The Hormonal Fingerprints and BMI: Implications for Risk Factors in Dental Caries and Malocclusion
Goguladinne Naga Deepthi Priyanka1, Madu Ghanashyam Prasad2, Ambati Naga Radhakrishna3, Juvva Ramakrishna4, Velagapudi Jyothi5
1 Postgraduate Student, Department of Pedodontics and Preventive Dentistry, St. Joseph Dental College, Eluru, Andhra Pradesh, India.
2 Professor and Head, Department of Pedodontics and Preventive Dentistry, St. Joseph Dental College, Eluru, Andhra Pradesh, India.
3 Reader, Department of Pedodontics and Preventive Dentistry, St. Joseph Dental College, Eluru, Andhra Pradesh, India.
4 Postgraduate Student, Department of Pedodontics and Preventive Dentistry, St. Joseph Dental College, Eluru, Andhra Pradesh, India.
5 Senior Lecturer, Department of Pedodontics and Preventive Dentistry, St. Joseph Dental College, Eluru, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Madu Ghanashyam Prasad, Professor and Head, Department of Pedodontics and Preventive Dentistry, St. Joseph Dental College, Duggirala, Eluru, Andhra Pradesh, India.
E-mail: drghanasyam@gmail.com
Introduction
The hormonal fingerprint is the ratio between 2nd and 4th digit lengths. It was evidenced in the medical scenario that it can be used as an indirect marker in many diseases like Coronary Heart Disease (CHD) and metabolic syndromes. As far as dentistry is concerned very few studies in the literature have been done to evaluate the influence of hormonal fingerprint on oral health, thus provoking us to formulate new method for predicting dental caries and malocclusion and its association with Body Mass Index (BMI).
Aim
The purpose of this retrospective study was to highlight the role of new biological marker–Hormonal fingerprints in the early detection of malocclusion, caries, the influence of BMI on malocclusion and caries. We also attempted to study the correlation of BMI with hormonal fingerprints.
Materials and Methods
A total of 300 children were randomly selected from both sexes of age group 10-15 years. The hormonal fingerprint was made by measuring the length ratio of the index and ring finger with the help of digital Vernier caliper. Anthropometric measures (weight in kilograms and height in metres) for the calculation of BMI were recorded. Caries assessment was done using standard mouth mirrors and Community Periodontal Index probes. DMFT index was followed for assessment of caries according to the WHO assessment form, 1997. Occlusal characteristics of the children evaluated were molar relation, anterior and posterior cross bite, open bite, deep bite, lower anterior crowding. All the factors were recorded by two investigators.
Results
The results of the study showed that majority of the children among study population were having 2D:4D <1. The rate of occurrence of malocclusion was increasing with increase in the value of 2D:4D ratio with a statistically significant p-value of <0.001. Higher BMI values were associated with normal occlusal conditions (p= 0.041) and lower 2D:4D ratio (p= 0.037). High caries experience was noticed in children with malocclusion (p= 0.027) which further influences the caries susceptibility. Pearson’s correlation test, t-test and ANOVA were used in the study for statistical analysis using SPSS software.
Conclusion
This study confirms the impact of hormones on incidence of malocclusion, BMI which in turn influences the caries index and could be used as an early predictor.
