, but it was to a lesser extent in Dexmedetomidine group in comparison to midazolam group. Mean Blood Pressure values were significant (p-value<0.05) in Postoperative period also [Table/Fig-4]. We have compared Mean Blood Pressure values in all three groups in graphical form [Table/Fig-5]. No patient developed bradycardia or hypotension, and SpO2 was maintained more than 95% in all the patients throughout the observation.
Haemodynamic variables: mean blood pressure.
| Time | Group K | Group M | Group D | p-value |
|---|
| Mean | SD | Mean | SD | Mean | SD |
|---|
| Pre operative | 91.83 | 11.614 | 90.37 | 15.013 | 92.07 | 8.715 | 0.426 |
| Pre induction | 92.30 | 12.231 | 87.80 | 15.419 | 87.60 | 9.257 | <0.001 |
| 1 min | 97.07 | 12.452 | 92.63 | 13.769 | 89.93 | 11.545 | <0.001 |
| 3 min | 100.56 | 15.248 | 96.00 | 12.253 | 92.03 | 9.755 | <0.05 |
| 5 min | 100.73 | 9.127 | 96.83 | 11.176 | 92.76 | 8.769 | <0.05 |
| 10 min | 99.45 | 11.231 | 95.13 | 9.751 | 91.30 | 10.625 | <0.05 |
| 15 min | 97.13 | 10.124 | 92.86 | 8.679 | 89.86 | 13.451 | <0.05 |
| Postoperative | 93.88 | 14.271 | 90.70 | 9.217 | 89.56 | 12.712 | <0.05 |
Comparison of mean blood pressure in three groups.
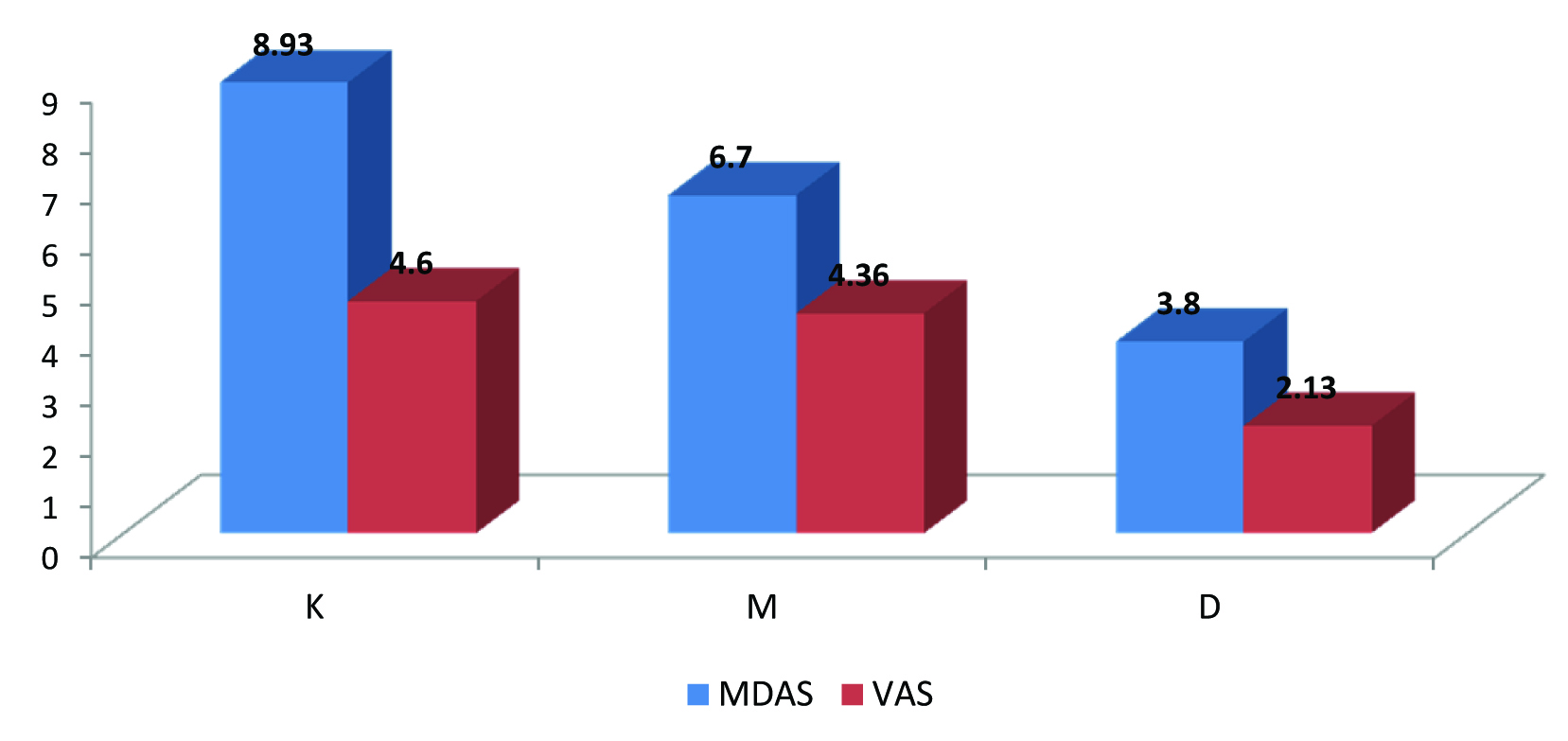
Midazolam reduced delirium to a greater level, but in comparison to control group and midazolam group, Dexmedetomidine reduced delirium to a much great level. (p-value<0.001). For Group K, MDAS Score was 8.93±1.45. For Group M, it was 6.7±1.1 and for Group D, it was 3.8±0.54 [Table/Fig-6]. Postoperative pain was less in Dexmedetomidine group. For Group K, VAS Score was 4.6±0.41and for Group M, it was 4.36±0.38 which was comparable but for Group D, VAS Score was 2.13±0.31 which was highly significant (p-value< 0.001) [Table/Fig-6].