Biological marker, Caries risk susceptibility, 2D:4D ratio, Occlusal status, Obesity
Introduction
Malocclusion is an appreciable deviation from the ideal occlusion and may be considered aesthetically unsatisfactory [1] thus implying a condition of imbalance in the relative sizes and position of teeth, facial bones and soft tissues (lips, cheek and tongue). Malocclusion is neither an unhealthy nor normal condition which occurs in most [2] as at this state the teeth stay firm, function efficiently, do not change the position during and after their contact, do not cause pain and remain in good state of health [3]. The hormonal fingerprint which is the ratio of second and fourth digit lengths (2D:4D) is a new risk marker that has been used in the study to predict caries risk at a very early stage of life is found to be more stable, reproducible and consistent for each individual. Research confirms the impact of hormones on human physical and personality traits. The second to fourth digit ratio (2D:4D) is sexually differentiated in humans [4] as for humans, men tend to have lower 2D:4D than women, this sex effect is due to men’s greater relative length of the ring finger, in comparison with their index finger. The first mechanism explaining this sexual dimorphism is that the development of digits and gonads occur by the common genes Hox A and Hox D. The timing of gene regulation results in formation of a digit ratio which is constant throughout the life and also reflects the amount of androgen produced [5]. The second proposed mechanism is that finger ratio is a function of androgen sensitivity rather than androgen concentration. That is the two digit ratio affected by exposure to androgens e.g., testosterone while in the uterus, and that this 2D:4D ratio can be considered a crude measure for prenatal androgen exposure, with lower 2D:4D ratios pointing to higher prenatal androgen exposure [5]. These sex and individual differences in 2D:4D emerge in-utero at the beginning of the second trimester and seems to be fairly stable during postnatal life. This ratio will be helpful for assessing the action of prenatal sex hormone retrospectively on the brain, body and behaviour and for the prediction of malocclusion and caries risk for the individual [5].
Obesity and childhood overweight are becoming a major public health concern all over the world. Sedentary life style and altered dietary patterns have led to the development of obesity. Obesity appears to influence the general health as well as the oral health of an individual. Obesity is considered as a major risk factor in increased prevalence of hypertension, type 2 diabetes mellitus, accelerates dental development and decreases masticatory performance. Diet which is one of the etiological factors along with obesity which also has an equal importance in the caries process. There are conflicting reports in the literature regarding the association between BMI and dental caries [6].
The 2D:4D ratio which was established early in life was constant throughout the life of an individual. As it can be used as a marker for many diseases including CHD etc., these further lines of evidence have led to the proposal that 2D:4D might be useful as a retrospective, indirect marker for BMI, caries susceptibility and malocclusion and the current study was conducted with the aim of detecting relation between 2D:4D ratio and caries risk susceptibility and malocclusion. As obesity and childhood overweight were associated with many health related issues including dental problems [5]. This study was aimed to detect the relation between 2D:4D ratio and BMI also.
Materials and Methods
The present study was a retrospective type of study which was conducted on a group of 300 children of 10-15 years age group from both sexes who had attended the outpatient Department of Pedodontics and Preventive Dentistry, St. Joseph Dental College and Hospital, Eluru with good general health and no systemic illness or hospitalization. The study was conducted for a time period of six months. The Guardian/the Parents of the participants signed individual informed consent forms containing information about the aim of the study and the study procedures. The study was approved by the Ethical Committee of the Institution. Children with no systemic illness, healthy normal children with no physical or mental disability, children of age group–10 to15 years were included in the study and children with injuries or deformities of the hands, children with long-standing systemic illness, children who were on any medication within the past two months, children with physical or mental disability, children whose parents did not give consent were excluded from the study.
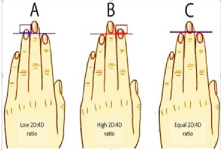
Calculation of 2D:4D ratio: [Table/Fig-1,2]
Illustration of three possible 2D:4D ratio outcomes [7].
Measurement of 2D:4D ratio.

The length of the Index (2D) and Ring (4D) fingers were measured for all the children from the ventral proximal crease of the digit to the tip. In the case there were multiple creases at the base of the digit, measurement taken from the most proximal of these creases with the help of digital Vernier’s caliper.
Calculation of Body Mass Index: Height and weight were measured for all those who are enrolled in the study. The weight of each child was measured in standing posture with equal distribution of mass between feet, to the nearest 0.1 kg using a Krups Imperial analogue weighing scale which was calibrated before use. Each child was instructed to stand still, with mass equally distributed between feet, until the scale reading stabilized. The reading was then recorded. Height was measured to the nearest 0.1cm using a stature meter attached to the wall in the department. For the calculation of BMI, the following formula was used.