Delerium and pain score variables.
Discussion
In day to day practice there are a lot of short surgical procedures for which patients are posted in O.T. Many patients do not prefer local anaesthesia for these procedures and in the same time, they do not want any pain or bad memories. So a short acting anaesthetic agent having properties like amnesia and analgesia is needed. Because general anaesthesia is much time consuming for these types of cases as duration of procedure is very short and no. of cases posted is high. This study was conducted to compare the effect of Dexmedetomidine and Midazolam when used as premedicating agent with Ketamine. As Ketamine is associated with emergent reactions like delirium and hallucination, so the aim of current study was to see the effects of Dexmedetomidine and Midazolam on delirium caused by Ketamine.
Our study showed significant difference in HR and MBP in Group D when compared to Group K and Group M. Group D had significantly lower HR and MBP (p-value<0.001) [Table/Fig-2,4]. These results are in accordance with previous studies by Murat Gündüz et al., [10]. They compared the effects of ketamine, ketamine-dexmedetomidine and ketamine-midazolam on dressing changes of burn patients. These findings suggest that Dexmedetomidine has clinical advantages over midazolam with regard to controlling haemodynamic variability.
But study of Mohamed A. Daabiss and Mohamed Hashish differ from our view [11]. Their study compared the efficacy of oral Dexmedetomidine and oral ketamine-midazolam as pre-anaesthetic in paediatric patients (2-6 yrs). Results show that oral ketamine-midazolam causes better haemodynamic stability and higher degree of parental satisfaction and appears to be superior anxiolytic and hypnotic. This difference in result may be due to different age group of patients and different route of administration.
Walker et al., stated that no respiratory depression is associated with the use of Dexmedetomidine [12]. Similarly, in a recent study, Taghinia et al., reported that Dexmedetomidine decreased the frequency of oxygen desaturation and reduced the amounts of narcotic and anxiolytic requirement [13]. These results are in accordance with present study. We did not observe any respiratory depression, hypoxia or apnea in any group. The most frequently seen adverse effects of IV Dexmedetomidine that have been reported are hypotension and bradycardia. In this study, only a brief episode of hypotension (SBP, 60 mm Hg) was observed in a 23-year-old male patient who had received ketamine-dexmedetomidine combination, and it was treated mainly with inj ephedrine 10mg bolus and IV fluid (0.9% saline 5-10 mL kg-1h-1) administration.
The delirium scoring was done according to the “Memorial Delerium Assessment Scale” as published in an article by Breitbart W et al., in journal of pain symptom manage [8]. Minimum score is zero (0) which is “no delirium”. This was the score for all of the patient’s pre operatively. Maximum score is 15 which is “severe grade of delirium”. Previous study by Levanen J et al., used DSST (Digital Symbol Substitution Test) to quantitate psychomotor performance which was very complex [14]. Our scoring method is easier and based on 10 items which include consciousness, disorientation, short term memory impairment, impaired digit span, ability to maintain and shift attention, disorganized thinking, perceptual disturbances, delusions, psychomotor activity and sleep wake cycle disturbances. First five items are used in our study to assess acute delirium. The results of our study [Table/Fig-6] are in accordance with the study by Levanen J et al., that is Dexmedetomidine induced significantly less psychomotor impairment and delirium in comparison to midazolam (p-value<0.001) [14]. But in study by Mohamed A. Daabiss and Mohamed Hashis, emergence from anaesthesia was comparable between two groups [11]. This difference may be due to the fact that this study has been done in different age group of patients.
Our study showed that Postoperative pain was significantly less in Group D in comparison to Group K and Group M. (p-value<0.001) [Table/Fig-6]. These results are in accordance with previous study by Levänen J et al., [14] But the study of Murat Gündüz et al., conducted on burn patients, showed no significant difference in pain scores with use of dexmedetomidine and midazolam [10]. This difference in result may be due to the fact that the study was done in burn patients and the pain threshold of burn patients is less [15].
Limitation
The present study has been done for short procedures like laparoscopic ligation, debridement, cyst removal, etc. No long duration surgeries were included in the study. Only short term effects of anaestheic drug have been studied.
Conclusion
Current study shows that Dexmedetomidine can be a good alternative to Benzodiazepines as pre medicating agent with Ketamine in short duration surgeries. Dexmedetomidine can reduce delirium caused by Ketamine more effectively than Midazolam. It provides excellent haemodynamic stability in intraoperative and postoperative period. It also complements analgesia caused by Ketamine.