BMI = Weight in kg/ height in m2
From the values obtained children were categorized as,
Underweight = <18.5
Normal weight = 18.5–24.9
Overweight = 25–29.9
Obesity = BMI of 30 or greater
Clinical Examination: Caries status (deft and DMFT) was recorded based on WHO standard criteria mentioned in the WHO oral health proforma, 1997 [8]. Two trained and calibrated examiners performed comprehensive clinical examination with the assistance of one recorder. The values of one investigator were cross examined by other investigator. Children were made to sit on the dental chair and examination was conducted under light attached to the dental chair. Sterile mouth mirrors, Community Periodontal Index (CPI) ballpoint probes. Caries was recorded as present when a lesion in a pit and a fissure or on a smooth surface had cavity with undermined enamel or smooth surface which may be arrested or active lesion. Recordings of the data were noted by a trained assistant. The occlusal characteristics including molar relation, anterior and posterior cross bite, open bite, deep bite, lower anterior crowding were also recorded.
All the data were tabulated and subjected to statistical analysis. Pearson’s correlation test, t-test and Chi-Square test were used for analysing the data in SPSS software.
Results
The entire study population was divided into children with 2D:4D ratio less than 1 and ≥1 based on the calculations of 2D:4D. Out of 300 children 78.6% were males and 71.2% were females with 2D:4D less than 1, 21.4% males and 28.8% females were having 2D:4D ≥1. Male population showed higher prevalence in the low 2D:4D ratio [Table/Fig-3].
Distribution of males and females in 2D:4D <1or ≥1.
| Sex | <12D:4D | % | ≥12D:4D | % | Total |
|---|
| Male | 121 | 78.57 | 33 | 21.43 | 154 |
| Female | 104 | 71.23 | 42 | 28.77 | 146 |
| Total | 225 | 75.00 | 75 | 25.00 | 300 |
2D:4D with Occlusion
The Pearson’s correlation test and chi-square test showed 2D:4D has significant positive correlation with occlusal status of the individual (p=0.0001) suggesting that higher the 2D:4D higher will be the occurrence of malocclusion [Table/Fig-4]. Children having Angles Class II, Class III molar relation, anterior and posterior cross bite and anterior crowding were considered as children with malocclusion. Either one or more of the above mentioned characteristics were considered under malocclusion. Among 300 children 147(49%) of them were identified with malocclusal characteristics. With increasing values of 2D:4D ratios children were identified with more number of malocclusal characteristics.
Comparison between 2D:4D ratio and malocclusion.
| Occlusion | <12D:4D | % | ≥12D:4D | % | Total |
|---|
| Normal | 113 | 73.86 | 40 | 26.14 | 153 |
| Malocclusion | 112 | 76.19 | 35 | 23.81 | 147 |
| Total | 225 | 75.00 | 75 | 25.00 | 300 |
Pearson Correlation = 0.657 chi square (p = 0.0001*)
2D:4D with BMI
• A significant negative correlation between 2D:4D ratio and BMI (p=0.0372) indicating higher BMI value associated with lower the 2D:4D [Table/Fig-5].
Comparison between 2D:4D ratio and BMI.
| Group | Mean | Standard Deviation | t-value | p-value |
|---|
| <1 2D:4D | 16.80 | 3.07 | -2.0926 | 0.0372* |
| ≥1 2D:4D | 17.66 | 3.15 | | |
*‘t’ test
BMI with occlusion
• BMI of the individual had significant negative correlation with occlusal status (p=0.041) reflecting malocclusal condition with lesser BMI [Table/Fig-6].
Comparison between BMI and malocclusion.
| BMI | N | % | M | % | Total |
|---|
| <18.5 | 120 | 81.63 | 108 | 70.59 | 228 |
| 18.5 – 25.0 | 23 | 15.65 | 39 | 25.49 | 62 |
| 25.0 – 30.0 | 4 | 2.72 | 6 | 3.92 | 10 |
| Total | 147 | 100.00 | 153 | 100.00 | 300 |
Pearson Correlation = -0.101 Chi-Square (p = 0.041)
DMFT with occlusion
• Higher caries experience seen with deviated occlusal condition with significant p value (p=0.027*) [Table/Fig-7].
Cross tabulation of mean and standard deviation of comparison between DMFT and malocclusion among study population.
| Mean | Std. Deviation | Number |
|---|
| Occlusion Grading | 1.49 | 0.501 | 300 |
| DMFT | 0.78 | 1.151 | 300 |
| p-value | 0.027* | | |
*‘t’ test
Discussion
As predicted, male mean 2D:4D was lower than female mean 2D:4D across nations and the effected size was greatest for the right hand. This indicates that men may have experienced higher levels of prenatal testosterone and lower levels of prenatal oestrogen than women. 2D: 4D ratio has been found as a reliable marker for prenatal testosterone which causes prolongation of 4th digit relative to the 2nd digit [1].
2D:4D ratio is sexually dimorphic. Our findings suggest that 2D:4D ratio was lower in males than females, which was in accordance with the Manning et al., [4]. The sexual dimorphism in 2D:4D ratio was also reported by Brown et al., [9]. The sexual dimorphism in digit ratio was explained by Lutchmaya et al., [10] who studied the relationships between 2D:4D ratios and Fetal Testosterone (FT) and Fetal Estrogen (FE) from amniotic fluid in a sample of 33 children. They reported significant negative associations between right 2D:4D ratio and FT/FE ratio – independent of sex – such that low 2D:4D was associated with higher levels of FT relative to FE, and high 2D:4D correlated with low FT relative to FE. They concluded that there is association between low 2D:4D and high levels of FT relative to FE, and high 2D:4D with low FT relative to FE [4,9,10].
The value of 2D:4D is lower in men and within each sex lower 2D:4D ratio points to the higher intrauterine androgen levels. Men with high sensitivity to the androgen receptors have lower (more masculine) 2D:4D ratio. 2D:4D ratio is stable and fixed in early life. There is no evidence that 2D:4D ratio changes with age [4]. Low 2D:4D digit ratio has been associated with high levels of androgens, whereas higher ratio is associated with high estrogen levels. The mean 2D:4D in the present study was 0.96 which was supported by Kangassalo et al., who concluded that the mean 2D:4D ratios of South Indian population was ranged between 0.96 -0.97, and they also noted the mean 2D:4D ratios of (Poland, Spain and England), (Zulus, Finns and Jamaican) populations as 0.99 to 1.00 and 0.93 to 0.96 respectively [11]. The 2D:4D ratio has been much spoken and discussed in the medical scenario, but not much information is available as far as dentistry is concerned [5]. The impact of human hormones (2D:4D ratio) on taste perception was explained by Verma et al., [5]. Thereby they explained the influence of 2D:4D ratio on caries index of the individuals with prevalence of more sweet likers in the low digit ratio category [5]. Lower 2D:4D ratio was associated with less malocclusion and higher dental caries was associated with more deviated occlusal characteristics according to the current study. Hence, it can be assumed that the individuals with higher 2D:4D ratio tends to have greater caries experience. Elangovan A reported that caries prevalence was more in obese children and caries scores were increasing with increased BMI for age. But the relation was not statistically significant [12] Begum MZ conducted a survey to evaluate the relation between BMI and dental caries and concluded that there was no relation between them [13]. According to Hooley et al., the higher caries incidence was associated with both high and low BMI values and stated that dental caries and BMI are related in a nonlinear fashion with more dental caries occurring in individuals with either higher or lower BMI [6]. Gupta P, Gupta N, Singh HP evaluated the prevalence of dental caries in relation to BMI in 12 year old school going children and the results showed that there was no significant correlation between them which was in accordance with the present study [14]. Malocclusion and BMI were inversely related in the present study which was supported by Stefan Van Dongen who reported that there is inverse relation between them [15]. Prevalence of malocclusion in the current study was 49% and a slightly higher value of 53.7% reported by Kumar P and co-workers [16]. However, further research to explore the impact of 2D:4D ratio and BMI on malocclusion as they are multifactorial in origin and necessitate exploration with larger sample size are necessary to confirm their practical applicability in paediatric dentistry.
Conclusion
The hormonal finger prints are new biological markers which can be used as predictors for the incidence of malocclusion as high 2D:4D ratio associated with high malocclusion and Lower BMI values. The present study confirms the impact of hormones on incidence of malocclusion, BMI which in turn influence the caries index and could be used as an early predictor for malocclusion and dental caries in children.
[1]. Houston WJB, Stephens CD, Tulley WJ, A Textbook of Orthodontics 1992 Great BritainWright:1-13. [Google Scholar]
[2]. Proffit WR, Fields HW, Contemporary Orthodontics 2000 ChicagoMosby Year Book:1-15. [Google Scholar]
[3]. Hassan R, Rahimah AK, Occlusion, malocclusion and method of measurements - an overviewArchives of Orofacial Sciences 2007 2:3-9. [Google Scholar]
[4]. Manning JT, Scutt D, Wilson J, Lewis-Jones DI, The ratio of 2nd to 4th digit length: A predictor of sperm numbers and concentrations of testosterone, luteinizing hormone and oestrogenHum Reprod 1998 13:3000-04. [Google Scholar]
[5]. Verma P, Hegde AM, Narayanacharyulu R, Hormonal fingerprints: a key to early diagnosis of cariesIndian J Dent Res 2013 24(6):674-77. [Google Scholar]
[6]. Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N, Body mass index and dental caries in children and adolescents: a systematic review of literature published 2004 to 2011Syst Rev 2012 21:1-57. [Google Scholar]
[7]. Glenn Lim, What does your finger say about you? [Internet]Glennlim thoughts 2015 [cited 2015 aug, 4] Available from Netlibrary: https://glennlimthots.wordpress.com/page/2/ [Google Scholar]
[8]. Oral Health Surveys-Basic Methods 1997 4th edGenevaWHOWHO [Google Scholar]
[9]. Brown W, Hines M, Fane B, Breedlove S, Masculinized finger length patterns in human males and females with congenital adrenal hyperplasiaHormones and Behavior 2002 42(4):380-86. [Google Scholar]
[10]. Lutchmaya S, Baron-Cohen S, Raggatt P, Knickmeyer R, Manning JT, 2nd to 4th digit ratios, fetal testosterone and estradiolEarly Human Development 2004 77:23-28. [Google Scholar]
[11]. Kangassalo K, Pölkki M, Rantala MJ, Prenatal influences on sexual orientation: digit ratio (2D:4D) and number of older siblingsEvol Psychol 2011 9(4):496-508. [Google Scholar]
[12]. Elangovan A, Mungara J, Joseph E, Exploring the relation between body mass index, diet, and dental caries among 6-12-year-old childrenJ Indian Soc Pedod Prev Dent 2012 30(4):293-300. [Google Scholar]
[13]. Begum MZ, Nagamalleshwari M, Srinivas P, Gadagi JS, Gadde P, Jyothirmai K, Is body mass index truly related to dental caries? Survey on predisposing factors for overweight among Indian school childrenJ Dent Hypotheses 2014 5(4):150-54. [Google Scholar]
[14]. Gupta P, Gupta N, Singh HP, Prevalence of dental caries in relation to body mass index, daily sugar intake, and oral hygiene status in 12-year-old school children in Mathura city: A pilot studyInt J Pediatr 2014; Feb 12 [Google Scholar]
[15]. Dongen S, Second to fourth digit ratio in relation to age, BMI and life history in a population of young adults: A set of unexpected resultsJournal of Negative Results 2009 6:1-7. [Google Scholar]
[16]. Kumar CP, Londhe BSM, Kotwal CA, Mitra CR, Prevalence and orthodontic treatment need in school children – An epidemiological studyMed J Armed Forces India 2013 69:369-74. [Google Scholar]